Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
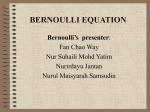
Pulse Pressure Variation Predicts Fluid Responsiveness Following Coronary Artery Bypass Surgery* Andreas Kramer, MD; David Zygun, MD; Harvey Hawes, MSC; Paul Easton, MD, FCCP; and Andre Ferland, MD Study objective: To determine whether the degree of pulse pressure variation (PPV) and systolic pressure variation (SPV) predict an increase in cardiac output (CO) in response to volume challenge in postoperative patients who have undergone coronary artery bypass grafting (CABG), and to determine whether PPV is superior to SPV in this setting. Design and setting: This was a prospective clinical study conducted in the cardiovascular ICU of a university hospital. Patients: Twenty-one patients were studied immediately after arrival in the ICU following CABG. Intervention: A fluid bolus was administered to all patients. Measurements: Hemodynamic measurements, including central venous pressure (CVP), pulmonary artery occlusion pressure (PAOP), CO (thermodilution), percentage of SPV (%SPV), and percentage of PPV (%PPV), were performed shortly after patient arrival in the ICU. Patients were given a rapid 500-mL fluid challenge, after which hemodynamic measurements were repeated. Patients whose CO increased by > 12% were considered to be fluid responders. The ability of different parameters to distinguish between responders and nonresponders was compared. Results: In response to the volume challenge, 6 patients were responders and 15 were nonresponders. Baseline CVP and PAOP were no different between these two groups. In contrast, the %SPV and the %PPV were significantly higher in responders than in nonresponders. Receiver operating characteristic curve analysis suggested that the %PPV was the best predictor of fluid responsiveness. The ideal %PPV threshold for distinguishing responders from nonresponders was found to be 11. A PPV value of > 11% predicted an increase in CO with 100% sensitivity and 93% specificity. Conclusion: PPV and SPV can be used to predict whether or not volume expansion will increase CO in postoperative CABG patients. PPV was superior to SPV at predicting fluid responsiveness. Both of these measures were far superior to CVP and PAOP. (CHEST 2004; 126:1563–1568) Key words: cardiac output; preload; pulse pressure variation; systolic pressure variation Abbreviations: CABG ⫽ coronary artery bypass grafting; CO ⫽ cardiac output; CVP ⫽ central venous pressure; HR ⫽ heart rate; LV ⫽ left ventricle, ventricular; LVEDA ⫽ left ventricular end-diastolic area; MAP ⫽ mean arterial pressure; PAOP ⫽ pulmonary artery occlusion pressure; PPV ⫽ pulse pressure variation; %PPV ⫽ percentage of pulse pressure; RV ⫽ right ventricle; SPV ⫽ systolic pressure variation; %SPV ⫽ percentage of systolic pressure; SVV ⫽ stroke volume variation measurement of intravascular volume status T heto guide fluid management is an important aspect of caring for critically ill patients. Central venous pressure (CVP) and pulmonary artery occlusion pressure (PAOP) are still commonly used by clinicians in determining whether or not to adminis*From the Brandon Regional Health Center (Dr. Kramer), Brandon, MB, Canada; the Department of Critical Care Medicine (Drs. Zygun, Easton, and Ferland), Foothills Medical Center, Calgary, AB, Canada; and the Faculty of Medicine (Mr. Hawes), University of Calgary, Calgary, AB, Canada. Manuscript received December 2, 2003; revision accepted June 15, 2004. www.chestjournal.org ter fluid. This practice persists despite numerous studies showing that cardiac filling pressures are often misleading when used to predict the effects of volume expansion on cardiac output (CO).1–5 Even the assessment of left ventricular end-diastolic area (LVEDA) with echocardiography is not necessarily a good predictor of fluid responsiveness.5,6 Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (e-mail: [email protected]). Correspondence to: Andreas H. Kramer, MD, Intensive Care Unit, Brandon Regional Health Center, 150 McTavish Ave East, Brandon, MB, R7A 2B3 Canada; e-mail: [email protected] CHEST / 126 / 5 / NOVEMBER, 2004 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22018/ on 05/05/2017 1563 Systolic pressure variation (SPV) and pulse pressure variation (PPV) during mechanical ventilation have been shown to predict the hemodynamic effects of volume expansion in patients with septic shock.5,7 Positive