Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
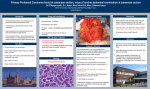
review articles IMAGING EVALUATION OF PRIMARY AND SECONDARY PERITONEAL MALIGNANCIES Evaluación por imágenes de las neoplasias peritoneales primarias y secundarias Catalina Wilches, MD1 Oscar M. Rivero, MD2 Diego A. Aguirre, MD2 Key words (MeSH) Peritoneum, peritoneal neoplasm, CT-scan SUMMARY This article is a review of the normal peritoneal anatomy as seen on different cross sectional imaging modalities.The definitions and demographic and imaging characteristics of primary and secondary malignancies involving the peritoneum are discussed for the appropriate assessment of patients with suspected peritoneal pathology. Introduction Resident IVth year of Radiology and Diagnostic Imaging. Hospital Universitario Fundación Santa Fe de Bogotá. Bogotá, Colombia. 2 Institutional Radiologist. Body Imaging Department. Hospital Universitario Fundación Santa Fe de Bogotá. Bogotá, Colombia. 1 Rev Colomb Radiol. 2010; 21:(3):1-11 The purpose of this article is to review the basic anatomy of the peritoneum using cross section diagnostic images and its pathological implications, in addition to describing the most frequent peritoneal malignancies. Just as in other anatomical locations, neoplastic peritoneal processes are divided into: primary (these occur rarely) and secondary. The peritoneum is a usual route for the dissemination of intra-abdominal malignancies including the most frequent GI tract pathology, as well as ovarian cancer, lung and breast cancer and melanoma. The clinical presentation is unspecific. The patient presents abdominal pain and bloating, palpable masses and ascites. Unfortunately, most patients are in advanced stages of the disease at the time of diagnosis, usually with diffuse peritoneal neoplastic involvement. There are multiple diagnostic imaging modalities for evaluating the condition. Multi-slice CT scan delivers the best anatomic resolution; MRI provides good soft tissue contrast and better anatomical resolution; positron emission tomography (PET) is not widely available in our environment but it enables staging and restaging, as well as the possibility to differentiate between tumor relapse vs. post-surgical changes. Ultrasound plays a limited role in the assessment of these pathologies but allows for the identification of ascites with retroperitoneal implants and peritoneal pseudomixoma. Breakthroughs in CT scan allow for fine slices and multiplanar reconstructions. The CT scanner using fine abdomen and pelvic slices identifies sub-centimeter implants and renders 3-D images with less artifacts and adequate evaluation of structures like the diaphragm, parietocolic gutters, the intestine and the posterior cul-de-sac. Anatomy of the Peritoneum The peritoneum is a serous membrane covered by a single layer of mesothelial cells that coats the complete abdomen. The peritoneal spaces are potential spaces not usually visualized unless they are distended by fluid or when there is thickening of the surrounding fascia. The abdomen can be divided into supracolic, infracolic, pericolic and pelvic spaces. The supra 1 and infracolic spaces are divided by the transverse colon and the mesenterium. In front the greater epiplon is located between the peritoneal wall and the intestine (1). The supracolic space includes the perihepatic spaces and the transcavity of the omenta. The mesenteric root extends right to left from the ligament of Treitz to the ilieocecal area, separating the infracolic space into the right and left spaces. On the outside, the pericolonic folds are communicated with the perihepatic spaces and the pelvic region (1) Figs. 1 & 2). Usually