Survey
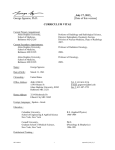
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Investigations and research Molecular imaging for visualization and quantification of individualized targeted cancer therapy M. Lubberink S.N.F. Rizvi O.S. Hoekstra G.A.M.S. van Dongen Targeted therapy and imaging Recent advances in molecular biology have facilitated the identification of molecular targets on tumor cells, such as those involved in proliferation, differentiation, apoptosis, and angiogenesis. This has boosted the design of targeted pharmaceuticals, with monoclonal antibodies (MAbs) forming the largest category. Examples of MAbs used in targeted therapy include: • Trastuzumab (Herceptin®) directed against the HER-2 receptor and approved for treatment of metastatic breast cancer •C etuximab (Erbitux®) and panitumumab (Vectibix®) directed against the epidermal growth factor receptor (EGFR) and approved for treatment of e.g. colorectal cancer •B evacizumab (avastin™) directed against the vascular endothelial growth factor (VEGF) and approved for treatment of colorectal cancer and non-small cell lung cancer •R ituximab (Rituxan®) and 90Y-ibritumomab tiuxetan (Zevalin®; see Figure 1) directed against CD20 and approved for treatment of non-Hodgkin’s lymphoma. These MAbs may be used as monotherapy, but more often in combination with chemo- or radiotherapy. Hundreds of new MAbs are under development. The global market for MAbs is expected to triple between 2005 and 2010, to 20-30 billion US dollars. Targeted therapies are highly expensive and will generally be beneficial to only a subgroup of patients, depending on such factors as over-expression of the target, differences in metabolism, and variability and heterogeneity of tumor uptake. In order to understand the efficacy of a certain targeted drug in an individual patient, its uptake in the tumor and normal tissues should be assessed during a scouting procedure prior to the start of therapy or immediately upon the start of a course of therapy. Response to therapy is usually addressed by anatomical (CT) imaging using RECIST criteria. Department of Nuclear Medicine and PET Research, VU Medical Center, Amsterdam, the Netherlands. Departments of Nuclear Medicine and PET Research, and Otolaryngology/ Head and Neck Surgery, VU Medical Center, Amsterdam, the Netherlands However, anatomical changes to treatment are usually not visible during the earliest stages of therapy, and several cycles of therapy are given before response can be assessed. Targeted therapeutic agents have compromised the association of volume-based measures and patient outcomes even further. There is increasing evidence that using PET with a metabolic tracer such as 18F-fluorodeoxyglucose (FDG) shows changes in tumor glucose metabolism before anatomical changes are visible. However, even the use of FDG-PET for response monitoring still requires one or two cycles of therapy before the efficacy of the therapy can be evaluated. Measurement of tumor uptake of the targeted drug, labeled with a positron-emitting nuclide, may provide a predictor of treatment efficacy even before the start of therapy. A PET study with the labeled drug could then be used to select in advance those patients who will benefit from a certain targeted therapy, avoiding unnecessary administration of expensive targeted drugs and avoiding delay in effective treatment for the patient. This, of course, assumes that the kinetics of a tracer amount of the drug are similar to those of pharmacological dosages, so that a tracer study can predict pharmacological distribution of the tracer, and, equally important, that the uptake of the drug in the tumor is an accurate measure of treatment efficacy. Quantitative imaging of targeted drugs is also of value in drug development. Information on the optimal dosage, the uptake in critical