Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
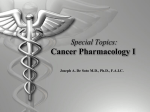
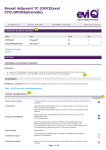
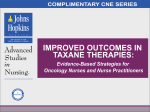
Breast Adjuvant TC (DOCEtaxel and CYCLOPHOSPHamide) ID: 000024 (V.2) Approved: 10 Nov 2007 Last Modified: 22 Jul 2014 Review Due: 30 Jun 2016 Treatment Schedule Summary Drug Dose Route Day DOCEtaxel 75 mg/m2 IV 1 CYCLOPHOSPHamide 600 mg/m2 IV 1 Frequency: 21 days Cycles: 4 Full View Indications and Patient Population Indications: ■ ■ stage I to III operable invasive breast cancer after complete surgical excision of the primary tumour may be considered for use in patients where an anthracycline is contraindicated Drug Status: Docetaxel: (PBS authority) Adjuvant treatment of operable breast cancer in combination with cyclophosphamide Cost: ~$165 per cycle (chemotherapy only) Clinical Information Tools/Links Venous access required IV cannula (IVC) or central venous access device (CVAD) is required to administer this treatment. Premedication Dexamethasone 8 mg TWICE a day for 3 consecutive days, commencing one day prior to docetaxel administration. Dexamethasone premedication helps to reduce the severity and frequency of fluid retention. Emetogenicity MODERATE Dexamethasone as per premedication then 8 mg daily for up to 3 days post chemotherapy AND Palonosetron IV 0.25 mg day 1. Ensure that patients have sufficient antiemetics for breakthrough emesis: Metoclopramide 10 mg to 20 mg every 4 to 6 hours when necessary OR Prochlorperazine 10 mg PO every 4 to 6 hours when necessary. Hypersensitivity High risk with docetaxel. Growth factor support G-CSF (filgrastim, lenograstim or pegfilgrastim) is available on the PBS for the secondary prevention of neutropenia. Peripheral neuropathy Assess prior to each cycle. If a patient experiences > grade 2 peripheral neuropathy, a dose reduction or delay of treatment may be required; review by medical officer before commencing treatment. Blood tests Baseline and repeat prior to each treatment FBC, EUC, LFTs. Nadir FBC cycle 1. Page 1 of 10 Breast Adjuvant TC (DOCEtaxel and CYCLOPHOSPHamide) Hepatitis B screening and prophylaxis Routine screening for HBsAg and anti-HBc is recommended prior to initiation of chemotherapy or immunosuppressive therapy for: haematology patients AND all patients with solid tumours receiving curative treatment. Screening is NOT routinely recommended for patients who are not being treated with curative intent, except those receiving immunosuppressive chemotherapy, high dose glucocorticoids or an anthracycline containing regimen. Vaccinations Live vaccines, including BCG, MMR, zoster and varicella vaccines, are contraindicated in cancer patients receiving immunosuppressive therapy and/or who have poorly controlled malignant disease. Refer to the recommended schedule of vaccination for oncology patients, as outlined in the 2013 Australian Immunisation Handbook 10th Edition. Effects of cancer treatment on fertility Information regarding the effects on fertility of cancer treatments. The supportive therapies included in the treatment schedule (antiemetics, premedications etc) are listed as defaults. These may be substituted to reflect individual institutional policy. Additionally, infusion times, diluents, volumes and routes of administration (as applicable) may vary between institutions. Treatment Schedule Drug list Cycle 1 to 4 Day 1 Palonosetron 0.25 mg (IV bolus) 30 minutes before chemotherapy Dexamethasone 8 mg (PO ) TWICE a day with or after food (to start the day before chemotherapy) DOCEtaxel 75 mg/m2 (IV infusion) in 250 mL to 500 mL sodium chloride 0.9% over 60 minutes CYCLOPHOSPHamide 600 mg/m2 (IV infusion) in 500 mL sodium chloride 0.9% over 30 to 60 minutes 8 mg (PO ) TWICE a day with or after food 8 mg (PO ) ONCE a day with or after food. May be continued up to Day 4 if required for the management of nausea. Day 2 Dexamethasone Day 3 Dexamethasone Frequency: 21 Days Cycles: 4 Dose Modifications There is limited evidence for dose modification and the recommendations made on eviQ are intended as a guide only. They are generally conservative, placing a greater weight on safety compared to efficacy. Link to Dosing Considerations & Disclaimer Note: All dose reductions are calculated as a percentage