Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
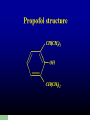
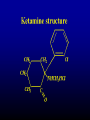
CNS Depressants Prof. Faris Abachi College of Pharmacy University of Mosul Classifications 1- General Anesthesia 2- Sedative – Hypnotics 3- Anti – psychotic drugs 4- Anti – Consultants drugs. . Mode of Action Positive modulation of the action of γ – amino butyric acid (GABA) at GABAA receptor .Except anti consultants has been associated with neuronal voltage - gated sodium channel block , leading to decrease neuronal excitation . What are General Anesthetics? A drug that brings about a reversible loss of consciousness. These drugs are generally administered by an anesthesiologist in order to induce or maintain general anesthesia to facilitate surgery. Background General anesthesia was absent until the mid-1800’s William Morton administered ether to a patient having a neck tumor removed at the Massachusetts General Hospital, Boston, in October 1846. The discovery of the diethyl ether as general anesthesia was the result of a search for means of eliminating a patient’s pain perception and responses to painful stimuli. (CH3CH2)2O HISTORY OF ANESTHESIA INHALATION AGENTS Nitrous Oxide 1799 Davy 1824 Hickman 1844 Wells Ether 1842 Long 1847 Snow Anesthetics divide into 2 classes: Inhalation Anesthetics – – Gasses or Vapors Usually Halogenated Intravenous Anesthetics – – Injections Anesthetics or induction agents Inhaled Anesthetics Halothane Enflurane Isoflurane Desflurane Halogenated compounds: Contain Fluorine and/or bromide Simple, small molecules Nomenclature Halothane is an inhalational general anesthetic. Its IUPAC name is 2-bromo-2-chloro1,1,1trifluoroethane. Stages of Anesthesia 1- Stage I :Cortical stage 2- Stage II :Excitement 3- Stage III :surgical Anesthesia 4- Stage IV :Modularly Paralysis Component of general anesthesia 1-Uncinicousness ( Hypnosis ) 2- Analgesia 3- Muscles relaxants . Routine Monitors ECG. BP. Oximetry (2 wavelengths , red and infrared) End Tidal CO2 . Temperature (axillary vs. core). FUTURE : Depth of anesthesia - BIS (Bispectral index EEG) -scale from 0 to 100 BIS > 65 deepen. Physical and Chemical Properties of Inhaled Anesthetics Although halogenations of hydrocarbons and ethers increase anesthetic potency, it also increase the potential for inducing cardiac arrhythmias in the following order F<Cl<Br.1 Ethers that have an asymmetric halogenated carbon tend to be good anesthetics (such as Enflurane). Halogenated methyl ethyl ethers (Enflurane and Isoflurane) are more stable, are more potent, and have better clinical profile than halogenated diethyl ethers. fluorination decrease flammibity and increase stability of adjacent halogenated carbons. Complete halogenations of alkane and ethers or full halogenations of end methyl groups decrease potency and enhances convulsant activity. Flurorthyl (CF3CH2OCH2CF3) is a potent convulsant, with a median effective dose (ED50) for convulsions in mice of 0.00122 atm. The presence of double bonds tends to increase chemical reactivity and toxicity. SAR for Inhalated Gases 7 8 1 C C 6 5 2 O C 4 3 Diethyl ether Fluroxene Methoxyflurane Desflurane Isoflurane Enflurane Sevoflurane MW 74 126 165 168 184 184 200 1 H H F H H F H 2 3 4 5 H CH3 H H H =CH2 H H H H F F H F F F H F Cl F H F F H F H CF3 6 H F Cl F F Cl F 7 H F H F F H F 8 H F Cl F F F F Intravenous Anesthetics Used in combination with Inhaled anesthetics to: – – – – – Supplement general anesthesia Maintain general anesthesia Provide sedation Control blood pressure Protect the brain Intravenous Anesthetics Thiopental Sodium ( Ultrashort acting barbiturates), 3D-structure ; Benzodiazepines Alone cant produce surgical anesthesia, i.v. used to introduce anesthesia.Relaxant. Uses of Benzodiazepines Benzodiazepines generally share the same pharmacological properties, such as anxiolytic, sedative, hypnotic, skeletal muscle relaxant, amnesic and anticonvulsant (hypertension in combination with other anti hypertension medications). Propofol ( Diprivan ) It is a 2 , 6 diisopropylphenol (Emulsion ) Used o inducion and maintenance of anesthesia . Has lipid / water P.C. The drug binds alloster ically o GABA A2 Ketamine Hydrochloride ( Ketalar) ± 2- ( o-chlorophenyl) -2- methyl amino cyclohexanone HCI . ( racemic mixtures ) Ketamine produces a sense of dissociation from events being experienced , followed by anesthesia , analgesia and sometimes amnesia. Essential Components of Anesthesia Analgesia- perception of pain eliminated Hypnosis- unconsciousness Depression of spinal motor reflexes Muscle relation * These terms together emphasize the role of immobility and of insensibility! Hypotheses of General Anesthesia 1. Lipid Theory: based on the fact that anesthetic action is correlated with the oil/gas coefficients. The higher the solubility of anesthetics is in oil, the greater is the anesthetic potency. Meyer and Overton Correlations Irrelevant 2. Protein (Receptor) Theory: based on the fact that anesthetic potency is correlated with the ability of anesthetics to inhibit enzymes activity of a pure, soluble protein. Also, attempts to explain the GABAA receptor is a potential target of anesthetics acton. Other Theories included Binding theory: – Anesthetics bind to hydrophobic portion of the ion channel Mechanism of Action UNKNOWN!! Most Recent Studies: – – General Anesthetics acts on the CNS by modifying the electrical activity of neurons at a molecular level by modifying functions of ION CHANNELS. This may occur by anesthetic molecules binding directly to ion channels or by their disrupting the functions of molecules that maintain ion channels. Cont on Mechanism Scientists have cloned forms of receptors in the past decades, adding greatly to knowledge of the proteins involved in neuronal excitability. These include: – – – Voltage-gated ion channels, such as sodium, potassium, and calcium channels Ligand-gated ion channel superfamily and G protein-coupled receptors superfamily. Anesthetic Suppression of Physiological Response to Surgery Pharmacokinetics of Inhaled Anesthetics 1. Amount that reaches the brain 1. 2. Partial Pressure of anesthetics 1. 3. 5% anesthetics = 38 mmHg Solubility of gas into blood 1. 4. Indicated by oil:gas ratio (lipid solubility) The lower the blood:gas ratio, the more anesthetics will arrive at the brain Cardiac Output 1. Increased CO= greater Induction time Rate of Entry into the Brain: Influence of Blood and Lipid Solubility Increase in Anesthetic Partial Pressure in Blood is Related to its Solubility General Actions of Inhaled Anesthetics Respiration – Kidney – Depressed respiration and response to CO2 Depression of renal blood flow and urine output Muscle – High enough concentrations will relax skeletal muscle Cont’ Cardiovascular System – Generalized reduction in arterial pressure and peripheral vascular resistance. Isoflurane maintains CO and coronary function better than other agents Central Nervous System – Increased cerebral blood flow and decreased cerebral metabolism