Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
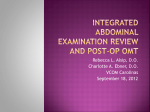
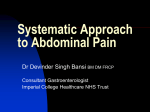
Recurrent epiploic appendagitis mimicking appendicitis and cholecystitis Claudia Lorente, MSc, Christopher B. Hearne, MD, and Jorge Taboada, MD Epiploic appendagitis (EA) is a rare cause of acute abdominal pain caused by inflammation of an epiploic appendage. It has a nonspecific clinical presentation that may mimic other acute abdominal pathologies on physical exam, such as appendicitis, diverticulitis, or cholecystitis. However, EA is usually benign and self-limiting and can be treated conservatively. We present the case of a patient with two episodes of EA, the first mimicking acute appendicitis and the second mimicking acute cholecystitis. Although recurrence of EA is rare, it should be part of the differential diagnosis of acute, localized abdominal pain. A correct diagnosis of EA will prevent unnecessary hospitalization, antibiotic use, and surgical procedures. E piploic appendagitis (EA) is a rare cause of acute abdominal pain that is usually benign and self-limiting and can be treated conservatively with analgesics and antiinflammatory medications (1–3). Recurrence of EA is rare, and documented cases describe abdominal pain recurring at the same location (3–5). We describe the case of a patient with two episodes of EA, the first mimicking acute appendicitis and the second mimicking acute cholecystitis. CASE REPORT A 66-year-old Caucasian woman presented with a 3-day history of progressively worsening right mid abdominal pain exacerbated by positional change. On a pain scale of 1 to 10, she rated the pain an 8. She had some degree of anorexia, but denied any associated chills, fever, nausea, vomiting, change in bowel habits, or skin rash. Her past medical history included hypertension, hyperlipidemia, hypothyroidism, and stress-induced cardiomyopathy. Her only abdominal surgeries consisted of C-sections. Two years prior, she had a colonoscopy showing no diverticulosis or significant polyps. Her family history was significant for gallbladder disease requiring cholecystectomies. On physical examination, she was ambulatory and not in acute distress. She was afebrile, nonicteric, had normal vital signs, and had a body mass index (BMI) of 30 kg/m2. Abdominal exam revealed tenderness with some degree of guarding along the right flank. Bowel sounds were present. The differential diagnosis included retrocecal appendicitis and EA. The complete blood count and comprehensive metabolic panel 44 were normal. Computed tomography (CT) findings, shown in Figure 1, were diagnostic for EA. The patient was treated with analgesics and antiinflammatory medication. Her symptoms resolved after 2 days of treatment. She returned 19 months later with a 2-day history of constant sharp right upper quadrant pain aggravated by movement and similar in quality and severity to the pain she had experienced during her diagnosis of EA months earlier, this time without associated anorexia. The pain radiated towards the epigastric region. On physical examination she appeared uncomfortable, pressing her hand against her right subcostal region. She had normal vital signs, and her BMI was now 28 kg/m2 after dieting. Key findings on physical exam were point tenderness in the right upper quadrant with a positive Murphy sign. A positive Murphy sign increases the likelihood of an inflamed gallbladder and occurs when the patient arrests inspiration as the examiner palpates the abdominal right upper quadrant while the patient is taking a deep breath. The differential diagnosis included acute cholecystitis and recurrent EA. Her complete blood count, comprehensive metabolic panel, and lipase levels were normal. Abdominal ultrasonography showed a normal gallbladder, liver, and pancreas. Once again, the CT scan was diagnostic (Figure 2), showing a mass of similar size and location as the previous EA lesion. The patient was treated with analgesics and antiinflammatory medication, and her symptoms resolved within 5 days. DISCUSSION Epiploic appendages are 50 to 100 pedunculated peritoneal fat pouches oriented in two rows parallel to the taenia coli of the colon, between the cecum and rectosigmoid junction, each usually 1 to 2 cm thick and 0.5 to 5 cm long (3). Each epiploic