of the starting dose Haematological toxicity ANC x 109/L (on day of chemotherapy) 0.5 to less than 1.0 Delay treatment until recovery and consider adding G-CSF for subsequent cycles less than 0.5 Delay treatment until recovery and consider adding G-CSF for subsequent cycles; If patient is already on G-CSF, consider reducing docetaxel and cyclophosphamide by 25% for subsequent cycles Febrile neutropenia Delay treatment until recovery and consider adding GCSF for subsequent cycles; If patient is already on GCSF, consider reducing docetaxel and cyclophosphamide by Page 2 of 10 Breast Adjuvant TC (DOCEtaxel and CYCLOPHOSPHamide) 25% for subsequent cycles Platelets x109/L (at any stage of the cycle) 50 to less than 100 Delay treatment until recovery less than 50 Delay treatment until recovery and consider reducing docetaxel and cyclophosphamide by 25% for subsequent cycles Renal impairment Creatinine clearance (mL/min) 30 to 50 Reduce cyclophosphamide by 25% less than 30 Reduce cyclophosphamide by 50% Link to classification of renal dysfunction for dose modification Hepatic impairment Hepatic dysfunction Minimal Reduce docetaxel by 25% Mild Reduce docetaxel by 50% Moderate/Severe Omit docetaxel Link to classification of hepatic dysfunction for dose modification Peripheral neuropathy CTC grading Grade 2 which is present at the start of the next cycle Reduce docetaxel by 25%, if persists, reduce docetaxel by 50% Grade 3 or Grade 4 Omit docetaxel Mucositis & stomatitis CTC grading Grade 2 Delay treatment until toxicity has resolved to Grade 1 or less and reduce the dose for subsequent cycles as follow: 1st occurrence: No dose reduction 2nd occurrence: Reduce docetaxel and cyclophosphamide by 25% 3rd occurrence: Reduce docetaxel and cyclophosphamide by 50% 4th occurrence: Withhold chemotherapy Grade 3 or Grade 4 Delay treatment until toxicity has resolved to Grade 1 or less and reduce the dose for subsequent cycles as follow: 1st occurrence: Reduce docetaxel and cyclophosphamide by 50% 2nd occurrence: Withhold chemotherapy Diarrhoea CTC grading Grade 2 Delay treatment until toxicity has resolved to Grade 1 or less and reduce the dose for subsequent cycles as follow: 1st occurrence: No dose reduction 2nd occurrence: Reduce docetaxel and cyclophosphamide by 25% 3rd occurrence: Reduce docetaxel and cyclophosphamide by 50% Page 3 of 10 Breast Adjuvant TC (DOCEtaxel and CYCLOPHOSPHamide) 4th occurrence: Withhold chemotherapy Grade 3 or Grade 4 Delay treatment until toxicity has resolved to Grade 1 or less and reduce the dose for subsequent cycles as follow: 1st occurrence: Reduce docetaxel and cyclophosphamide by 50% 2nd occurrence: Withhold chemotherapy Interactions References & Disclaimer Cyclophosphamide Interaction Clinical management CYP3A4 inducers (e.g. carbamazepine, phenytoin, phenobarbitone, rifampicin, St John’s wort etc.) Increased toxicity of cyclophosphamide possible due to increased conversion to active (and inactive) metabolites Avoid combination or monitor for cyclophosphamide toxicity CYP3A4 inhibitors (e.g. aprepitant, azole antifungals, clarithromycin, erythromycin, grapefruit juice, ritonavir etc.) Reduced efficacy of cyclophosphamide possible due to decreased conversion to active (and inactive) metabolites Avoid combination or monitor for decreased clinical response to cyclophosphamide Amiodarone Possible additive pulmonary toxicity with high-dose cyclophosphamide (i.e. doses used prior to stem cell transplant; 60 mg/kg daily or 120 to 270 mg/kg over a few days) Avoid combination or monitor closely for pulmonary toxicity Allopurinol, hydrochlorothiazide, indapamide Delayed effect. Increased risk of bone marrow depression; probably due to reduced clearance of active metabolites of cyclophosphamide Avoid combination, consider alternative antihypertensive therapy or monitor for myelosuppression Cyclosporin Reduced efficacy of cyclosporin due to reduced serum concentration Monitor cyclosporin levels; adjust dosage as appropriate; monitor response to cyclosporin Suxamethonium Prolonged apnoea due to marked and persistent inhibition of cholinesterase by cyclophosphamide Alert the anaesthetist if a patient has been treated with cyclophosphamide within ten days of planned general anaesthesia Link to table of CYP inducers, inhibitors