Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
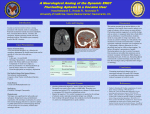
SECOND EXPERT WORKING GROUP (EWG) ON RETROSPECTIVE SEVERITY ASSESSMENT FELASA/ECLAM/ESLAV Contribution Appendix I – Severity Classification and Retrospective Severity Assessment a. Stroke Models ...........................................................................................................................1 b. Drug Dependence model in non-human primate ..................................................................6 a. Stroke Models Stroke is defined as loss or alteration of normal body function that results from an insufficient supply of blood to part of the brain. In the US, stroke is ranked third as cause of death, after cancer and heart disease, with a mortality rate of around 50%. Stroke survivors can suffer from serious, long term disabilities, which results not only in a decreased quality of life for affected patients, but also a huge economic burden for the community. Despite our better understanding of the pathophysiology of vascular brain injury, an effective treatment for stroke remain an important unmet medical need, and more research is needed to find appropriate preventive and therapeutic measures. Three different types of stroke can be seen in human patients: ischaemic, intracerebral haemorrhage and subarachnoid haemorrhage, but most of the animal models currently available are based on the ischaemic type. Rodent species have been routinely used to induce stroke by occlusion (temporary or permanent) of the middle cerebral artery. Following disappointing results in a number of human clinical trials, a number of reports (Fisher et al. ,2009; Braeuninger S and Kleinschnitz C, 2009) have underlined the need to improve translationality of these models by using other animal species in particular non-human primates. The common marmoset has been identified as a suitable model because of its large gyrencephalic brain, despite its small size, and its extensive behavioural repertoire which allows detailed evaluation of manual dexterity before and after the procedure. Stroke models represent a challenge from the perspective of animal welfare. Good interaction between all individuals involved in the experiments (veterinarians, investigators, animal technicians) and the Animal Welfare Body is critical to ensure adequate balance between a valid model in this research area and the welfare of the animals used. References Permanent or transient chronic ischemic stroke in the non-human primate: behavioural, neuroimaging, histological, and immunohistochemical investigations. Bihel et al. J Cereb Blood Flow Metab, 2010;30273-285. Rodent stroke model guidelines for preclinical stroke trials (1st edition).Liu S et al. Journal of experimental stroke and translational medicine, 2009 Jan 1;2(2):2-27. Update of the stroke therapy academic industry roundtable preclinical recommendations. Fisher et al. Stroke,2009 Jun;40(6):2244-50. Recent models of focal cerebral ischemia: procedural pitfalls and translational problems. Braeuninger S and Kleinschnitz C. Experimental & Translational Stroke Medicine, 2009 Nov; 1:8. Improvements of the Stroke Model Guidelines – Animal body weight and long-term functional concerns. Freret T and Bouet V. JExp Stroke Transl Med. 2009; 2(2): 28-31 Intraluminal thread model of focal stroke in the non-human primate. Freret T et al. J Cereb Blood Flow Metab, 2008; 28: 786-796. 1 A new primate model of focal stroke: endothelin-1-induced middle cerebral artery occlusion and reperfusion in the common marmoset. Virley D et al. J Cereb Blood Flow Metab, 2003 Jan;24(1):24-41. Animal models of ischemic stroke: balancing experimental aims and animal care. Graham SM et al. Comparative Medicine, 2004 Oct; 54(5): 486-496 Evaluation of MCAo stroke models in normotensive rats: standardized neocortical infarction by the 3VO technique. Yanamoto H et al. Exp Neurol, 2003 Aug; 182(2):26174. Assessment of cognitive and motor deficits in a marmoset model of stroke. Marshall JW, and Ridley RM. ILAR J. 2003;44(2):153-60. A temporal MRI assessment of neuropathology after transient middle cerebral artery occlusion in the rat: correlations with behaviour. Virley et al. J Cereb Blood Flow Metab, 2000;20: 563-582. 