organs, and interpatient variations in kinetics and targeting can be obtained at early stages during drug development, thereby allowing for early selection of promising drug candidates and reducing development costs [1]. Labeling of the targeted drug with a positronemitting isotope allows for quantitative PET imaging of the distribution and kinetics of the drug both prior to and during therapy. The radioactive half-lives of the most commonly used PET isotopes, 18F and 11C, are 110 and 20.4 min, E Recent advances in molecular biology have facilitated the identification of tumor cells. E Quantitative imaging of targeted drugs is also of value in drug development. MEDICAMUNDI 54/2 2010 47 respectively. This is too short to measure the kinetics of intact MAbs. The longer half-life positron emitters such as 66 Ga , 64Cu [2], 86Y, 76Br [3], 89Zr [4-6] and 124I [7, 8] have been used for labeling of MAbs, MAb fragments and peptides [4-6, 9-15] and a number of mainly 124I-labeled tracers have been suggested for measuring apoptosis [16, 17], insulin receptors [18], hypoxia [19], and proliferation [20]. The half lives of these isotopes are shown in Table 1. E Table 1. Positron-emitting isotopes for labeling of monoclonal antibodies Isotope 66 Ga 9.5 h 64 Cu 12.7 h Y 14.7 h Br 16.7 h Zr 78 h I 100 h 86 76 Half-life 89 124 labeled with 90Y or 131I, such as 90Y-labeled ibritumomab and 131I-labeled tositumomab (Bexxar™) have been approved for (radio-) immunotherapy [24]. The biological effect of therapy with radionuclides is due to the deposition of energy of ionizing radiation per unit mass of tissue, i.e. the absorbed dose. This is a well-defined physical quantity, unlike those of other systemic treatments such as chemotherapy [25]. Although absorbed dose alone might not be sufficient to fully predict response to radionuclide therapy, with dose rate, type of radiation, and biological characteristics of targeted drug, tumor and normal organs being additional factors that can affect response, knowledge of absorbed doses is required for an optimal application of radionuclide therapy. The amount of radioactivity injected should be chosen such that toxicity to the dose-limiting organ (usually red marrow in the case of antibodies, and the kidneys in the case of smaller molecules such as peptides) is limited, while maximizing tumor absorbed dose. Internal emitter dosimetry 1 In current clinical practice in targeted radiotherapy, radioactivity is usually administered as a fixed amount, or at best as a function of patient size. Absorbed dose calculations, if done at all, are generally performed on a total body or region of interest basis. The necessary parameters for internal emitter dosimetry are the number of decays in each tissue of interest or voxel (cumulative activity) and the geometry of the patient which defines the transport of radiation. Generally three to four measurements of the radioactivity distribution can be made (Figure 2), after which a (dual-)exponential fit through these few data points is used to calculate the cumulative activity in each tissue of interest, and absorbed dose calculations are made using the MIRD (Medical Internal Radiation Dose Committee) approach applying a standardized geometry [26, 27]. G Figure 1. [18F]FDG (left) and 6 days p.i. [89Zr]ibritumomab tiuxetan ([89Zr]Zevalin) PET image of a patient with Non-Hodgkin lymphoma showing high Zevalin uptake in parailiac lymph nodes. FDG uptake in the lymph nodes is only moderate (SUV 2). Images were acquired on a Gemini TF-64 PET-CT scanner (Philips Healthcare). 