there are less than 50 mL of sterile fluid inside the cavity. This fluid is secreted by the visceral surface of the peri- toneum and, similar to lymph, with less than 3,000 ce ls/mm3 and low protein content. Inside the peritoneal cavity, the movement of fluid is caused by the negative pressure area in the subphrenic space, due to the movement of the diaphragm. By injecting fluid in the paracecal region, the fluid migrates initially into the subphrenic space and the pelvis; then it goes to the parietocolic gutter and the subhepatic spaces. The fluid absorption in the peritoneum basically takes place through the lymphatic circulation of the parietal peritoneum. There is also fluid absorption at the diaphragmatic lymphatics, b a a a b a b d c e f e Fig. 1 ab. Anatomy of the peritoneum. Right peritoneal space: a) perihepatic; f) lesser sac. Left peritoneal space: b) anterior perihepatic; c) posterior perihepatic; d) anterior subphrenic; e) posterior subphrenic. b a c est f f a f e Fig. 2. Anatomy of the peritoneum. Right peritoneal space: a) perihepatic; f) lesser sac. Left peritoneal space: b) anterior perihepatic; c) posterior perihepatic; d) anterior subphrenic; e) posterior subphrenic. Est = stomach. 2 Imaging evaluation of primary and secondary peritoneal malignancies, Wilches C, Rivero OM, Aguirre DA review articles which are in turn responsible for transporting microorganisms, cells and other particles present in the peritoneal fluid (2). The peritoneum that covers the muscle portion of the diaphragm has intercellular gaps called stomata, which are located between the mesothelial cells. Their size ranges between 4 to 12 microns, depending on the diaphragm’s stretching and contraction. When inflammation occurs, the fluid and the substances that cannot be absorbed by the peritoneal membrane are transported by the stomata through fenestrations of the basement membrane into specialized diaphragmatic lymphatic structures called lacunae. The relaxation of the diaphragm during expiration opens the stomata and promotes rapid filling of the lacunae. During inspiration, the contraction of the diaphragm empties the lacunae into the efferent lymphatic channels and passing to the central circulation via the thoracic duct (3, 4). It has been found in animal models that after injecting bacteria into the peritoneal cavity, these bacteria disappear immediately to be found 6 minutes later in the mediastinum and 12 minutes later in the blood stream. It has been determined as well that the stomata may get clogged with particles such as platelets or talcum powder. a Then we will discuss the major peritoneal primary and secondary neoplasms, their image presentation and the key diagnostic factors. Primary Peritoneal Neoplasms Malignant Peritoneal Mesothelioma Malignant mesotheliomas are a rare condition with high mortality rates (5-12 months in untreated patients) (5-7). Usually it affects 50 to 60 year old males, but it may occur at any age (7,8). This condition is found to be associated to asbestos exposure (6,8,9). There are two types of MPM: the diffuse type that behaves as an infiltrating tumor, associated with irregular and nodular thickening of the peritoneum and ascites (10,11); the focal type presents itself as a heterogeneous mass with heterogeneous contrast enhancement. Contrary to pleural mesothelioma, calcified plaques are unusual in the peritoneal mesothelioma (12). The CT findings are soft tissue masses, nodes, thickened peritoneum, ascites or local invasion of the intestine, the pancreas, and the liver (13, 14) (Fig.3). b Fig. 3 a,b. Malignant mesothelioma. Axial CT images with evidence of diffuse and nodular thickening of the peritoneum, with