and substrates Docetaxel Interaction Clinical management CYP3A4 and P-gp inhibitors (e.g. amiodarone, aprepitant, azole-antifungals, ritonavir, lapatinib, nilotinib, sorafenib, macrolides, cyclosporin, grapefruit juice etc.) Increased toxicity of docetaxel possible due to reduced clearance Avoid combination or monitor for docetaxel toxicity CYP3A4 inducers (e.g. carbamazepine, phenytoin, phenobarbitone, rifampicin, St John’s wort etc.) Reduced efficacy of docetaxel possible due to increased clearance Avoid combination or monitor for decreased clinical response to docetaxel Link to table of CYP inducers, inhibitors and substrates General Interactions Interaction Warfarin Antineoplastic agents may alter the anticoagulant effect of warfarin Page 4 of 10 Clinical management Monitor INR regularly and adjust warfarin dosage as appropriate; consider alternative anticoagulant (e.g. LMWH, oral Factor Xa inhibitor, unfractionated heparin) Breast Adjuvant TC (DOCEtaxel and CYCLOPHOSPHamide) Digoxin Antineoplastic agents can damage the lining of the intestine; affecting the absorption of digoxin Monitor digoxin serum levels; adjust digoxin dosage as appropriate Antiepileptics Both altered antiepileptic and antineoplastic levels may occur, possibly leading to loss of efficacy or toxicity. Where concurrent use of an enzyme-inducing antiepileptic cannot be avoided, monitor antiepileptic serum levels for toxicity, as well as seizure frequency for efficacy; adjust dosage as appropriate Also monitor closely for efficacy of the antineoplastic therapy Antiplatelet agents and NSAIDs Increased risk of bleeding due to treatment related thrombocytopenia Avoid or minimise combination If combination deemed essential, (e.g. low dose aspirin for ischaemic heart disease) monitor for signs of bleeding Vaccines Diminished response to vaccines and increased risk of infection with live vaccines Live vaccines (e.g. BCG, MMR, zoster and varicella) are contraindicated For more information; refer to the recommended schedule of vaccination for oncology patients, as outlined in the 2013 Australian Immunisation Handbook 10th Edition. Administration Details Treatment time (~ 2.5 hours) General patient assessment prior to each day of treatment NOTE: Any toxicity greater than grade 2 may require dose reduction or delay of treatment and review by medical officer before commencing treatment. Prime IV lines Insert IV cannula or access Port, PICC or CVC Pre treatment medications Verify dexamethasone premedication has been taken Administer 5HT3 antagonist PO or by IV bolus over 3 to 5 minutes Chemotherapy Time out Docetaxel infusion Prior to administration The medicines information reference publications stipulate the use of nonPVC containing bags and administration sets. However, this is not consistently recommended in the product information, therefore the decision should be at the discretion of the administering unit. ■ ■ ■ assess for peripheral neuropathy prior to administration. Any toxicity grade 2 or above refer to medical officer assess patient for fluid retention or weight gain prior to each cycle ● notify medical officer of any signs of fluid retention or unexplained weight gain if using frozen gel gloves these need to be commenced ~ 15 minutes prior to administering the docetaxel Administer docetaxel (irritant with vesicant properties) over 60 minutes ■ ■ ■ via IV infusion observe for hypersensitivity reactions flush with ~ 100 mL of sodium chloride 0.9% NOTE: Continue with frozen gel gloves for ~ 15 minutes post completion of docetaxel Page 5 of 10 Breast Adjuvant TC (DOCEtaxel and CYCLOPHOSPHamide) Cyclophosphamide infusion Administer cyclophosphamide over 30 to 60 minutes ■ ■ via IV infusion flush with ~ 50 mL of sodium chloride 0.9% NOTE: Rapid infusion can cause dizziness, rhinitis, nausea and perioral numbness. If symptoms develop, slow infusion rate. Remove IV cannula and/or disconnect Port, PICC or CVC Continue safe handling precautions until 7 days after completion of drug(s) Discharge Information Premedication ■ dexamethasone tablets for next cycle of chemotherapy. Take home antiemetics ■ antiemetics as prescribed Growth factor support ■ arrangements for administration if prescribed Patient information ■ Patient Information Sheet Monitoring Test/Assessments