48 MEDICAMUNDI 54/2 2010 Targeted therapy with radionuclides Several radiopharmaceuticals have gained routine acceptance for radionuclide therapy, with 131I-iodide for the treatment for thyroid cancer being the best known example [21]. Other examples are the use of 131I-labeled MIBG (meta-iodobenzylguanidine) for treatment of neuroblastoma, 90Y, 177Lu or 111In-labeled somatostatin analogues for treatment of neuroendocrine tumors [22], and palliative or adjuvant treatment of skeletal metastases, for example using 89Sr-chloride [23]. Several MAbs In more advanced methods, the geometry used for absorbed dose calculation is based on a CT image of the patient involved. The absorbed dose in organ or tumor due to radiation originating from another organ or tumor is then calculated using voxel S-values [28], dose point kernel methods [29] or Monte-Carlo simulations [30-34] (Figure 3). The main error sources in absorbed dose calculations are the use of a standardized geometry, the computation of the cumulative activity, and the inaccuracy of tissue radioactivity measurements with single photon imaging [35]. F Figure 2. Serial 89Zr-cmAb U36 PET images of a patient with oropharyngeal tumor (indicated by arrows), arranged (left to right) from 1, 24, 72, and 144 h after injection. Gray scale settings were set for each image independently, for clarity. Adapted from Börjesson et al. [36]. 2a 2b Figure 2a. Increased uptake in time of 89Zr-cmAb U36 in tumor (indicated by arrows). Figure 2b. Circulating 89Zr-cmAb U36 in heart and uptake in organs. The distribution of most radionuclides used to deliver the absorbed dose in targeted therapy with radionuclides can either not be imaged at all (90Y, alpha-emitters) or can only be imaged with limited accuracy using single photon scintigraphy (177Lu, 131I). Here, a positronemitting analogue of the therapeutic nuclide can be used, if available, such as 86Y for 90Y [13], 124 I for 131I, 110mIn for 111In [37], or 83Sr for 89Sr [23], but otherwise an isotope with similar chemical properties may be used. An example of this is the use of 89Zr as surrogate for 90Y, which may be preferred to 86Y since 89Zr has more favorable decay characteristics for imaging and, due to its longer half-life, covers more of the kinetics of 90Y [6]. The most straightforward example here is the use of 124I-iodide as an analogue of 131I-iodide in thyroid cancer imaging. In the case of thyroid cancer therapy dosimetry, which is a relatively straightforward example because only a small part of the body needs to be imaged and used for dose calculations, this has even been done on a voxel-by-voxel basis yielding absorbed dose images [38-41] (Figure 3). Quantitative PET with long-lived isotopes Figure 4 shows simplified decay schemes of 124I, 89 Zr and, for comparison, 18F. In contrast with the pure positron emitters 18F and 11C, the longer-lived isotopes mentioned above all emit gamma radiation in addition to positrons. This gamma radiation is often emitted simultaneously with positrons, referred to as “prompt gamma radiation”. In the decay of 124I, for example, about 50% of all positrons (β+1 in Figure 4) are emitted simultaneously with a 603 keV gamma photon (γ1). This additional gamma radiation challenges quantitative image acquisition and image quality in a number of ways. 3 Detection of essentially true coincidences of these prompt gamma photons with each other or with annihilation photons introduces a bias in the images which is not corrected for by the standard PET corrections [42-45] (Figure 5). This bias also results in degraded image contrast [43, 46]. Crude correction methods for this effect have been suggested, in the form of a uniform background subtraction [43, 47], subtraction of a fit to the sinogram data outside the object [43, 48], a convolution subtraction algorithm [45], or a point-spread function subtraction [44], but all of these methods were developed for conventional PET scanners and they cannot be readily used in list-mode image reconstruction with state-of-the-art PET-CT scanners. The single-scatter simulation scatter correction applied on all the latest generation PET and PET-CT scanners [49] usually includes a scaling G Figure 3. Example of 3D 131I absorbed dose calculations in a thyroid cancer patient based on serial PET images with 124I and created using the STRATOS internal radiation dosimetry package on an Imalytics* workstation (Philips Research, Aachen, Germany). Image courtesy of Dr. Bernd Schweizer, Philips Research, and Dr. Walter Jentzen, University Hospital Essen. *This product is not licensed or intended for human diagnostic or therapeutic use. MEDICAMUNDI 54/2 2010 49 Figure 4. Simplified decay schemes of 124I, 89Zr, and, for comparison, the “standard” PET isotope 18F. Only radiation with abundance >1% is shown. 4 The fraction of detected photons with energy outside the scanner’s energy window increases considerably compared to positron-only emitters. Rejection of photons outside the energy window does contribute to dead time, but these photons are not counted in the singles rate. Since the dead time correction is usually implemented as a function of singles rate, it may become inaccurate [42, 54]. 5 G Figure 5 – Degrading effects in PET, from left to right random coincidences, scattered radiation, and prompt gamma coincidences where one of the annihilation photons is detected in coincidence with a prompt gamma photon. Adapted from Lubberink et al. [43]. 50 MEDICAMUNDI 54/2 2010 to match the estimated scatter contribution to the actual events measured just outside the body. If this scaling includes both a multiplicative as well as an additive factor, it implicitly performs a crude correction for a uniform bias caused by prompt gamma coincidences as well [50, 51]. Finally, is has been shown that the distribution of prompt gamma coincidences matches the distribution of random coincidences rather well [52]. Therefore, a correction method involving subtraction of a scaled randoms sinogram could be an accurate correction for prompt gamma coincidences [52], possibly incorporated into the single scatter simulation [53]. The increased singles rate due to gamma radiation leads to increased random coincidence rates. This can be accurately corrected for using the standard delayed window method, but correction for a larger random fraction increases image noise. One option to improve image quality may be the use of a narrower energy window, which reduces random coincidence rates involving higher-energy photons, such as the 603 keV photon emitted by 124I (Figures 6 and 7). The Philips Gemini TF-64 system in use in our research department allows the energy window to be adjusted while working in the research mode, but this is not a capability present in the normal, clinical mode. As can be concluded from the decay schemes in Figure 4, all of these problems affecting image quality and quantitative accuracy occur with 124I. For 89Zr, however, the 909 keV photon is not emitted simultaneously with positrons. Therefore, with 89Zr, an increased random coincidence rate can be expected, but no quantitative bias. Hence, in terms of decay radiation, 89Zr may be considered the optimal PET isotope for labeling MAbs. Future developments An inquiry among nuclear medicine departments in Europe revealed a high demand for new radionuclides, especially 124I [55]. Methods for large-scale production of highly pure 89Zr and 124 I, and for facile and stable coupling of these positron emitters to MAbs, have been developed at VU University Medical Center, Amsterdam [10, 56, 57]. In addition, a GMP facility has been established for large-scale production of these isotopes in quantities exceeding 3 GBq/day, so that these isotopes can be supplied worldwide. Furthermore, the availability of the PET-CT technique is increasing rapidly. For example, in 2002 there were only two PET sites in the Netherlands, but in 2010 there are more than 30, almost all of which are PET-CT. Similar increases can be seen worldwide. This allows for rapid clinical introduction of labeled targeted drugs for individualized therapy, and for development of the related techniques. 