associated ascites. Liposarcoma The liposarcoma is a very frequent tumor of the retroperitoneum and relatively rare in the mesenterium and the peritoneum (15, 16). There are several histological types of which the myxoid is the most common. This condition does not differentiate between genders or typical age of presentation (17). Both the CT scan and the MRI show a soft tissue mass with an adipose component in 40% of the cases. Finding an atypical lipoma in the images may assist in making a differential diagnosis; i.e., an adipose mass with additional characteristics that rule out the diagnosis of lipoma, including: irregular septa or solid nodes inside (17) (Fig.4). Rev Colomb Radiol. 2010; 21:(3):1-11 Leiomiosarcoma This is a very vascularized tumor. It shows up in the images as a heterogeneous mass with areas or necrosis and cystic formations (Fig. 5) that may cause fistulae and perforate towards the intestinal lumen or the peritoneal cavity (18-20). The level of necrosis correlates to the histological grade of the tumor (21). There is no ascites and adenomegaly is rare (21-23). Leiomiosarcomas have a high rate of local recurrence with metastases to the liver and lungs (22,24). 3 a b Fig. 4a. Liposarcoma. Axial CT showing a peritoneal mass with adipose component and associated septa (atypical lipoma presentation). (b) Retroperitoneal, solid, heterogeneous mass with no evidence of fatty component inside. a b Fig. 5 a.b. Leiomiosarcoma. Axial and coronal plane CT scan images depicting a solid and heterogeneous peritoneal mass with lower density areas inside. This is consistent with the confirmed histological diagnosis of leiomiosarcoma. Peritoneal Sarcoma Peritoneal sarcomas are rare tumors with an incidence of 0.2% among the general population. They represent 50% of the primary mesenteric malignancies and their appearance in images depends on the histological type: liposarcoma, leiomiosarcoma, malignant fibrous histiocitoma or fibrosarcoma, which are far less frequent than in the retroperitoneum (25). The CT usually depicts them as large single masses (26) (Fig. 6 a,b,), frequently infiltrating and poorly defined. Peritoneal Lymphoma The involvement of the peritoneum in lymphoma usually occurs in young patients with a classical palpable abdominal 4 mass. The CT shows a group of lymph nodes around the aorta and the inferior vena cava that does not compress the vascular structures (27). Following the administration of FDG, the PET images depict hypermetabolic nodes (Fig. 7 a.b.). Primary Benign Peritoneal Neoplasms Lipoma The peritoneal lipoma is a benign tumor originating at the sub peritoneal fatty tissue. Usually is an incidental finding (26). The images show a fatty attenuation mass without soft tissue involvement (26,28) (Fig. 8). Imaging evaluation of primary and secondary peritoneal malignancies, Wilches C, Rivero OM, Aguirre DA review articles b a Fig. 6 a, b. Peritoneal sarcoma. Axial and coronal TC image showing a solid peritoneal irregular and heterogeneous mass, consistent with a confirmed histological diagnosis of sarcoma. Additionally, the fat density caudal to the lesion is altered. a b Fig. 7 a.b. Peritoneal lymphoma. CT and PET-CT axial views depicting focal peritoneal hypermetabolic lesions consistent with Hodgkin lymphoma. Rev Colomb Radiol. 