Frequency Tools/Links Peripheral neuropathy Assess prior to each cycle. If a patient experiences > grade 2 a dose reduction or delay of treatment may be required; review by medical officer before commencing treatment. Blood tests Baseline and repeat prior to each treatment FBC, EUC, LFT. Nadir FBC cycle 1. Side Effects The side effects listed below are not a complete list of all possible side effects for this treatment. Side effects are categorised into the approximate onset of presentation and should only be used as a guide. Immediate (onset hours to days) Hypersensitivity Reaction Anaphylaxis and infusion related reaction. Nausea and Vomiting Treatment induced nausea and vomiting. Taste and Smell Alteration Changes in taste and smell can affect appetite and are a common side effect in patients receiving chemotherapy. Early (onset days to weeks) Neutropenia Low numbers of circulating neutrophils reduce the body's ability to fight infection. Any fever or suspicion of infection should be investigated immediately and managed aggressively. Thrombocytopenia A reduction in the number of circulating platelets increases the risk of bruising and bleeding. Oral Mucositis This is defined as chemotherapy induced damage to the oral mucosa which causes pain (ranging from mild soreness to severe ulceration associated with inability to eat or drink) and may become a portal for infection. This side effect focuses on oral mucositis; however mucositis can affect any mucous membrane. Arthralgia and Myalgia Generalised body aches and pains may occur a few days following treatment and last for several days. This may require moderately strong analgesia. Diarrhoea An increase in the frequency, or fluid content of stool. Page 6 of 10 Breast Adjuvant TC (DOCEtaxel and CYCLOPHOSPHamide) Fatigue Fatigue is a feeling of excessive tiredness or exhaustion for most or all of the time, typically not relieved by rest or sleep. Skin Rash Macular and Papular A disorder characterised by the presence of macules (flat) and papules (elevated lesions) and can be associated with pruritus Peripheral Neuropathy This is typically a symmetrical sensory neuropathy affecting the fingers and toes, and sometimes as treatment progresses may affect much of the hands and feet. Dosage adjustment, delay or cessation may be required. Hyperlacrimation Ocular symptoms include watery eyes, blepharitis, tear duct stenosis, acute and chronic conjunctivitis, photophobia, excessive lacrimation and drug excretion in tears. Fluid Retention Syndrome associated with Docetaxel 27% despite dexamethasone premedication (Jones et al 2006) Presents as peripheral oedema and weight gain and less frequently as pleural effusion and/or ascites. Incidence and severity appear to be related to cumulative dose and is caused by capillary leak. PalmarPlantar Erythrodysesthesia (PPE) Hand Foot Syndrome PalmarPlantar Erythrodysesthesia (PPE) also known as Hand Foot Syndrome (HFS) is characterized by the gradual onset of bilaterally symmetric erythema, tenderness, pain, swelling, tingling, numbness, pruritus, dry rash, or moist desquamation and ulceration over the palms and soles. Late (onset weeks to months) Anaemia Antineoplastic drugs can interfere with the reproduction of haematopoietic cells which results in a decreased production of red blood cell (RBC) precursors and mature RBCs. Alopecia is common and may include hair loss from all parts of the body. Cognitive Changes (chemo fog) Changes in cognition characterised by memory loss, forgetfulness and feeling vague during and after chemotherapy. Also referred to as 'chemo brain' or 'chemo fog'. Nail Changes severe nail changes can occur in 2% of patients having docetaxel Changes in the fingernail and toenails may be seen during chemotherapy. Nail changes include hyperpigmentation and damage to the epithelium under nails causing a change in the tight adhesion between the nail plate and nail bed which can lead to separation of the nail plate from the nail bed, causing pain. Physical and psychological effects can be significant. Delayed (onset months to years) Menopausal Symptoms Irregularity or cessation of menstrual periods due to ovarian failure may occur. This may be associated with menopausal symptoms such as hot flushes, mood swings, sleep disturbance, dyspareunia, night