2 Efficacy of a novel therapeutic agent on intraluminal thread middle cerebral artery occlusion (MCAo) model in rats SEVERE Severity This model aims to reproduce experimentally the focal cerebral ischemia that occurs in stroke, and has been extensively used to help understand the mechanisms of injury, to identify potential targets and to test putative neuroprotective agents. Strain differences in mice and rats have been identified, as well as the complex and significant influence of age, sex and co-morbidities such as diabetes, hypertension and atherosclerosis. Whereas preclinical stroke research often uses healthy male juvenile rodents, the impact of factors such as those mentioned above can be explored using models with co-morbid conditions (e.g. Spontaneous Hypertensive Rats, Streptocitozin (STZ)-induced diabetes in rats). In those cases, severity limits should be adapted accordingly, to capture the additional effects on animal welfare. In a standard study design, animals will be trained to perform certain behavioural/ cognitive tests and then undergo the MCAo procedure. During the therapeutic time window, established according to mechanism of drug action and objective of the study, animals will be given the test compound and the behavioural/cognitive tests will be repeated to monitor progress. In addition, infarct development can be followed using serial magnetic resonance imaging (MRI). What does this study involve doing to the animals? What will the animals experience? How much suffering might it cause? What might make it worse? Adverse effects Pre-operative training on These are behavioural observations, perform behavioural tests over a 2-3 voluntarily by the animals and will not cause weeks period: bilateral sticky pain, distress or lasting harm label test (for contralateral neglect), beam walking (for hindlimb coordination) and staircase test (for skilled forelimb paw-reaching) Food restriction (85-90% of Mild hunger free feeding weight) preoperatively and from 7 days post-MCAo to facilitate performance on staircase test How will suffering be reduced to a minimum Methodology and interventions Weight loss will not exceed 10%, otherwise food will be supplemented 3 End –Points Typically, a maximum time to perform the requested task is set, and a final score is given. Animals not reaching a baseline performance will be excluded from the study Transient (90 min) occlusion of the MCA (MCAo) using an intraluminal thread advanced via the common carotid artery Behavioural tests (bilateral sticky label test and beam walking test) undertaken daily from day 1 to day 28 post-MCAo Staircase test undertaken daily from day 7 post-MCAo Administration of test substance by s.c./i.v./i.p. route before and/or after surgery (prophylactic/therapeutic) Longitudinal MRI under anaesthesia on days 1, 7, 14 and 28 post-MCAo Pain and discomfort associated with surgery Effect of anaesthesia, and physiological variables (hypothermia, arterial blood pressure, arterial blood gases) on stroke outcome Poor nutritional intake resulting from reduced consciousness level, impaired mastication and poor motility, generally in the first 48h post MCAo Variable degree of locomotor deficit , having some temporary difficulties to move around in the cage Specific complications can occasionally occur, typically during the setting up of the model (subarachnoid haemorrhage, ipsilateral retinal injury, intraluminal thrombus formation, hypothalamus involvement with consequent hyperthermia or temporal muscle necrosis) NA Use of appropriate anaesthesics and analgesics (with no neuroprotective properties) Good surgical technique Well-trained surgeon Maintenance of homeostasis during anaesthesia Use of standardized monofilaments and surgical technique to reduce variability and complications derived from extensive lesions Regular body weight Daily observation and wound care Providing easy reached soft, tasty food and water during the recovery period, or hand feeding if necessary Rehydratation NA These are behavioural observations, perform voluntarily by the animals and will not cause pain, distress or lasting harm . Animals will be euthanized if any of the following specific complications occur: subarachnoid haemorrhage, ipsilateral retinal injury, intraluminal thrombus formation, hypothalamus involvement with consequent hyperthermia or temporal muscle necrosis Animals failing to fully recover from anaesthesia will be euthanised. Bodyweight loss exceeds 20% pre-surgical weight, despite hand feeding and /or rehydration. Animals unable to move for > 24 hours. Neurological score based on presence (score=2), moderate occurrence (score=1) or absence (score=0) of the following abnormal movements and postures: forelimbs and hindlimbs splitting, at rest or during movement, head tilting and reaction to visual stimulus. Typically, a maximum time to perform the requested task is set, and a final score is given. End- of the procedure Transient discomfort associated with administration route No adverse effect expected at the dose levels administered. Administration according to Good Practice Well defined therapeutic window according to objective of the study Repeated anaesthesia