pressure in the thorax has the effect of decreasing preload and increasing afterload in the right ventricle (RV). This leads to a decrease in RV stroke volume during inspiration, which in turn induces a subsequent decrease in LV preload and stroke volume, usually reaching its nadir during expiration.8 In addition, LV stroke volume may increase slightly during inspiration as a consequence of increased LV filling from enhanced pulmonary venous return,9,10 increased LV compliance because of decreased RV dimensions,11 decreased LV afterload,12 and external pressure on the LV.13 Thus, respiratory variations in arterial pressure reflect, in large part, the corresponding cyclic variations in LV stroke volume. These variations are exaggerated when the LV is functioning on the steep portion of the Frank-Starling curve, whereby small changes in preload induce large changes in stroke volume.14 SPV is also due in part to the direct effects of positive pleural pressure on the aorta.15 This effect is potentially avoided with the use of PPV because pleural pressure affects systolic and diastolic BP to the same degree. Indeed, PPV has been shown in one study to be a better index of fluid responsiveness than SPV.7 Patients undergoing coronary artery bypass grafting (CABG) often require postoperative hemodynamic support in the ICU. LV and RV function are known to be depressed for several hours following CABG, probably as a result of multiple factors, including the lingering effects of cardioplegia, myocardial ischemia, reperfusion injury, hypothermiainduced vasoconstriction, and the perioperative use of -blockers. The use of PPV and SPV as predictors of fluid responsiveness may not be as reliable in patients with impaired LV function. Pizov et al16 showed in a dog model that LV depression caused a reduction in SPV. Moreover, with the induction of cardiac failure, a larger proportion of the SPV was due to the “delta up” (ie, the increase in systolic pressure during inspiration) rather than the “delta down” (ie, the decrease in systolic pressure during expiration). SPV may therefore also be indicative of the stroke volume enhancement that occurs due to the afterload-reducing effects of mechanical ventilation rather than reflecting only preload dependence. For this reason, numerous previous studies5,17–19 excluded patients with reduced LV function. In a study of patients undergoing CABG, BennettGuererro et al20 actually found SPV to be inferior to PAOP as a predictor of fluid responsiveness. In contrast, Reuter et al21,22 showed that the degree of stroke volume variation (SVV), assessed using pulse contour analysis, correlated well with changes in CO in response to volume loading in postoperative CABG patients, even when LV function was depressed. The objective of this study was (1) to determine whether PPV and SPV could be used to predict fluid responsiveness in patients recently separated from cardiopulmonary bypass following CABG and (2) to determine whether PPV was superior to SPV in this setting. Materials and Methods Patients The study protocol was approved by the Conjoint Health Research Ethics Board at the University of Calgary. Informed written consent was obtained. Any patient undergoing elective or emergency CABG met the inclusion criteria for the study. Patients were excluded if they had arrhythmias, valvular heart disease, a temperature of ⬍ 34.5°C, PAOP ⬎ 24 mm Hg, or the need to change vasoactive medications during the study protocol because of hemodynamic instability. A total of 21 nonconsecutive patients were studied. Hemodynamics All patients were monitored using an arterial catheter (Cook Critical Care; Bloomington, IN) and a pulmonary artery catheter (Abbott Critical Care Systems; Morgan Hill, CA). Transducers were positioned at the level of the fourth intercostal space in the midaxillary line and were zeroed to atmospheric pressure. BP, heart rate (HR), and CVP were measured continuously. PAOP was assessed at end-expiration. The CO level was determined by thermodilution using the mean of at least three measurements performed at end-expiration. Mechanical Ventilation All patients were sedated with propofol and an opiate to ensure that there was no evidence of spontaneous breathing effort. Mechanical ventilation was performed with tidal volumes of 8 to 10 mL/kg, a positive end-expiratory pressure of 5 mm Hg, and a fraction of inspired oxygen of 0.6. Chest wall excursion was recorded using