6 G Figure 6. Effect of using a narrower energy window. Figure 6a. Noise equivalent count rates, which are a measure of signal-to-noise ratio, of the Gemini TF-64 PET/CT with 11C using the standard 440-665 keV energy window (black), for 124I using this same window (blue) and for 124I using a narrow 440-560 keV window (red). NEC rates were normalized for positron abundance. Figure 6b. Improvement in recovery and image contrast of 124I using the narrower energy window. We foresee a very important role for PET in the development and application of targeted drugs, as recently described by Van Dongen et al. for Mabs [58]. However, despite clinical optimism, it is fair to state that the efficacy of current targeted drugs is still quite limited, with benefits for only a proportion of patients. Moreover, costs of these novel drugs are high, and this item became the subject of national discussions about the right to cancer care (e.g. trastuzumab) in the Netherlands. 7a 7b Important questions are how to improve the efficacy of targeted therapy and how to identify patients with the greatest chance of benefit. In other words: when, how, and for whom should targeted therapy be reserved? Quantitative imaging of targeted drugs can also be a valuable tool at several stages of drug development and application. From first-in-man clinical trials with new drugs it is important to learn about the ideal drug dosage for optimal tumor targeting (e.g. saturation of receptors), the uptake in critical normal organs to anticipate toxicity, and the inter-patient variations in pharmacokinetics and tumor targeting. Drug imaging might provide this information in an efficient and safe way, with fewer patients treated at suboptimal dose. This approach is especially attractive when the drug of interest is directed against a novel tumor target that has not been previously validated in clinical trials. Quantitative drug imaging might also be of value to guide optimal use of FDA-approved drugs, G Figure 7. PET images of a patient with metastatic thyroid cancer at 24 h after administration of 37 MBq 124I acquired on a Gemini TF-64 PET-CT scanner (Philips Healthcare). The narrower energy window (Figure 7b) results in a 15% improvement in image contrast in the largest metastasis (arrow) due to the decreased image background. Figure 7a. 440-665 keV energy window. Figure 7b. 440-560 keV energy window. including selection of patients with the highest chance of benefit from such drugs. To make this happen, software tools for optimal imaging and improved quantification of long-lived positron emitters are urgently needed L MEDICAMUNDI 54/2 2010 51 References [1] Bergstrom M, Grahnen A, Langstrom B. Positron Emission Tomography Microdosing: A New Concept with Application in Tracer and Early Clinical Drug Development. Eur J Clin Pharmacol. 2003; 59(5-6): 357-366. [11]Perk LR, Stigter-Van Walsum, Visser GW, Kloet RW, Vosjan MJWD, Leemans CR, et al. Quantitative PET Imaging of Met-Expressing Human Cancer Xenografts with 89Zr-Labeled Monoclonal Antibody DN30. Eur J Nucl Med Mol Imaging. 2008; 35(10): 1857-1867. [2]Williams HA, Robinson S, Julyan P, Zweit J, Hastings D. A Comparison of PET Imaging Characteristics of Various Copper Radioisotopes. Eur J Nucl Med Mol Imaging. 2005; 32(12): 1473-1480. [12]Perk LR, Visser OJ, Stigter-Van Walsum WM, Vosjan MJWD, Visser GWM, Zijlstra JM, et al. Preparation and Evaluation of (89)Zr-Zevalin for Monitoring of (90)Y-Zevalin Biodistribution with Positron Emission Tomography. Eur J Nucl Med Mol Imaging. 2006; 33(11): 1337-1345. [3]Orlova A, Höglund J, Lubberink M, Lebeda O, Gedda L, Lundqvist H, et al. Comparative Biodistribution of the Radiohalogenated (Br, I and At) Antibody A33. Implications for In Vivo Dosimetry. Cancer Biother Radiopharm. 