Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Embryogenesis and sexual
differentiation I and II
Dr. sc. nat.
Oliver Sterthaus
University Hospital Basel
Master Course in Toxicology
Section: Reproductive Toxicology
Swiss Center of Applied Human Toxicology
1
Embryogenesis and sexual
differentiation I
• Gametogenesis
• Fertilization
• Preimplantation
Embryogenesis and sexual differentiation II
•
Implantation
•
Embryonic disk
•
Embryonic phase
•
Fetal phase
Lecture from
http://www.embryology.ch
http://ivf-basel.ch/de/studenten/master-reproductive-toxicology/?L=0
2
Gametogenesis
•
•
•
•
•
The germline - origin of the germ cells
Determining the gender
Spermatogenesis
Oogenesis
Comparison of spermatogenesis with
oogenesis
3
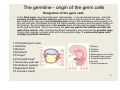
The germline - origin of the germ cells
Emigration of the germ cells
•
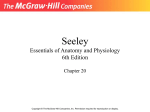
In the third week, the primordial germ cells wander - in an amoeboid manner - from the
primary ectoderm into the yolk sac wall and collect near the exit of the allantois. The
primordial germ cells are now extraembryonal, lying in the endoderm and mesoderm of
the yolk sac wall. Facilitated through the cranio-caudal curvature and the lateral folding of
the embryo, the primordial germ cells wander back into the embryo again between the
fourth and sixth week. They move along the yolk sac wall to the vitelline and into the
wall of the rectum. After crossing the dorsal mesentery they colonize the gonadal ridge.
During their journey, but also while still in the gonadal ridge, the primordial germ cells
multiply by mitotic divisions.
1 Primordial germ cells
2 Allantois
3 Rectum
4 Ectoderm
5 Foregut
6 Primordial heart
7 Secondary yolk sac
8 Endoderm (yellow)
9 Mesoderm (red)
10 Amniotic cavity
1 Rectum
2 Vitelline
3 Allantois
4 Nephrogenic cord (pink)
5 Gonadal ridge (green)
6 Primordial germ cells
(red dots)
7 Heart prominence
4
The germline - origin of the germ cells
•
•
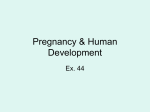
For both sexes the gonads arise in the gonadal ridges. These are bilateral, ridge-like protrusions
that appear ventromedially to the nephrogenic cord. They are generated in the 5th week through
the proliferation of the coelomic epithelium and the thickening of the underlying mesenchyma. At
this point, the gonadal ridge represents the primitive gonadal primordium. In order for this to
develop into the definitive and gender-specific gonads, the immigration of the primordial germ
cells is necessary.
In the 6th week, the primordial germ cells infiltrate into both gonadal ridges. The primordial germ
cells become surrounded by the coelomic epithelial cells that have proliferated and advanced
into the depths of the mesenchyma. These germinal cords are still connected with the surface of
the coelomic epithelium. At this point, the male and female gonadal primordia cannot be
distinguished and, for this reason, this condition is referred to as the indifferent gonadal
primordium.
1 Proliferating coelomic epithelium
2 Thickening of the mesenchyma
3 Germinal cords
4 Primordial germ cells (red dots)
5 Mesenchyma
6 Allantois
7 Vitelline
8 Intestinal tube
9 Dorsal mesentery
10 Gonadal ridge
11 Nephrogenic cord
12 Mesonephric (Wolffian) duct
13 Mesonephric tubule
14 Aorta
5
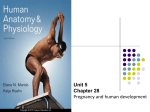
The germline - origin of the germ cells
6
http://www.rci.rutgers.edu/~uzwiak/EndoSpring10/Endo08_Lect16.htm
Determining the gender
Male gonadal primordium
•
The key to sexual differentiation lies on the Y chromosome in the SRY (sex
determining region of the Y chromosome). There the testis-determining factor (TDF)
is found that induces male development. Among other substances, testosterone is
formed beginning with the 7th week.
If no Y chromosome - and thus no SRY - is present, a feminine phenotype is
engendered.
7
Determining the gender
Female gonadal primordium
• The primary gonadal cords in the medullary region degenerate since
no SRY-gene exists in the female body. In the cortex region, on the
other hand, the proliferation of the coelomic epithelium remains
preserved - its cells surround the multiplying germinal cells. These
remain near the surface, however and, in contrast to the germinal
cords, are called cortical cords.