a band placed around the thorax in order to time BP variation to different phases of the respiratory cycle. BP Variation The arterial pressure tracing was recorded continuously during the first postoperative hour using an analog-to-digital converter and data acquisition software (Datasponge; Bioscience Analysis Software; Calgary, AB, Canada). The mean percentage of PPV (%PPV) and percentage of SPV (%SPV) over 1 min were determined before and after the administration of fluid. These values were calculated as follows: %SPV ⫽ (SBPmax ⫺ SBPmin)/ [(SBPmax ⫹ SBPmin)/2] ⫻ 100% %PPV ⫽ (PPmax ⫺ PPmin)/[(PPmax ⫹ PPmin)/2] ⫻ 100% where SBPmax is maximum SBP, SBPmin is minimum SBP, PPmax is maximum pulse pressure, and PPmin is minimum pulse pressure. 1564 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22018/ on 05/05/2017 Clinical Investigations Table 1—Patient Characteristics* Characteristics Values Gender Male Female Age, yr Weight, kg Elective surgery Recent ACS -blocker Calcium blocker ACE Inhibitor ARB Dopamine,† g/kg/min Phenylephrine,† g/kg/min Epinephrine,† g/kg/min Pump time, min Cross-clamp time, min 15 6 64.7 ⫾ 9.4 87.8 ⫾ 19.9 11 (52) 10 (48) 15 (71) 12 (57) 11 (52) 5 (24) 8/2.8 ⫾ 1.0 7/0.4 ⫾ 0.2 1/0.06 69.5 ⫾ 22.2 49.0 ⫾ 17.7 Values given as No. (%) or mean ⫾ SD, unless otherwise indicated. *ACS ⫽ acute coronary syndrome; ARB ⫽ angiotensin receptor blocker; ACE ⫽ angiotensin-converting enzyme. †Values given as No. of patients/mean dose. Fluid Challenge For volume expansion, we used 500 mL “pump blood,” which is collected during the separation of patients from cardiopulmonary bypass. The fluid bolus was administered rapidly over 10 to 15 min. Hemodynamic measurements were performed immediately before and after the volume challenge. Changes to vasoactive and sedative infusions or to ventilator settings were not permitted during the study period. Based on the work of Stetz et al,23 patients whose CO levels increased by ⱖ 12% in response to volume expansion were considered to be “responders.” The ability of different hemodynamic parameters to predict whether patients would be responders or nonresponders was compared. Statistical Analysis All variables were explored in a univariate manner using classical descriptive statistics. The change in hemodynamic variables associated with volume loading was assessed using the paired Student t test. Between-group comparisons were accomplished with the Student t test when variables were normally distributed and the Mann-Whitney U test if they were not. A p value of ⬍ 0.05 was considered to be statistically significant. Logistic regression models were created to assess the ability of each preload index to predict fluid responsiveness. The discriminative ability of each model was assessed by calculating the area under the receiver operating characteristic curve. Results Overall, 32 patients were recruited, but 11 had to be excluded for the following reasons: insufficient pump blood available (4 patients); spontaneous breathing not suppressed with additional sedation (3 patients); bradycardia requiring pacing (3 patients); and hemodynamic instability (necessitating the use of a cardiac assist device) (1 patient). The characteristics of the remaining 21 patients are described in Table 1. Eleven patients underwent surgery for chronic ischemic heart disease, while 10 patients required urgent revascularization for a recent acute coronary syndrome with high-risk coronary artery blockages. Preoperative investigations revealed that cardiac function was abnormal in numerous patients. Echocardiograms were performed in 17 patients, and were interpreted as showing depressed LV function in 7 patients (41%) and LV hypertrophy in 5 patients (29%). Preoperative cardiac catheterization revealed regional wall motion abnormalities in 16 of 21 patients (76%). Ejection fraction was determined by ventriculogram in 19 of 21 patients and was estimated to be ⬍ 50% in 5 of 19 patients (24%). A total of 9 of 21 patients (43%) had LV end-diastolic pressure measured at ⬎ 18 mm Hg. Hemodynamic measurements at baseline and following volume expansion are shown in Table 2. CO level, mean arterial pressure (MAP), CVP, and PAOP all increased significantly, while HR, %PPV, and %SPV all decreased in response to fluid administration. There was little correlation between base- Table 2—Hemodynamic Variables Before and After Volume Expansion in Fluid Responders and Fluid Nonresponders* Fluid