Effect of anaesthesia, and physiological variables (hypothermia, arterial blood pressure, arterial blood gases) on stroke outcome Use of appropriate anaesthesics and analgesics (without neuroprotective properties) Maintenance of homeostasis during anaesthesia 4 Animals failing to fully recover from anaesthesia will be euthanised Analysis This model is considered SEVERE because of the surgical procedure involved and the deleterious (but usually transient) effects of the MCA occlusion on the welfare of the animal, and the possibility of significant peri-operative complications From the experimental point of view, attention to refinement and standardization of each of the single procedures can lead to a reduced incidence of complications and variability, and consequently better quality of the data obtained and reduction of the number of animals used. A classification of SEVERE is therefore appropriate. Could the severity be MODERATE? Although initial severity of this model should always be SEVERE for the reasons outlined above, in the hands of experienced operators , together with veterinary supervision, and agreed early interventions if complications arise, could greatly contribute to a reduction of incidence of the severe effects discussed. MODERATE severity could be granted on a case by case basis to individual research groups with a proven track record of experience with this particular model. RETROSPECTIVE SEVERITY ASSESSMENT As described above 30 Male Sprague-Dawley rats (300-350g) underwent permanent MCAO using the intraluminal filament technique under general anaesthesia. Rats were randomized (n=10/ group) to receive either vehicle (10ml/kg) or a new test compound (compound A) at 1, 3, 10 mg/kg, infused intravenously into a tail vein over 1h beginning 30 min post- MCAO, subsequent doses (Compound A 1, 3, 10 mg/kg, or vehicle) were given intra-peritoneally at 6 and 24 h post MCAO. Functional outcome was assessed daily using a neurological scoring system (0-8), and in a series of behavioural tests carried out at 24, 48h and 7 days post MCAO. MRI was performed in anaesthetized rats on days 2 and 7, to assess lesion volume. All animals were euthanised after 7 days post MCAO. Prospective assessment of severity: SEVERE Results - Vehicle treated animals showed the lowest neurological score at 24, 48h and 7 days, and 1/10 had to be euthanised on day 2 post-surgery due body weight loss>20% (despite hand feeding and rehydration). Six further animals had a prolonged recovery time and required intensive care for 48 hours Retrospective assessment: SEVERE - 3/10 vehicle treated animals recovered reasonably well, with similar recovery to low-dose treated animals. Retrospective assessment: MODERATE - All compound A treated animals at lower doses (1 and 3 mg/kg) showed an improvement in neurological scoring by 48 h and 7 days post-MCAO, together with a reduction of lesion volume compared to controls at 7 days post-surgery. Retrospective assessment: MODERATE - Compound A treated animals at the highest dose (10 mg/ kg) showed improvement of neurological scoring compared with vehicle group from 24 hours post-MCAO, together with significant reduction of infarct size and only minimal (5%) body weight loss 24 hours post surgery. Retrospective assessment: MODERATE Neurological score based on presence (score=2), moderate occurrence (score=1) or absence (score=0) of the following abnormal movements and postures: forelimbs and hindlimbs splitting, at rest or during movement, head tilting and reaction to visual stimulus. Assessment of Actual Severity – 7 animals considered as SEVERE; 33 animals considered as MODERATE 5 b. Drug Dependence model in non-human primate Neuroscience models in NHP–Drug discrimination studies in non-human primates. Introduction Usually a drug will not be tested for dependence potential and/or abuse liability until other aspects of efficacy and safety have been demonstrated in a scientifically sound manner. At that point, a serious level of dependence potential and/or abuse liability can counterbalance the prospect for a modest therapeutic advance. Thus, screening for these effects may prevent the marketing of an undesirable new pharmaceutical agent. Associated with abuse liability are the subjective mood changes, the physical dependence (e.g.; anxiolytics, sedatives), dependence of centrally active stimulants (anorective agents, antidepressants) and the verification of the street-use of dissociative anaesthetics. Although drug addiction (s.a. morphine,) is a major issue in humans and a phenomenon which continues to be investigated in rodents, in the last decade, non-human primates are used far less in models that look for treatment of morphine