* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Scaling and root planing wikipedia , lookup
Tooth whitening wikipedia , lookup
Periodontal disease wikipedia , lookup
Dentures wikipedia , lookup
Dental implant wikipedia , lookup
Dental emergency wikipedia , lookup
Impacted wisdom teeth wikipedia , lookup
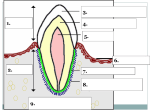
Dental anatomy wikipedia , lookup