appendage is supplied by two endarteries, originating from the vasa recta, and one single tortuous vein that passes through a narrow stalk at its base (3). The peduncular shape and From the Department of Internal Medicine (Hearne) and Department of Radiology (Taboada), Baylor Scott & White Health; and the Texas A&M Health Science Center College of Medicine (Lorente). Corresponding author: Claudia Lorente, MSc, College of Medicine, Texas A&M Health Science Center, 3950 North A. W. Grimes Blvd., Round Rock, TX 78665 (e-mail: [email protected]). Proc (Bayl Univ Med Cent) 2017;30(1):44–46 a b Figure 1. (a) Axial and (b) coronal CT images. The oval-shaped inflamed epiploic appendage (2.4 × 1.4 cm) which has fat attenuation is outlined by the peripheral rim of hyperattenuation (white arrows). Outside the borders of the appendage, surrounding fat stranding (black arrows) is seen. On the coronal image, a central dot of high attenuation is present, likely representing a thrombosed vein. narrow vascular supply stalk makes epiploic appendages prone to torsion, leading to ischemic or hemorrhagic infarction, and susceptible to venous thrombosis (3). Primary EA is a rare cause of acute abdominal pain thought to be caused by appendage torsion or venous thrombosis (3). In a case series of 58 patients with EA, 48% of cases occurred in the sigmoid colon, 28% in the descending colon, 7% in the transverse colon, and 17% in the ascending colon (6). Thus, EA often presents with lower abdominal pain mimicking diverticulitis and appendicitis, and there are few documented presentations that mimic cholecystitis (7, 8). Secondary EA results from inflammation of an adjacent organ, such as cholecystitis, pancreatitis, diverticulitis, or appendicitis (5, 9). These infarcted appendages undergo fat necrosis and calcify and may either stay attached to the colon or detach to become peritoneal loose bodies or “parasitized epiploic appendages” by reattaching to surfaces within the abdominal cavity, like the spleen (3). a Primary EA clinically presents as an abrupt onset of acute, well-localized, nonmigratory abdominal pain, often in the lower abdominal quadrants, that worsens with movement. The patient usually is afebrile without nausea, vomiting, anorexia, or change in bowel function (3, 6). On physical examination the patient presents with localized tenderness and possible guarding. Usually vital signs and laboratory values are within normal limits, but mild leukocytosis and slight elevation of C-reactive protein have been reported in some cases (1, 3, 4). EA is diagnosed via CT scan (preferred) and ultrasonography (6, 9). In CT, the inflamed epiploic appendage usually appears as a 1.5-cm to 3.5-cm fat-attenuation lesion adjacent to the colon with a peripheral rim of hyperattenuation (representing inflamed peritoneum), usually with a central dot of high attenuation (representing the thrombosed vein), with surrounding fat stranding (representing increased edema), and with asymmetric wall thickening of the colon, due to the inflammation being b Figure 2. (a) Axial and (b) coronal CT images obtained 19 months after the initial study. Either the same or a neighboring epiploic appendage (2.0 × 2.5 cm) anterior to the ascending colon is inflamed, with a peripheral rim of hyperattenuation (white arrows) with surrounding inflammatory changes. January 2017 Recurrent epiploic appendagitis mimicking appendicitis and cholecystitis 45 greater in the area surrounding the colon than on the colon wall itself (6, 9). Omental infarctions and mesenteric panniculitis may have clinical presentations similar to that of EA, but can be distinguished from EA on CT because omental infarctions usually are larger than 5 cm and lack a hyperattenuating rim (9), and mesenteric panniculitis appears as a fat-attenuation lesion within the mesentery usually with a “fat-ring sign,” which represents preserved noninflamed fat around vessels (9). Ultrasonography identifies an inflamed epiploic appendage as a noncompressible hyperechoic mass adjacent to the colon wall at the site of pain usually with a hypoechoic rim, representing inflamed peritoneum, and absence of blood flow on Doppler due to torsion or thrombosis (9). Before CT scans were established as standard diagnostic imaging tools, EA was a surgical diagnosis treated by laparoscopic