withdrawal. Studies of drug discrimination, among others, are more humane as a model and equally useful in evaluating e.g. the similarity between morphine and other potential mu opioid agonists. Why then use non-human primates (NHP) in drug addiction research? These animals are very expensive to purchase and maintain, and well trained personnel are required to work with them. The most obvious reason is the same as that of the people who oppose this type of research: NHPs are more like humans than are rats, and it is for humans that this research is designed to understand and treat. Also NHPs respond to drugs in ways that are, or are likely to be, more like the human response than that of a rodent. This is particularly true of responses to opioid drugs. For example, whereas rodents have highly variable responses to agonists at the nociceptin/orphinan opioid receptor (NOP receptor), including a tendency to report that these agonists produce pain, NHP consistently indicate that NOP agonists are strong analgesics with very little in the way of side effects. It is safe to assume that humans will have responses to NOP agonists that are similar to those of the NHP, and this drug class may be the next generation of analgesics for treatment of moderate to severe pain. We would not know this if only rodents had been evaluated. The pituitary-adrenal axis response of NHPss to mu opioid agonists is more like the response of humans (inhibition) than of rodents (stimulation). The behavioural response of NHP to some kappa opioid agonists is more like that of humans (aversion) than of rodents (reinforcement). Most drugs are much more potent in NHP and humans than they are in rodents. The lethal dose of cocaine in a monkey e.g. is the dose of cocaine that is used to train a discriminative stimulus in rats (10 mg/kg). In other words, to notice an effect in rats, a dose of 10 mg/kg cocaine is needed, whereas this dose would kill a monkey or a human! This suggests very different physiological and pharmacological systems, and the NHP systems are much more similar to the human systems. Drugs which are abused by humans are also self-administered by both NHPs and rats, but most of these drugs appear to be much better re-enforcers in NHPs and humans than they are in rats. Rats are often food-deprived and trained to work for food before they are exposed to drug-maintained responding. They then acquire drug-taking responses over a period of several days or weeks. NHPs do not require this type of training. They readily acquire drug self-administration responses without any pre-training or long acquisition periods. NHP have much longer experimental lives than do rodents. This implicitly means that a single individual can be used over a period of many years as opposed to several months. The effects of long periods (i.e., months) of drug-taking, the duration of action of potential therapeutic agents, the effects of subtle changes in environmental stimuli, and the effects of drugs on cognitive skills are among the variables which can be more readily studied in non-human primates; much less well or less relevantly in rodents. In terms of tolerance, various behavioural factors have been shown to have important effects, among which is the presence or absence of a requirement for task performance while the subject is under the influence, the effect of the drug upon the relationship between the performance and its consequences, and the presence or absence of environmental stimuli linked by Pavlovian conditioning to the administration of the test agent (i.e. an animal will show more tolerance when tested in the same environment than when tested with the same dose in a new environment). This detailed description of these conditions are of paramount importance in the interpretation of results. 6 Cynomolgus monkeys are used as they are the most common NHP species used in toxicology studies and reference data are available. References Broadbear JH, Winger G, Woods JH (2004). Self-administration of fentanyl, cocaine and ketamine: effects on the pituitary-adrenal axis in rhesus monkeys. Psychopharmacology, 176, 398-406 Brady J.V. and S.E. Lucas (1984) Testing drugs for physical dependence potential and abuse liability. National Institute on drug abuse Research Monograph Series 52. Rockville MD. Department of Health and Human Services. Drug discrimination studies in non-human primates MODERATE Severity What does this study involve doing to the animals? Surgical implantation of chronic indwelling intravenous catheters, sequentially into internal and external veins (depending on the needs) and allowing for i.v. perfusion, injection or sampling Single housing to prevent problems with catheters Training for drug