2010; 21:(3):1-11 5 a b Fig. 8 a,b. Peritoneal lipoma. CT and MRI axial view (T1 weighted image) showing a fatty mass that thins out and bulges the posterior right abdominal wall (lumbar region). These findings are consistent with the presence of lipoma. Hemangioma The cavernous hemangioma is the most common hemangioma in the peritoneum, characterized by large pools of blood surrounded by endothelium and blurred margins. It may look like a hypo-dense heterogeneous mass (Fig 9 a,b,). The presence of phleboliths in its images is diagnostic (26). Other less common variants are the capillary and the venous hemangiomas (29). a Ganglioneuroma These peritoneal masses are more frequent in type 1 rather than type 2 neurofibromatosis. The TC evidences a multifocal, low attenuation mass (Fig, 10a), branching out or coalescent, that may mimic adenomegaly (26,30). This tumor has a heterogeneous enhancement with contrast media (Fig. 10b) and may occasionally show a cystic appearance. b Fig. 9 a,b. Hemangioma. Axial CT showing a solid irregular, heterogeneous and hypodense mass, consistent with the histological diagnosis of hemangioma. Diffuse Peritoneal Leiomiomatosis This is usually an incidental finding in reproductive age women and it is associated with high estrogen levels; i.e., during pregnancy or contraceptive use (26,31). The CT depicts multiple well-defined masses with a myomalike enhancement. The MRI T1-weighted images show as isointense muscle masses; contrast media enhancement is variable and T2-weighted images give a low signal (26) (Fig.11a-c). 6 Secondary Peritoneal Neoplasms Peritoneal Pseudomixoma This is a clinical entity that involves the peritoneal surfaces and the omentum. It is characterized by the intraperitoneal accumulation of gelatin-like material produced by the rupture of secondary cystic mucin-producing lesions or by primary mucinous cystadenocarcinoma-like lesions; mostly the cecal Imaging evaluation of primary and secondary peritoneal malignancies, Wilches C, Rivero OM, Aguirre DA review articles a b Fig. 10 a,b. Ganglioneuroma. CT axial views evidencing a solid mass and heterogeneous enhancement than can be due to a ganglioneuroma, with histological diagnosis. a b c Fig. 11. Diffuse peritoneal leiomiomatosis in pregnant patient (*) with intermediate signal diffuse peritoneal malignancy in different sequences. (a) Axial T1-weighted MRI images; (b) T2-weighted coronal images; (c) Axial post-contrast MRI evidencing diffuse enhancement of the peritoneal neoplastic involvement. Rev Colomb Radiol. 2010; 21:(3):1-11 7 or ovarian appendix and less frequently the uterine, urachal or omphalomesenteric appendix (32). Diagnostic images show a multicystic thick-walled mass or ascites with septa inside and curvilinear or punctuated calcifications (Fig. 12 a,b) (32). b a Fig. 12. Peritoneal Pseudomixoma. (a) Axial view. (b). Coronal CT with evidence of ascites with septa inside and contrast enhancement. Peritoneal Carninomatosis The term peritoneal carcinomatosis refers to the presence of soft-tissue implants over the peritoneal surface (omental cake). These implants originate in a primary tumor; usually breast, stomach, colorectal, pancreatic or ovarian cancer. When associated with peritoneal carcinomatosis, ovarian cancer is usually in an advanced stage, caused by the circulation of peritoneal fluid as previously described. Tumor implants vary in size and can be found from the diaphragm down to the pelvis (33), The abdomen and the pelvis are evaluated to stage the neoplasms, focusing mainly on the sites that are surgically difficult to assess: the diaphragm, the splenic helium, the stomach, the lesser sac, the liver, the root of the mesenterium and the paraaortic nodes above the renal vessels (34, 35). Detecting these lesions is of clinical value because clinical parameters and CT information are used for cancer staging and to predict the surgical outcome (36). Adequate tumor resection is achieved when there is evidence of residual disease >1 cm in diameter. Images are also useful 8 to determine whether the patient is a