surgical excision. However, EA is considered a benign, self-limiting lesion that usually resolves spontaneously within days to weeks and can be treated conservatively with over-thecounter analgesics and antiinflammatory medications (1, 2). Rarely, surgical interventions are needed due to complications, such as small bowel obstruction due to adhesions or external compression (6). Recurrence of EA is rare, but has been documented in cases managed conservatively. In a case study of 10 patients with EA treated conservatively, Sand et al observed recurrence of EA in 4 out of the 10 patients (3). Recurrence was also observed in a case report of one patient on peritoneal dialysis (4). Authors of both articles suggest involvement of the same epiploic appendage in both presentations and recommend considering laparoscopic excision for these cases. Only one case report described recurrence of EA involving two distinct epiploic appendages, both with similar presentation and treated by laparoscopic excision due to severe symptoms (5). Even though surgical excision would remove the inflamed epiploic appendage that is causing irritation, the benefit of surgical excision should be weighed against its risks—mainly anesthesia complications, excessive bleeding, and infection—and cost (1–3). The patient in this report had two occurrences of EA, each with similar clinical presentation but eliciting pain in different abdominal quadrants, first with right flank pain, mimicking retrocecal appendicitis, and later in the right upper quadrant, mimicking acute cholecystitis. Possible risk factors for develop- 46 ing EA are obesity and postprandial strenuous exercise, supported by some case reports (7, 10) but not by others (3). From the patient’s past medical history, only obesity (BMI >30 kg/m2) during the first episode of EA and being overweight (BMI 25– 29.9 kg/m2) during the second episode could predispose her for developing EA. CT scans taken in each instance found an inflamed epiploic appendage of similar dimensions in the ascending colon adjacent to the hepatic flexure. The recurrent EA could be due to involvement of the same epiploic appendage in both presentations, causing pain in different quadrants because the colon has some range of mobility within the abdominal cavity, or it could be due to involvement of a neighboring epiploic appendage. EA should be part of the differential diagnosis of acute abdominal pain because it is a benign, self-limiting lesion that can be diagnosed with CT and treated conservatively. Correct diagnosis avoids unnecessary hospitalizations, antibiotic treatment, and surgeries. 1. Schnedl WJ, Krause R, Wallner-Liebmann SJ, Tafeit E, Mangge H, Tillich M. Primary epiploic appendagitis and successful outpatient management. Med Sci Monit 2012;18(6):CS48–CS51. 2. Rao PM, Rhea JT, Wittenberg J, Warshaw AL. Misdiagnosis of primary epiploic appendagitis. Am J Surg 1998;176(1):81–85. 3. Sand M, Gelos M, Bechara FG, Sand D, Wiese TH, Steinstraesser L, Mann B. Epiploic appendagitis—clinical characteristics of an uncommon surgical diagnosis. BMC Surg 2007;7:11. 4. Shrestha B, Hampton J. Recurrent epiploic appendagitis and peritoneal dialysis: a case report and literature review. World J Nephrol 2014;3(3): 114–117. 5. Marschall J, Karimuddin A, Hayes P. Soft-tissue case 44. Recurrent epiploic appendagitis. Can J Surg 2002;45(2):93:154–155. 6. Patel NB, Wenzke DR. Evaluating the patient with right lower quadrant pain. Radiol Clin North Am 2015;53(6):1159–1170. 7. Lien WC, Lai TI, Lin GS, Wang HP, Chen WJ, Cheng TY. Epiploic appendagitis mimicking acute cholecystitis. Am J Emerg Med 2004;22(6): 507–508. 8. Maillet JM, Thierry S, Sverzut JM, Brodaty D. An unusual cause of acute abdominal pain after cardiac surgery: acute epiploic appendagitis. Interact Cardiovasc Thorac Surg 2012;15(2):292–293. 9. Almeida AT, Melão L, Viamonte B, Cunha R, Pereira JM. Epiploic appendagitis: an entity frequently unknown to clinicians—diagnostic imaging, pitfalls, and look-alikes. AJR Am J Roentgenol 2009;193(5): 1243–1251. 10. Ortega-Cruz HD, Martínez-Souss J, Acosta-Pumarejo E, Toro DH. Epiploic appendagitis, an uncommon cause of abdominal pain: a case series and review of the literature. P R Health Sci J 2015;34(4):219–221. Baylor University Medical Center Proceedings Volume 30, Number 1