selfadministration in operant chambers What will the animals experience? How much suffering might it cause? What might make it worse? Adverse effects Pain and discomfort associated with surgery (pain, infection thrombi). How will suffering be reduced to a minimum Methodology and interventions Best Practice in anaesthesia, analgesia, post-operative care. Routine (frequent) care of catheter exit site, clinical examination at regular intervals, blood analysis to check for infection End –Points Infection which is unresponsive to antibiotic treatment without removal of the catheter; When catheter patency is lost in all accessible veins : animal will be removed from study Social isolation while still having visual, auditory and olfactory contact with same species and humans. Special jackets allowing free movement of the animal in the cage. Appropriate enrichment, interaction with caretakers and NHP in room Appropriate training Adapted chairs to minimize discomfort NA Moving NHP from cage to NHP training chair Restraint in chair during training session Possible adverse effects of drugs Rare because NHP usually do not overdose (they get nauseous before that or do not perform well enough (sedation) to obtain an additional injection (FR schedule). Anyway, to avoid overdose 7 Administration of appropriate antagonists or palliative treatment Self-administration in home cages Administration of pharmaceutical agent by the i.v. or i.m. route Chronic restraint using flexible tethers and jackets Possible adverse effects of agent under evaluation (very rare) Transient discomfort if associated with i.m. injection Accidental withdrawal syndrome if the test agent is an antagonist, overdosing if the test agent is an agonist the maximal number of self-injections is limited to four Gradual adaptation of NHP to the jacket and tether Administration of appropriate agonist or other drug Habituation to injections Animals are not allowed to take sufficient amounts of drug to produce robust physiological dependence. drug withdrawal signs do not develop Removed from study if refuses to eat when placed in a jacket or when access to veins is lost (thrombi, infection dislodgement) NA Catheter patency is lost in a physically dependent animal, thus withdrawal symptoms occur: remove temporarily from study and treat with appropriate dose of dependend drug Analysis There is no need to train monkeys with food prior to establishing self-administration of drugs such as cocaine or remifentanil. There is no need to deprive NHPs of food at any point in the study. In fact, they often need to be food-restricted to prevent obesity. Virtually all animals respond well for drugs such as cocaine or remifentanil. Therefore, veins that are available are catheterized during the experimental life of the animal. The catheters can remain in place and patent for many years, so animals can remain in the self-administration studies for 10 years or more. This means that a single animal can be involved in several experimental studies during its tenure in the laboratory. Nevertheless, the procedure is invasive, animals become dependent, and agents tested can provoke withdrawal symptoms, which can cause moderate discomfort A classification of MODERATE is therefore appropriate Could the severity limit be MILD? No, the animal will have undergone surgery for cannulation of veins, will become dependent on the drug and some form of abstinence may occur although animals are allowed self-injection daily throughout the study; this thus can induce moderate discomfort. Could the severity limit be SEVERE? Only in exceptional circumstances where overdosing would provoke unexpected toxic effects 8 RETROSPECTIVE SEVERITY ASSESSMENT Evaluation of the effects of a new pharmaceutical agent on cocaine self-administration in Rhesus monkeys. Six adult male Rhesus monkeys (Macaca mulatta) weighing between 9.9 and 15.4 kg were used in this study. Each subject had chronic indwelling catheters implanted under sterile conditions in the femoral, internal, or external jugular vein. The catheter passed subcutaneously to the animal’s back where it exited. The outer portion of the catheters was protected by a flexible stainless steel tether with one end attached to a double layer jacket worn by the NHP and the other bolted to the rear of the cage. Brief description of training and self-administration procedure: each cage had a panel with three stimulus lights: two red and one green light; placed above two response levers. The red light signaled drug availability. The green central light was illuminated for the duration of the drug injection or saline (during a 5 second period). During a time out, all stimulus lights were extinguished and responding had no programmed