candidate for neoadjuvant chemotherapy prior to surgery. The diagnostic images show evidence of thickened lymph nodes of the peritoneum and peritoneal enhancement with contrast, associated with loculated ascites (37-40) (Fig. 13). The most salient non-malignant entities to consider for differential diagnosis are: granulomatous pathologies such as TB and less often, peritoneal histoplasmosis. Although the imaging characteristics are alike, there are some findings such as mesenteric macronodules, omental irregularity, spleen calcifications and splenomegaly that enable the diagnosis of TB (41.43). Peritoneal Metastases The peritoneum is the target of multiple metastatic processes, including the GI tract, GIST (gastrointestinal stromal tumor), the ovary (Fig 14 a,b), the breast, the lung and melanoma (44). CT and MRI are used for staging and evaluation of tumor relapses with peritoneal involvement. The PET-CT is particularly useful in those cases in which CT and MRI are negative and tumor markers are high (45). Imaging evaluation of primary and secondary peritoneal malignancies, Wilches C, Rivero OM, Aguirre DA review articles b a Fig. 13 a,b. Peritoneal carcinomatosis. Axial CT images. Different patterns of carcinomatosis can be identified due to the presence nodular soft tissue lesions and associated ascites. b a Fig. 14 a,b. Axial PET-CT images in two patients with a diagnosis of ovarian carcinoma. The images depict focal hypermetabolic solid nodular lesions. It is important to keep in mind that since 18-fluorodeoxiglucose (18 FGD) is mainly cleared through the urine, the kidneys, the ureters and the bladder have an increased uptake. Likewise, the intestine increased uptake is normal because of its own physiological activity but this should not be mistaken by hyper-uptake foci secondary to malignancy. Furthermore, benign conditions involving the intestine, such as duodenal ulcers, colon polyps, intestinal inflammatory disease or diverticulitis, among others, present 18 FDG hyper-uptake (46, 47). GIST (Gastro-Intestinal Stromal Tumor) The primary tumor is characterized by its exophytic submucosal mass appearance in the GI tract, mostly present in the stomach and the small gut. It may exhibit a hypovascular or hypervascular behavior. 25% of the cases show calcifications, necrosis (42,44,48). The PET image depicts a hypermetabolic mass (Fig. 15 a,b). This modality is more sensitive than the CT scan to assess treatment response (45,49). Rev Colomb Radiol. 2010; 21:(3):1-11 Krukenberg Tumor The Krukenberg tumor is a metastatic tumor of a primary adenocarcinoma that involves the ovary and contains mucinsecreting cells in the signet-ring; usually it originates in the breast or the GI tract, but mainly in the stomach (50,51). This tumor presents specific imaging characteristics including complex bilateral masses with a solid component (dense stromal reaction) and internal hyperintensity (mucin) in T1 and T2 (52,53). Conclusion Peritoneal neoplastic pathology occurs in different clinical scenarios and having an adequate knowledge of the anatomy, the pathophysiology and the appearance on diagnostic images is crucial for a correct interpretation. CT is the method of choice to assess this pathology and it is a useful guide to biopsy those masses. MRI is an alternate diagnostic modality, more costly, does not generate any ionizing radiation and is a good tool for 9 b a Fig. 15 a,b. GIST. Axial and coronal PET CT image showing a hypermetabolic mass in the upper left quadrant of the abdomen, consistent with proliferative deposit secondary to GIST. those cases in which CT is contraindicated. PET is extremely helpful for staging, follow-up and to differentiate between local relapse and surgical changes. References 1. Haaga J, Lanzieri Ch, Gilkeson R. TC y RM diagnóstico por imagen del cuerpo humano. Volumen 2. Elsevier. Cuarta edición. 