2002; 17(4): 385-396. [4]Verel I, Visser GWM, Boerman OC, Eerd JEM, Finn R, Boellaard, et al. Long-Lived Positron Emitters Zirconium-89 and Iodine-124 for Scouting of Therapeutic Radioimmunoconjugates with PET. Cancer Biother Radiopharm. 2003; 18(4): 655-661. [5]Verel I, Visser GW, Boellaard R, Stigter-van Walsum M, Snow GB, van Dongen GAMS, et al. Quantitative 89Zr Immuno-PET for In Vivo Scouting of 90Y-Labeled Monoclonal Antibodies in XenograftBearing Nude Mice. J Nucl Med. 2003; 44(10): 1663-1670. [6]Perk LR, Visser GW, Vosjan MJ, Stigter-van Walsum M, Tijink BM, Leemans CR, et al. (89)Zr as a PET Surrogate Radioisotope for Scouting Biodistribution of the Therapeutic Radiometals (90)Y and (177)Lu in Tumor-Bearing Nude Mice after Coupling to the Internalizing Antibody Cetuximab. J Nucl Med. 2005; 46(11): 1898-1906. [7]Eschmann SM, Reischl G, Bilger K, Kupferschläger J, Thelen MH, Dohmen BM, et al. Evaluation of Dosimetry of Radioiodine Therapy in Benign and Malignant Thyroid Disorders by Means of Iodine-124 and PET. Eur J Nucl Med Mol Imaging. 2002; 29(6): 760-767. [8] Erdi YE, Macapinlac H, Larson SM, Erdi AK, Yeung H, Furhang EE, et al. Radiation Dose Assessment for I-131 Therapy of Thyroid Cancer Using I-124 PET Imaging. Clin Positron Imaging. 1999; 2(1): 41-46. [9]Lovqvist A, Lundqvist H, Lubberink M, Tolmachev V, Carlsson J, Sundin A. Kinetics of 76Br-Labeled Anti-CEA Antibodies in Pigs; Aspects of Dosimetry and PET Imaging Properties. Med Phys. 1999; 26(2): 249-258. [10]Perk LR, Vosjan MJ, Visser GW, Budde M, Jurek P, Kiefer GE, et al. P-Isothiocyanatobenzyl-Desferrioxamine: A New Bifunctional Chelate for Facile Radiolabeling of Monoclonal Antibodies with Zirconium-89 for Immuno-PET Imaging. Eur J Nucl Med Mol Imaging. 2010; 37(2): 250-259. 52 MEDICAMUNDI 54/2 2010 [13]Herzog H, Rosch F, Stocklin G, Lueders C, Qaim SM, Feinendegen LE. Measurement of Pharmacokinetics of Yttrium-86 Radiopharmaceuticals with PET and Radiation Dose Calculation of Analogous Yttrium-90 Radiotherapeutics. J Nucl Med. 1993; 34(12): 2222-2226. [14]Rösch F, Herzog H, Stolz B, Brockmann J, Köhle M, Mühlensiepen H, et al. Uptake Kinetics of the Somatostatin Receptor Ligand [ 86Y]DOTA-Dphe1- Tyr3-Octreotide ([86Y]SMT487) using Positron Emission Tomography in Non-Human Primates and Calculation of Radiation Doses of the 90Y-Labeled Analogue. Eur J Nucl Med. 1999; 26(4): 358-366. [15]Graham MC, Pentlow KS, Mawlawi O, Finn RD, Daghighian F, Larson SM. An Investigation of the Physical Characteristics of 66Ga as an Isotope for PET Imaging and Quantification. Med Phys. 1997; 24(2): 317-326. [16]Keen HG, Dekker BA, Disley L, Hastings D, Lyons S, Reader AJ, et al. Imaging Apoptosis in Vivo Using 124I-Annexin V and PET. Nucl Med Biol. 2005; 32(4): 395-402. [17]Dekker B, Keen H, Lyons S, Disley L, Hastings D, Reader A, et al. MBP-Annexin V Radiolabeled Directly with Iodine-124 can be used to Image Apoptosis In Vivo Using PET. Nucl Med Biol. 2005; 32(3): 241-252. [18]Iozzo P, Osman S, Glaser M, Knickmeier M, Ferrannini E, Pike VW, et al. In Vivo Imaging of Insulin Receptors by PET: Preclinical Evaluation of Iodine-125 and Iodine-124 Labeled Human Insulin. Nucl Med Biol. 2002; 29(1): 73-82. [19]Zanzonico P, O’Donoghue J, Chapman JD, Schneider R, Cai S, Larson S, et al. Iodine-124-Labeled Iodo-Azomycin-Galactoside Imaging of Tumor Hypoxia in Mice with Serial Micropet Scanning. Eur J Nucl Med Mol Imaging. 2004; 31(1): 117-128. [20]Roelcke U, Hausmann O, Merlo A, Missimer J, Maguire RP, Freitag P, et al. PET Imaging Drug Distribution After Intratumoral Injection: The Case for (124)I-Iododeoxyuridine in Malignant Gliomas. J Nucl Med. 2002; 43(11): 1444-1451. [21]Sawka AM, Thephamongkhol K, Brouwers M, Thabane L, Browman G, Gerstein HC. Clinical Review 170: A Systematic Review and Metaanalysis of the Effectiveness of Radioactive Iodine Remnant Ablation for Well-Differentiated Thyroid Cancer. J Clin Endocrinol Metab. 