consequences. During the training, at first 0.03 mg/kg cocaine was ‘automatically’ injected and the green light signaled drug administration. Thereafter, through incidental touching of the lever, the animal provoked a new injection. During training animals were video-recorded to evaluate progress and possible clinical signs. Animals were trained quickly i.e. after a week all would lever press for cocaine injection. Animals were trained (twice daily, 7 days a week). to maintain their dependence, although signs of physical dependence were not seen. At each cage changes (every 2 weeks) a clinical check-up was performed, bodyweight was measured, rectal temperature was taken and catheters exit sites were checked and cleaned. Once a month, under ketamine sedation, jackets were replaced by clean ones. To avoid overdosing during the self-administration, animals were put on a Fixed Ratio schedule (FR), and either doses of cocaine injected were small, or the time out interval was prolonged (changing to Progressive Ratio was not indicated in this experiment for other reasons not evoked here). Data recoded were total responses/session, total injections/session, break point and intertrial interval. All subjects had an extensive cocaine self-administration history, and were maintained so through training sessions since over 2 years. Drug self-administration was scheduled twice daily for 130 min, starting at approximately 10 a.m. and 4 p.m. Depending on agents to be tested, the procedure would be classified as continuous use or reuse. Catheters were filled between sessions with a solution of 100 IU/ml heparin to prevent clotting at the catheter tip. The pharmaceutical agent tested to evaluate efficacy for drug abuse was injected 30 min before the self-administration procedure. As all animals had a stable rate of responding (in use since more than 2 years), and as toxicity information on the test agent were available, animals were randomly assigned to the high and low dose group. The procedure thus was classified as re-use. Whereas drug-dependent animals would, on a FR schedule, make2 responses per second when cocaine was available for responding, their response would drop to an average 0.1 response/second, upon ‘saline only’ availability, and ultimately they stopped performing. At high dose the pharmaceutical agent seemed effective, as responses for all animals present a right-shift of the cocaine behavior (increased response rate and frequency). This is similar to decreasing the dose of cocaine, which typically produces an increase in response rates and an increase in number of cocaine injections. Thus, a drug that produces an increase in cocaine-maintained responding has an ability to antagonize the reinforcing effects of cocaine. At the low dose the compound was deemed inefficacious, as no increase in cocaine self-administration was observed. The clinical score sheet identified sedation as only side effect at the very high dose. Prospective assessment of severity: MODERATE One animal had to be removed from the study when halfway in the re-use procedure; upon the clinical check-up it was noted that the catheter was getting clogged; physical examination revealed a minor weight loss and fever. The animal was pulled out of the study and given parenteral antibiotic treatment. When blood culture identified a Staphylococcus infection of the catheter, the animal was scheduled for surgery and the catheter removed. Fever dropped immediately and body weight gain was noted. 9 Following a negative blood culture, a new catheter was implanted in the contralateral vein, and the animal was again introduced into the study and allowed for completion of missing date. Retrospective assessment: MODERATE At no point the animals experienced pain or distress above the MODERATE level, as clinical observations allowed identification of problems related to the catheter use before, and information available on the test agent prevented exceeding a dose which would have provided side effects although at the highest dose tested a break point could be established. Continued use in these procedures is the usual way procedures are described within the project. However, upon specific request from authorities, it can occur that these very valuable and highly costly animals are used to evaluate the potential abuse liability of a new pharmaceutical agent with possible exceptional or dangerous addictive potential. In those cases, REUSE of these animals in procedures is deemed to be acceptable, as the part of the procedure which calls for a MODERATE classification is the surgery and possibly the drug dependence in severe cases, not the actual drug evaluated. The Re-use procedure thus is classified as MILD. 10