Responders Fluid Nonresponders Variables Baseline Volume Expansion Baseline Volume Expansion HR, beats/min MAP, mm Hg CO, L/min CVP, mm Hg PAOP, mm Hg % PPV % SPV 92.8 ⫾ 13.8† 65.5 ⫾ 3.7† 5.6 ⫾ 1.4 13.5 ⫾ 4.1 11.5 ⫾ 6.1 16.3 ⫾ 4.0‡ 9.3 ⫾ 2.1‡ 88.8 ⫾ 12.8 78.7 ⫾ 12.9 6.7 ⫾ 1.5 16.5 ⫾ 5.2 15.7 ⫾ 5.3 9.1 ⫾ 4.7 5.6 ⫾ 2.2 76.7 ⫾ 12.6 73.1 ⫾ 8.8 6.3 ⫾ 1.7 13.3 ⫾ 2.9 11.9 ⫾ 3.4 7.1 ⫾ 2.7 4.8 ⫾ 1.7 75.1 ⫾ 11.2 80.7 ⫾ 10.6 6.6 ⫾ 1.8 15.3 ⫾ 2.8 14.7 ⫾ 4.2 4.8 ⫾ 1.7 3.7 ⫾ 0.9 *Values given as mean ⫾ SD. †p ⬍ 0.05 vs baseline value in nonresponder. ‡p ⬍ 0.001 vs baseline value in nonresponder. www.chestjournal.org CHEST / 126 / 5 / NOVEMBER, 2004 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22018/ on 05/05/2017 1565 line values of both CVP and PAOP and the percent change in CO following fluid challenge (Fig 1) (r ⫽ ⫺0.13, p ⫽ 0.58 and r ⫽ ⫺0.16, p ⫽ 0.50, respectively). In contrast, the baseline %SPV and the %PPV correlated significantly with the change in CO induced by fluid (r ⫽ 0.65, p ⫽ 0.001 and r ⫽ 0.66, p ⫽ 0.001, respectively). Of the 21 patients, 6 were found to be responders (increase in CO, ⱖ 12%), while 15 were nonresponders. Baseline CVP and PAOP were no different in responders compared with nonresponders. In contrast, the baseline values of %SPV and %PPV were significantly higher in responders than in nonresponders (Table 2). The area under the receiver operating characteristic curve, showing the ability of different hemodynamic parameters to discriminate between responders and nonresponders, was greatest for the %PPV (0.99), followed by the %SPV (0.93) [Table 3]. A PPV of ⱖ 11% predicted an increase in CO of ⱖ 12%, with a sensitivity of 100% and a specificity of 93%. PAOP was only slightly better than chance at predicting fluid responsiveness. Discussion Our results show that variations in arterial pressure during mechanical ventilation can be used to accurately predict the effects of volume expansion in cardiac surgical patients. In contrast, both CVP and PAOP were poor predictors of fluid responsiveness. These findings support those of a systematic review24 that concluded that “dynamic” measures of preload responsiveness (ie, SPV, PPV, inspiratory decrease in CVP, and respiratory changes in aortic blood velocity) are superior to “static” preload parameters (ie, CVP, PAOP, and LVEDA) at guiding fluid management. This review acknowledged that there are still relatively few studies validating dynamic parameters. PPV was the best predictor of fluid responsiveness, with a threshold value of 11% being optimal. Michard et al7 previously found a PPV of 13% to have the highest sensitivity and specificity in predicting an increase in CO in response to volume expansion in a study of septic patients. The rationale for using PPV rather than SPV is that it is more reflective of variations in stroke volume. SPV occurs not only because of variations in stroke volume, but also because of the direct effects of positive pleural pressure on the aorta during inspiration. Therefore, a degree of SPV is observed even if the stroke volume remains constant. In contrast, pleural pressure is transmitted to the aorta during both systole and diastole, such that there should be no impact on PPV. Our findings are of particular interest given the patient population studied. A significant proportion of the patients were recognized preoperatively as having LV dysfunction. Even in those without preoperative cardiac dysfunction, it is well-recognized that LV ejection fraction is usually reduced significantly following CABG. Breisblatt et al25 found that the mean LV ejection fraction of CABG patients was reduced from 58% preoperatively to 46% immediately postoperatively, reaching a nadir of 37% in the first few hours following surgery. Despite the concern that variations in BP in patients with LV dysfunction may reflect the beneficial afterloadreducing properties of mechanical ventilation rather Table 3—Area Under the Receiver Operating Characteristic Curve Showing Ability of Various Hemodynamic Parameters to Predict Fluid Responsiveness* Baseline % PPV % SPV HR MAP PAOP CVP Figure 1. Correlation between the percent change in CO and the baseline values of PAOP and %PPV AUROC 95% CI 0.99 0.94 0.81 0.81 0.63 0.49 0.96–1.00 0.83–1.00 0.61–1.00 0.62–1.00 0.32–0.94 0.18–0.81 *AUROC ⫽ area under the receiver operating characteristic; CI ⫽ confidence interval. 