The cortical cords decay into isolated collections of cells and the
epithelial cells surround one to two primordial germ cells, forming
follicles. The primordial germ cells inside differentiate into oogonia
and, with the first meiotic division, become primary oocytes. The
interaction that then commences between primary oocytes with the
surrounding epithelial cells stops the completion of the first meiotic
division, which is then arrested until puberty begins.
8
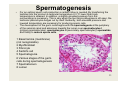
Spermatogenesis
9
Spermatogenesis
•
Spermatogenesis is initiated in the male testis with the beginning of puberty. This
comprises the entire development of the spermatogonia (former primordial germ
cells) up to sperm cells. The gonadal cords that are solid up till then in the juvenile
testis develop a lumen with the start of puberty. They then gradually transform
themselves into spermatic canals that eventually reach a length of roughly 50-60 cm.
They are termed convoluted seminiferous tubules (Tubuli seminiferi contorti) and
are so numerous and thin that in an adult male testicle their collective length can be
300 to 350 meters. They are coated by a germinal epithelium that exhibits two
differing cell populations: some are sustentacular cells (= Sertoli's cells) and the
great majority are the germ cells in various stages of division and differentiation.
10
Spermatogenesis
•
•
For an optimal sperm cell production a certain milieu is needed. By transferring the
testicles into the scrotum a testicular temperature 2-3 ºC lower than body
temperature is attained. In addition, a slightly elevated pressure from the
surroundings is necessary. This is why when the taut tunica albuginea is slit open, the
testicular parenchyma bulges out by itself. Evidently, both elevated pressure and
lowered temperature are necessary for producing sperm cells.
The development of the germ cells begins with the spermatogonia at the periphery
of the seminal canal and advances towards the lumen over spermatocytes I
(primary spermatocytes), spermatocytes II (secondary spermatocytes), spermatids
and finally to mature sperm cells.
1 Basal lamina (membrane)
(not recognizable)
2 Myofibroblast
3 Fibrocyte
4 Sertoli's cell
5 Spermatogonia
6 Various stages of the germ
cells during spermatogenesis
7 Spermatozoon
8 Lumen
11
Spermatogenesis
Developmental stages of spermatogenesis
http://scientopia.org/blogs/scicurious/2010/03/10/basics-guest-post-2spermatogenesis
12
Spermatogenesis
Spermiogenesis (spermatohistogenesis) and structure of the
sperm cell
1 Axonemal structure, first flagellar
primordium
2 Golgi complex
3 Acrosomal vesicle
4 Pair of centrioles (distal and
proximal)
5 Mitochondrion
6 Nucleus
7 Flagellar primordium
8 Microtubules
9 Sperm cells tail
10 Acrosomal cap
13
Spermatogenesis
1 Plasma membrane
2 Outer acrosomal membrane
3 Acrosome
4 Inner acrosomal membrane
5 Nucleus
6 Proximal centriole
7 Rest of the distal centriole
8 Thick outer longitudinal fibers
9 Mitochondrion
10 Axoneme
11 Anulus
12 Ring fibers
A Head
B Neck
C Mid piece
D Principal piece
E Endpiece
14
Spermatogenesis
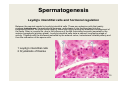
Leydig's interstitial cells and hormonal regulation
Between the seminal canals lie Leydig's interstitial cells. These are endocrine cells that mainly
produce testosterone, the male sexual hormone, and release it into the blood and into the
neighboring tissues. An initial active stage of these cells occurs during the embryonic development of
the testis. Later in juvenile life, due to the influence of the LH (luteinizing hormone) secreted by the
anterior hypophysis (pituitary gland), Leydig's interstitial cells enter a second, long lasting stage of
activity. Together with the hormones secreted by the adrenal cortex, testosterone initiates puberty and
thus the maturation of the sperm cells.