sweats, and a decrease in libido. Page 7 of 10 Breast Adjuvant TC (DOCEtaxel and CYCLOPHOSPHamide) Evidence The evidence supporting this treatment comes from a phase III randomised trial by Jones comparing the efficacy of doxorubicin and cyclophosphamide (AC) to docetaxel and cyclophosphamide (TC)1, 2 Between June 1997 and December 1999, 1016 patients were randomly assigned to receive 4 cycles of the above regimens every 3 weeks as adjuvant therapy. Both treatment groups were well balanced with respect to major prognostic factors for breast cancer outcome. The primary end point was diseasefree survival (DFS) and secondary endpoints included overall survival (OS). Efficacy At a median of 7 yrs followup the the difference in DFS between TC and AC was significant (81% TC v 75% AC; P=.033; hazard ratio [HR], 0.74; 95% CI 0.56 to 0.98) as was OS (87% TC v 82% AC; P=.032; HR, 0.69; 95% CI, 0.50 to 0.97). Disease Free Survival2 Overall Survival2 © Journal of Clinical Oncology 2009 Toxicity The TC group experienced significantly more grade 1 and 2 oedema, myalgia and arthralgia (p< 0.01) whereas in the AC group, patients had more grade 1 to 4 nausea and vomiting (p<0.01). In the AC group, 1 patient died from congestive heart failure and 4 patients died from myocardial infarction. In the TC group, no case of congestive heart failure was observed but 2 patients died from myocardial infarction. There was more febrile neutropenia observed with TC compared with AC (5% vs 2.5%; p=0.07). 2 patients died while receiving TC (one unrelated cardiac death and one death with sepsis and neutropenia). No patients died during treatment with AC. Frequency of Reported Adverse Events all Grades at Median Followup of 5.5 yrs1 TC (n=506) % AC (n=510) % Grade 1 & 2 Grade 3 &4 Grade 1 & 2 Grade 3 &4 Anaemia 5 <1 7 1 Neutropenia 1 61 3 55 Thrombocytopenia <1 <1 <1 1 Asthenia 75 4 73 5 Oedema 34 <1 20 <1 Fever 19 5 15 3 Page 8 of 10 Breast Adjuvant TC (DOCEtaxel and CYCLOPHOSPHamide) Infection 12 7 12 8 Myalgia 32 1 16 <1 Nausea 51 2 75 7 Phlebitis 11 <1 2 0 Stomatitis 33 <1 44 2 Vomiting 14 <1 37 5 This paper has been used as the reference for the side effects of TC in the adjuvant setting as the key study trial 9735 did not capture all the well known side effects of docetaxel 3 Non Haematological Toxicity3 © Japanese Journal of Clinical Oncology 2009 References 1. 2. 3. Jones, S. E., M. A. Savin, F. A. Holmes, et al. 2006. "Phase III trial comparing doxorubicin plus cyclophosphamide with docetaxel plus cyclophosphamide as adjuvant therapy for operable breast cancer." J Clin Oncol. 24 (34):53815387. Jones, S., F. A. Holmes, J. O'Shaughnessy, et al. 2009. "Docetaxel With Cyclophosphamide Is Associated With an Overall Survival Benefit Compared With Doxorubicin and Cyclophosphamide: 7Year FollowUp of US Oncology Research Trial 9735." J Clin Oncol 27(8):11771183. Takabatake, D., N. Taira, F. Hara, et al. 2009. "Feasibility study of docetaxel with cyclophosphamide as adjuvant chemotherapy for Japanese breast cancer patients." Jpn J Clin Oncol 39(8):478483. Support & Information Services For telephone support Page 9 of 10 Breast Adjuvant TC (DOCEtaxel and CYCLOPHOSPHamide) ■ Cancer Council Helpline Phone 13 11 20 For online support ■ Cancer Connections www.cancerconnections.com.au For further information ■ ■ ■ ■ ■ ■ ■ ■ eviQ Cancer Treatments online www.eviQ.org.au Cancer Council Australia www.cancer.org.au Cancer Council NSW www.cancercouncil.com.au Food Standards Australia New Zealand Listeria & Food Safety (at www.foodstandards.gov.au/consumer/safety/listeria/pages/listeriabrochuretext.aspx) Cancer Australia www.canceraustralia.gov.au/affectedcancer/cancertypes/breastcancer Breast Cancer Network Australia www.bcna.org.au Westmead Breast Cancer Institute www.bci.org.au Australasian Menopause Society www.menopause.org.au For patient advocacy ■ Cancer Voices NSW www.cancervoices.org.au For support for young people living with cancer (1224 years): ■ ■ Canteen www.canteen.org.au NOWWHAT www.nowwhat.org.au For free workshops on caring for your hair and skin while on treatment ■ Look Good Feel Better www.lgfb.org.au The currency of this information is guaranteed only up until the date of printing, for any updates please check www.eviq.org.au 31 Oct 2014 Page 10 of 10