2004; 89(8): 3668-3676. [22]Van Essen M, Krenning EP, De Jong M, Valkema R, Kwekkeboom DJ. Peptide Receptor Radionuclide Therapy with Radiolabelled Somatostatin Analogues in Patients with Somatostatin Receptor Positive Tumours. Acta Oncol. 2007; 46(6): 723-734. [23]Lundqvist H, Lubberink M, Tolmachev V, Lövqvist A, Sundin A, Beshara S, et al. Positron Emission Tomography and Radioimmunotargeting - General Aspects. Acta Oncol. 1999; 38(3): 335-341. [24]Wiseman GA, White CA, Sparks RB, Erwin WD, Podoloff DA, Lamonica D, et al. Biodistribution and Dosimetry Results from a Phase III Prospectively Randomized Controlled Trial of Zevalin Radioimmunotherapy for Low-Grade, Follicular, or Transformed B-Cell Non-Hodgkin’s Lymphoma. Crit Rev Oncol Hematol. 2001; 39(1-2): 181-194. [25]Sgouros G. Dosimetry of Internal Emitters. J Nucl Med. 2005; 46 Suppl 1: 18S-27S. [26]Siegel JA, Thomas SR, Stubbs JB, Stabin MG, Hays MT, Koral KF, et al. MIRD Pamphlet No. 16: Techniques for Quantitative Radiopharmaceutical Biodistribution Data Acquisition and Analysis for Use in Human Radiation Dose Estimates. Journal of Nuclear Medicine. 1999; 40(2): 37S-61S. [27]Stabin MG, Sparks RB, Crowe E. OLINDA/EXM: The SecondGeneration Personal Computer Software for Internal Dose Assessment in Nuclear Medicine. J Nucl Med. 2005; 46(6): 1023-1027. [28]Bolch WE, Bouchet LG, Robertson JS, Wessels BW, Siegel JA, Howell RW, et al. MIRD Pamphlet No. 17: the Dosimetry of Nonuniform Activity Distributions--Radionuclide S Values at the Voxel Level. Medical Internal Radiation Dose Committee. J Nucl Med. 1999; 40(1): 11S-36S. [29]Furhang EE, Sgouros G, Chui CS. Radionuclide Photon Dose Kernels for Internal Emitter Dosimetry. Med Phys. 1996; 23(5): 759-764. [30]Strand SE, Jonsson BA, Ljungberg M, Tennvall J. Radioimmunotherapy Dosimetry - A Review. Acta Oncologica. 1993; 32(7-8): 807-817. [31]Ljungberg M, Frey E, Sjogreen K, Liu X, Dewaraja Y, Strand SE. 3D Absorbed Dose Calculations Based On SPECT: Evaluation for 111-In/90-Y Therapy Using Monte Carlo Simulations. Cancer Biother Radiopharm. 2003; 18(1): 99-107. [32]Furhang EE, Chui CS, Sgouros G. A Monte Carlo Approach to Patient-Specific Dosimetry. Med Phys. 1996; 23(9): 1523-1529. [33]Furhang EE, Chui CS, Kolbert KS, Larson SM, Sgouros G. Implementation of a Monte Carlo Dosimetry Method for PatientSpecific Internal Emitter Therapy. Med Phys. 1997; 24(7): 1163-1172. [34]Song H, Du Y, Sgouros G, Prideaux A, Frey E, Wahl RL. Therapeutic Potential of 90Y- and 131I-Labeled Anti-CD20 Monoclonal Antibody in Treating Non-Hodgkin’s Lymphoma with Pulmonary Involvement: A Monte Carlo-Based Dosimetric Analysis. J Nucl Med. 2007; 48(1): 150-157. [35]Norrgren K, Svegborn SL, Areberg J, Mattsson S. Accuracy of the Quantification of Organ Activity from Planar Gamma Camera Images. Cancer Biother Radiopharm. 2003; 18(1): 125-131. [36]Borjesson PK, Jauw YW, de Bree R, Roos JC, Castelijns JA, Leemans CR, van Dongen GA, Boellaard R, et al. Radiation Dosimetry of 89Zr-Labeled Chimeric Monoclonal Antibody U36 as used for Immuno-PET in Head and Neck Cancer Patients. J Nucl Med. 2009; 50(11): 1828-1836. [37]Lubberink M, Tolmachev V, Widström C, Bruskin A, Lundqvist H, Westlin JE. 110min-DTPA-D-Phe1-Octreotide for Imaging of Neuroendocrine Tumors with PET. J Nucl Med. 2002; 43(10): 1391-1397. [38]Kolbert KS, Sgouros G, Scott AM, Bronstein JE, Malane RA, Zhang J, et al. Implementation and Evaluation of Patient-Specific Three-Dimensional Internal Dosimetry. J Nucl Med. 1997; 38(2): 301-308. [39]Prideaux AR, Song H, Hobbs RF, He B, Frey EC, Ladenson PW, et al. Three-Dimensional Radiobiologic Dosimetry: Application of Radiobiologic Modeling to Patient-Specific 3-Dimensional ImagingBased Internal Dosimetry. J Nucl Med. 2007; 48(6): 