1566 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22018/ on 05/05/2017 Clinical Investigations than only preload dependence, both PPV and SPV were good predictors of fluid responsiveness. It is possible, however, that these measures may not be as useful in patients with more severe cardiac depression than the ones included in this study. Reuter et al21 used pulse contour analysis to determine SVV in a patient population that was similar to ours. In patients with normal preoperative LV function, SVV was superior to PAOP and LVEDA at predicting fluid responsiveness. However, while SVV was still useful in patients who were known preoperatively to have a reduced ejection fraction, it was no better than conventional preload measures in predicting fluid responsiveness in these patients.22 Our study sample was too small to allow a comparison of the utility of PPV in patients with normal preoperative LV function and those with depressed LV function. Bennett-Guerrero et al20 studied CABG patients preoperatively and found SPV to be significantly higher in fluid responders than in nonresponders, but they were unable to determine an optimal threshold value to distinguish the two groups. PPV was not specifically assessed. SPV was reported as an absolute value rather than as a percentage, even though the latter is likely more meaningful.14,26 The methodology used to determine variations in BP from the arterial tracing differed somewhat from that used in our study. Although all information was obtained in a prospective manner, the analysis of the BP tracing was performed after completion of the study protocol, thereby introducing the possibility of bias. This is a weakness that has been apparent in most previous studies of arterial pressure variation. At the time of this study, monitors with the capability of determining these values “on-line” in an automated fashion were not yet available. Because SPV and PPV were determined as the mean value over a whole minute, and therefore several respiratory cycles, we believe that our measurements were very accurate. In our center, pump blood is routinely reinfused into patients on admission to the ICU following coronary bypass surgery. In order to interfere as little as possible with standard patient care, we used this pump blood, rather than colloid or crystalloid, as our means of volume expansion. It should be kept in mind that because properties such as the viscosity and hematocrit of pump blood are not completely consistent, the potency of our fluid challenge will have varied slightly from patient to patient. Given that the goal of our study was to evaluate the ability of SPV and PPV to predict fluid responsiveness in general, rather than predicting the magnitude of response, we do not believe that minor differences in www.chestjournal.org the degree of volume expansion would have influenced our results significantly. The purpose of assessing intravascular volume status in critically ill patients is primarily to determine whether or not they will benefit from the administration of fluid. The overuse of catecholamines without adequate volume resuscitation may result in tissue ischemia. Conversely, the excessive use of fluids with no resultant increase in CO may cause edema and contribute to further tissue injury and organ dysfunction. Despite the inability of conventional static preload parameters such as PAOP and CVP to predict fluid responsiveness, these measures are still commonly used in making decisions about fluid management.27,28 It is possible that the measurement of cardiac filling pressures may help to predict whether or not volume expansion will contribute to edema formation, and therefore act as a safeguard against excessive fluid administration. In summary, both PPV and SPV during controlled mechanical ventilation are useful predictors of increased CO in response to volume expansion in postoperative CABG patients. In this study, PPV was slightly superior to SPV, and far superior to CVP and PAOP at predicting fluid responsiveness. References 1 Raper R, Sibbald W. Misled by the wedge? Chest 1986; 89:427– 433 2 Reuse C, Vincent JL, Pinsky MR. Measurements of right ventricular volumes during fluid challenge. Chest 1990; 98: 1450 –1454 3 Calvin JE, Driedger AA, Sibbald WJ. The hemodynamic effect of rapid fluid infusion in critically ill patients. Surgery 1981; 90:61–76 4 Diebel L, Wilson RF, Tagett MG, et al. End-diastolic volume: a better indicator of preload in the critically ill. Arch