2. Andrade A., Mejía A. Manejo de abdomen abierto: nuevo concepto en cirugía abdominal. Departamento de Cirugía. Pontificia Universidad Javeriana. Available in: http://med.javeriana.edu.co/ publi/vniversitas/. 3. Wang N. The performed stomas connecting the pleural cavity and the lymphatics in the parietal pleura. Am Rev Respir Dis, 1975. 4. Zinner M. Maingot’s abdominal operations. Stamford, CT.: Appleton & Lange, 1997. 5. Loggie BW, Fleming RA, McQuellon RP, Russell GB, Geisinger KR, Levine EA. Prospective trial for the treatment of malignant peritoneal mesothelioma. Am Surg 2001;67:999-1003. 6. Busch J., Kruskal J., Wu B. Best Cases from the AFIP Malignant Peritoneal Mesothelioma. RadioGraphics 2002;22:1511-15. 7. Tandar A, Abraham G, Gurka J, Wendel M, Stolbach L. Recurrent peritoneal mesothelioma with long-delayed recurrence. J Clin Gastroenterol 2001;33:247-50. 8. Wagner JC, Sleggs CA, Marchand P. Diffuse pleural mesothelioma and asbestos exposure in the North Western Cape Province (South Africa). Br J Ind Med 1960;17:260. 9. Antman KH. Presentation and natural history of benign and malignant mesothelioma. Semin Oncol I 981 8:313-20. 10 10.Antman KH. Current Concepts. Malignant mesothelioma. NEngi J Med 1980;303:200-202 8:313-20. 11. Whitley N, Brenner D., Antman K., Grant D., et al. CT of Peritoneal Mesothelioma: Analysis of Eight Cases. AJR 138:531 -535, March 1982. 12.Park J., Won Kim K., Kwon et al.Peritoneal Mesotheliomas: Clinicopathologic Features, CT Findings, and Differential Diagnosis. AJR 2008;191:814-825. 13.Reuter K., Raptopoulos V.,ReaIe F. Diagnosis of Peritoneal Mesothelioma: Computed Tomography, Sonography, and FineNeedle Aspiration Biopsy. AJR 140:1189-1194, June 1983. 14.Lazarus H., Widrich W.,Robbins A. Peritoneal mesothelioma with Roentgenographic findings. Volumen 113 Número 1. Boston University School of Medicine, Boston VA Hospital, Boston, Massachusetts. 15.Dach J., Patel N., Patel S., et al. Peritoneal Mesothelioma: CT, Sonography, and Gallium-67 Scan. AJR 1980;135:614-616. 16.Yeh H., Chahlnlan P. Ultrasonography and Computed Tomography of Peritoneal Mesothelioma. Radiology 1980;135:705-712. 17.Banner M., Gohel V. Peritoneal mesothelioma. Radiology, 1979;129, 637-40. 18.Evans HL. Liposarcomas and atypical lipomatous tumors: a study of 66 cases followed for a minimum of 10 years. Surg Pathol 1988;1:41-54. 19.Moyama TN. Primary mesenteric liposarcoma. Am J 1988;83:89-92. 20.Tonsok K., Takamichi M., Hiromichi 0. CT and MR Imaging of Abdominal Liposarcoma. AJR 1996;166:829-833. 21.Ranched M, Kempson AL. Smooth muscle tumors of the gastrointestinal tract and retroperitoneum: a pathological analysis of 100 cases. Cancer 1977;39:255-263. Imaging evaluation of primary and secondary peritoneal malignancies, Wilches C, Rivero OM, Aguirre DA review articles 22.Scatarige JC, Fishman EK, Jones B, Cameron JL, Sanders RC. Siegelman. Gastric leiomyosarcoma: CT observation. J Comput Assist Tomogr 1985;9:320-327. 23.Zornoza J, Shirkhoda A. Leiomyosarcoma: computed tomographic findings. Radiology 1984;152:133-136. 24.Byung Ihn Ch., Won Jae L., Je G Ch. CT Manifestations of Peritoneal Leiomyosarcomatosis. AJR 1990;155:799-801. 25.McLeod AJ, Zornoza J, Shirkhoda A. Leiomyosarcoma: computed tomegraphic findings. Radiology 1984;152:133-36. 26.Clark RA, Alexander ES. Computed tomography of gastrointestinal leiomyosarcoma. Gastrointest Radiol 1982;7:127-9. 27.Rha S., Ha H., Kim A., et al. Peritoneal Leiomyosarcomatosis Originating from Gastrointestinal Leiomyosarcomas: CT Features. Radiology 2003;227:385-90. 