1008-1016. [40]Sgouros G, Kolbert KS, Sheikh A, Pentlow KS, Mun EF, Barth A, et al. Patient-Specific Dosimetry for 131I Thyroid Cancer Therapy Using 124I PET and 3-Dimensional-Internal Dosimetry (3D-ID) Software. J Nucl Med. 2004; 45(8): 1366-1372. [41]Kolbert KS, Pentlow KS, Pearson JR, Sheikh A, Finn RD, Humm JL, et al. Prediction of Absorbed Dose To Normal Organs in Thyroid Cancer Patients Treated with 131I by Use of 124I PET and 3-Dimensional Internal Dosimetry Software. J Nucl Med. 2007; 48(1): 143-149. [42]Martin CC, Christian BT, Satter MR, Nickerson LDH, Nickles RJ. Quantitative PET with Positron Emitters That Emit Prompt Gamma Rays. IEEE Trans Med Imaging. 1995; 14(4): 681-687. MEDICAMUNDI 54/2 2010 53 [43]Lubberink M, Schneider H, Bergström M, Lundqvist H. Quantitative Imaging and Correction for Cascade Gamma Radiation of 76Br with 2D and 3D PET. Phys Med Biol. 2002; 47(19): 3519-3534. [56]Tijink BM, Perk LR, Budde M, Stigter-van Walsum M, Visser GW, Kloet RW, et al. (124)I-L19-SIP for Immuno-PET Imaging of Tumor Vasculature and Guidance of (131)I-L19-SIP Radioimmunotherapy. Eur J Nucl Med Mol Imaging. 2009; 36(8): 1235-1244. [44]Walrand S, Jamar F, Mathieu I, De Camps J, Lonneux M, Sibomana M, et al. Quantitation in PET using Isotopes Emitting Prompt Single Gammas: Application To Yttrium-86. Eur J Nucl Med Mol Imaging. 2003; 30(3): 354-361. [57]Vosjan MJ, Perk LR, Visser GW, Budde M, Jurek P, Kiefer GE, et al. Conjugation and Radiolabeling of Monoclonal Antibodies with Zirconium-89 for PET Imaging Using the Bifunctional Chelate P-Isothiocyanatobenzyl-Desferrioxamine. Nature Protocols. 2010; 5: in Press. [45]Beattie BJ, Finn RD, Rowland DJ, Pentlow KS. Quantitative Imaging of Bromine-76 and Yttrium-86 with PET: A Method for the Removal of Spurious Activity Introduced by Cascade Gamma Rays. Med Phys. 2003; 30(9): 2410-2423. [46]Lubberink M, Van Schie A, De Jong HW, Van Dongen GA, Teule GJ. Acquisition Settings for PET of 124I Administered Simultaneously with Therapeutic Amounts of 131I. J Nucl Med. 2006; 47(8): 1375-1381. [47]Pentlow KS, Finn RD, Larson SM, Erdi YE, Beattie BJ, Humm JL. Quantitative Imaging of Yttrium-86 with PET. The Occurrence and Correction of Anomalous Apparent Activity in High Density Regions. Clin Positron Imaging. 2000; 3(3): 85-90. [48]Kull T, Ruckgaber J, Weller R, Reske S, Glatting G. Quantitative Imaging of Yttrium-86 PET with the ECAT EXACT HR+ in 2D Mode. Cancer Biother Radiopharm. 2004; 19(4): 482-490. [49]Watson CC. New, Faster, Image-Based Scatter Correction for 3D PET. IEEE Trans Nucl Sci. 2000; 47(4): 1587-1594. [50]Gregory R, Partridge M, Flux GD. Assessment of Cascade Correction Methods for Quantitative 124I PET Imaging. Eur J Nucl Med Mol Imaging. 2009; 36: OP066. [51]Surti S, Scheuermann R, Karp JS. Correction Technique for Cascade Gammas in I-124 Imaging on a Fully-3D, Time-Of-Flight PET Scanner. IEEE Trans Nucl Sci. 2009; 56(3): 653-660. [52]Lubberink M. Quantitative Imaging with PET - Performance and Applications of 76Br, 52Fe, 110mIn and 134La. Uppsala: Acta Universitatis Upsaliensis. Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1034; 2001. [53]Watson CC, Hayden C, Casey ME, Hamill J, Bendriem B. Prompt Gamma Correction for Improved Quantification in 82Rb PET. J Nucl Med. 2008; 49: 64P. [54]Lubberink M, Schneider H, Bergström M, Lundqvist H. Count Rate Characteristics of PET with Bromine-76. European Journal of Nuclear Medicine. 2001; 28(8): 1008. [55]Bockisch A, Freudenberg L, Rosenbaum S, Jentzen W. (124)I in PET Imaging: Impact On Quantification, Radiopharmaceutical Development and Distribution. Eur J Nucl Med Mol Imaging. 2006; 33(11): 1247-1248. 54 MEDICAMUNDI 54/2 2010 [58]Van Dongen GA, Visser GW, Lub-De Hooge MN, De Vries EG, Perk LR. Immuno-PET: A Navigator in Monoclonal Antibody Development and Applications. Oncologist. 2007; 12(12): 1379-1389.