Surg 1992; 127:817– 821 5 Tavernier B, Makhotine O, Lebuffe G, et al. Systolic pressure variation as a guide to fluid therapy in patients with sepsisinduced hypotension. Anesthesiology 1998; 89:1313–1321 6 Feissel M, Michard F, Mangin I, et al. Respiratory changes in aortic blood velocity as an indicator of fluid responsiveness in ventilated patients with septic shock. Chest 2001; 119:867– 873 7 Michard F, Boussat S, Chemla D, et al. Relation between respiratory changes in arterial pulse pressure and fluid responsiveness in septic patients with acute circulatory failure. Am J Respir Crit Care Med 2000; 162:134 –138 8 Jardin F, Delorme G, Hardy A, et al. Reevaluation of hemodynamic consequences of positive pressure ventilation: emphasis on cyclic right ventricular afterloading by mechanical lung inflation. Anesthesiology 1990; 72:966 –970 9 Brower R, Wise RA, Hassapoyannes C, et al. Effects of lung inflation on lung blood volume and pulmonary venous flow. J Appl Physiol 1985; 58:954 –963 10 Vieillard-Baron A, Chergui K, Augade R, et al. Cyclic changes in arterial pulse during respiratory support revisited by Doppler echocardiography. Am J Respir Crit Care Med 2003; 168:671– 676 CHEST / 126 / 5 / NOVEMBER, 2004 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22018/ on 05/05/2017 1567 11 Taylor RR, Corell JW, Sonnenblick EH, et al. Dependence of ventricular distensibility on filling the opposite ventricle. Am J Physiol 1967; 213:711–718 12 Pinsky M, Summer W, Wise R, et al. Augmentation of cardiac function by elevation of intra-thoracic pressure. J Appl Physiol 1983; 54:950 –955 13 Pinsky M, Marquez J, Martin D, et al. Ventricular assist by cardiac cycle-specific increases in intrathoracic pressure. Chest 1987; 91:709 –715 14 Michard F, Teboul JL. Respiratory changes in arterial pressure in mechanically ventilated patients. In: Vincent JL, ed. Update in intensive care and emergency medicine. Berlin, Germany: Springer, 2000; 696 –704 15 Denault AY, Gasior TA, Gorcsan J, et al. Determinants of aortic pressure variation during positive-pressure ventilation in man. Chest 1999; 116:176 –186 16 Pizov R, Ya’ari Y, Perel A. The arterial pressure waveform during acute ventricular failure and synchronized external chest compression. Anesth Analg 1989; 68:150 –156 17 Ornstein E, Eidelman LA, Drenger B, et al. Systolic pressure variation predicts the response to acute blood loss. J Clin Anesth 1998; 10:137–140 18 Rooke GA, Schwid HA, Shapira Y. The effect of graded hemorrhage and intravascular volume replacement on systolic pressure variation in humans during mechanical and spontaneous ventilation. Anesth Analg 1995; 80:925–932 19 Coriat P, Vrillon M, Perel A, et al. A comparison of systolic blood pressure variations and echocardiographic estimates of end-diastolic left ventricular size in patients after aortic surgery. Anesth Analg 1994; 78:46 –53 20 Bennett-Guerrero E, Kahn RA, Moskowitz DM, et al. Comparison of arterial systolic pressure variation with other clinical parameters to predict the response to fluid challenges during cardiac surgery. Mt Sinai J Med 2002; 69:97–100 21 Reuter DA, Felbinger TW, Schmidt C, et al. Stroke volume variations for assessment of cardiac responsiveness to volume loading in mechanically ventilated patients after cardiac surgery. Intensive Care Med 2002; 28:392–398 22 Reuter DA, Kirchner MS, Felbinger TW, et al. Usefulness of left ventricular stroke volume variation to assess fluid responsiveness in patients with reduced cardiac function. Crit Care Med 2003; 31:1399 –1404 23 Stetz CW, Miller RG, Kelly GE, et al. Reliability of the thermodilution method in the determination of cardiac output in clinical practice. Am Rev Respir Dis 1982; 126:1001– 1004 24 Michard F, Teboul JL. Predicting fluid responsiveness in ICU patients: a critical analysis of the evidence. Chest 2002; 121:2000 –2008 25 Breisblatt WM, Stein KL, Wolfe CJ, et al. Acute myocardial dysfunction and recovery: a common occurrence after coronary bypass surgery. J Am Coll Cardiol 1990; 15:1261–1269 26 Perel A. Assessing fluid responsiveness by the systolic pressure variation in mechanically ventilated patients. Anesthesiology 1998; 89:1309 –1310 27 Vincent JL. Hemodynamic support in septic shock. Intensive Care Med 2001; 27:S80 –S92 28 Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345:1368 –1377 1568 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22018/ on 05/05/2017 Clinical Investigations