28.Hamrick-Turner JE, Chiechi MV, Abbitt PL, Ros PR. Neoplastic and inflammatory processes of the peritoneum, omentum, and mesentery: diagnosis with CT. RadioGraphics 1992;12:1051-68. 29.Pickhardt P., Bhalla S. Primary Neoplasms of Peritoneal and Subperitoneal Origin: CT Findings. RadioGraphics 2005;25:98395. 30.Lynch M, Cho K, Jeffrey, Jr. R, et al. CT of Peritoneal Lymphomatosis. AJR 15i:713-715,October 1988. 31.Sato M, Ishida H, Konno K, et al. Mesenteric lipoma: report of a case with emphasis on US findings.Eur Radiol 2002;12:793-95. 32.Varma JD, Hill MC, Harvey LAC. Hemangioma of the small intestine manifesting as gastrointestinal bleeding. RadioGraphics 1998;18:1029-33. 33.Pannu H, Bristow R, Montz F, Fishman E. Multidetector CT of Peritoneal Carcinomatosis from Ovarian Cancer. RadioGraphics 2003;23:687-701. 34.Bristow RE, Duska LR, Lambrou NC, et al. A model for predicting surgical outcome in patients with advanced ovarian carcinoma using computed tomography. Cancer 2000;89:1532-40. 35.Forstner R, Chen M, Hricak H. Imaging of ovarian cancer. J Magn Reson Imaging 1995;5:606-613. 36.Jeong YY, Outwater EK, Kang HK. Imaging evaluation of ovarian masses. RadioGraphics 2000;20:1445-70. 37.Matsuki K, Kakitsubata Y, Watanabe K, Tsukino H, Nakajima K. Mesenteric plexiform neurofibroma associated with Recklinghausen’s disease. Pediatr Radiol 1997;27:255-6. 38.Papadatos D, Taourel P, Bret PM. CT of leiomyomatosis peritonealis disseminata mimicking peritoneal carcinomatosis. AJR Am J Roentgenol 1996;167:475-6. 39.Seshul M., Coulam C. Pseudomyxoma Peritonei: Computed Tomography and Sonography. AJR 1981;136:803-6. 40.Goerg C., Schwerk W. Peritoneal Carcinomatosis with Ascitis. AJR 1991;156:1185-7. 41.Walkey M., Friedman A., Sohotra P., et al. CT Manifestations of Peritoneal Carcinomatosis. AJR 1988;150:1035-41. 42.Epstein BM, Mann JH. CT of abdominal tuberculosis. AJR 1982;139:881-6. 43.Nelson R., Chezmar J., Hoel M., et al. Peritoneal Carcinomatosis: Preoperative CT with Intraperitoneal Contrast Material. Radiology 1992;182:133-8. Rev Colomb Radiol. 2010; 21:(3):1-11 44.Ha H., Jung J., Lee M., et al. CT Differentiation of Tuberculous Peritonitis and Peritoneal Carcinomatosis. AJR 1996;167:743-8. 45.Cho SM, Ha HK, Byun JY, et al. Usefulness of FDG PET for assessment of early recurrent epithelial ovarian cancer. AJR Am J Roentgenol 2002;179:391-5. 46.Conti P., Cham D. PET-CT A Case-Based Approach. 2005 Springer Science+Business Media, Inc. 47.Coakley F., Choi P., Gougoutas C., et al. Peritoneal Metastases: Detection with Spiral CT in Patients with Ovarian Cancer. Radiology 2002;223:495-9. 48.Levy A, Remotti H, Thompson W, et al. Gastrointestinal Stromal Tumors: Radiologic Features with Pathologic Correlation. RadioGraphics 2003;23:283-304. 49.Sharp R, Ansel H, Keel S. Best cases from the AFIP: gastrointestinal stromal tumor. RadioGraphics 2001;21:1557-60. 50.Pannu H., Bristow R., Cohade C., et al. PET-CT in Recurrent Ovarian Cancer: Initial Observations. RadioGraphics 2004;24:209-23. 51.Ha HK, Baek SY, Kim SH, Kim HH, Chung EC, Yeon KM. Krukenberg’s tumor of the ovary: MR imaging features. AJR 1995;164:1435-9. 52.Jung S., Lee J., Rha S. CT and MR Imaging of Ovarian Tumors with Emphasis on Differential Diagnosis. 2010;30:118-22. 53.Brown DL, Zou KH, Tempany CM, et al. Primary versus secondary ovarian malignancy: imaging findings of adnexal masses in the Radiology Diagnostic Oncology Group Study. Radiology 2001;219:213-18. Correspondence Catalina Wilches Departamento de Radiología Fundación Santa Fe Calle 119 # 7 -75 Bogotá, Colombia [email protected]. Recived: June 28th, 2010 Accepted: July 26th, 2010 11