1 Leydig's interstitial cells
2 Crystalloids of Reinke
15
Oogenesis
Structure of the ovary
1 Primordial follicle
2 Primary follicle
3 Secondary follicle
4 Tertiary follicle
5 Antrum folliculi
6 Cumulus oophorus
16
Oogenesis
The follicle stages from primordial follicle to tertiary follicle
Primordial follicle
Secondary follicle
and Primary follicle
A Primordial follicle
B Primary follicle
1 Oocyte
2 Follicular epithelium
Tertiary follicle
1 Oocyte
2 Pellucid zone
3 Stratum granulosum
4 Theca folliculi cells
1 Oocyte
2 Pellucid zone
3 Stratum granulosum
4 Theca interna
5 Theca externa
6 Antral follicle
17
7 Cumulus oophorus (Granulosa cells, together with the oocyte)
8 Basal lamina between theca and stratum granulosum
Oogenesis
Temporal course of the number of germ cells / follicles
Phase A:
Primordial germ cells grow, proliferate and
become sheathed with coelomic epithelial
cells. Gonadal cords arise; 6th to 8th
week.
Phase B:
Spurt of growth: cellular clones of the
oogonia are formed, whereby the cells
remain connected with each other through
cellular bridges; 9th to the 22nd week.
Phase C:
The oogonia become primary oocytes
that enter the prophase of the first meiosis;
12th to the 25th week.
Phase D:
The primary oocytes become arrested in
the dictyotene stage of the prophase: the
primordial follicles are engendered; 16th
to the 29th week.
Phase E:
At around the 14th week a quantitatively
increased decline in the number of germ
cells commences as well as atresia in all
of the follicle stages.
18
Tabular comparison of
spermatogenesis and oogenesis
Spermatogenesis
Oogenesis
Number of gametes
Principle: continuous production.
Although from puberty to old age sperm
cells are constantly being engendered,
the production is subject to extreme
fluctuations regarding both quantity and
quality.
Principle: Using up the oocytes
generated before birth.
Continual decrease of the oocytes,
beginning with the fetal period.
Exhaustion of the supply at menopause.
Meiotic output
Four functioning, small (head 4 µm),
motile spermatozoids at the end of the
meiosis
One large, immotile oocyte (diameter
120 µm) and three shriveled polar bodies
are left at the end of the meiosis
Fetal period
No meiotic divisions
Entering into meiosis (arrested in the
dictyotene stage)
No germ cell production
Production of the entire supply of germ
19
cells
Fertilization
•
Ovulation
•
Getting the spermatozoa ready
-The path of the sperm cells to the oocyte – capacitation
-The sperm cells meet the oocyte - the acrosome reaction
•
The penetration of the spermatozoon into the oocyte
•
The fertilization is complete. The formation of the zygote
20
Ovulation
The female genital tract
1 Ovary
2 Infundibulum
3 Fimbriae
4 Fallopian or uterine tube
5 Ampullary part of the tube
6 Uterine musculature
7 Uterine mucosa
8 Cervix
9 Portio
10 Vagina
11 Ligamentum ovarii proprium
12 Suspensory ligament of the ovary
13 Ovary cut open (follicles in various stages)
21
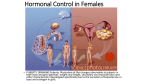
Ovulation
In the center of this hormonal control is
the hypothalamamics-hypophysial
(pituitary gland) system with the two
hypophysial gonadotropins FSH and
LH. The pulsating liberation of GnRH by
the hypothalamus is the fundamental
precondition for a normal control of the
cyclic ovarian function. This cyclic
activity releases FSH and LH, both of
which stimulate the maturation of the
follicles in the ovary and trigger
ovulation. During the ovarian cycle,
estrogen is produced by the theca
interna and follicular cells (in the socalled follicle phase) and progesterone
by the corpus luteum (so-called luteal
phase).
http://commons.wikimedia.org/wiki/File:MenstrualCycle.png
22
Ovulation
Maturation of the oocyte in the dominant follicle shortly before ovulation
1 Theca interna and externa
2 Basal membrane between theca
and granulosa
3 Granulosa
4 Graafian follicle with follicle fluid
5 Primary oocyte
6 Cumulus oophorus
7 Ovarian tissue
8 Tunica albuginea of the ovary
9 Abdominal space
10 Pellucid zone
11 Nucleus in the diakinesis stage
12 Granulosa cells
13 Processes of the granulosa
cells
14 Microvilli of the oocyte surface
23
Ovulation
Termination of the first meiosis
1 Pellucid zone
2 Perivitelline space
3 Spindle apparatus in the anaphase
of the first meiosis
4 Granulosa cells retract their cell
processes
5 Microvilli of the oocyte surface
6 Granulosa cells
7 Polar body
24
Ovulation
The follicle that is
about to rupture
1 Peritoneal cavity
2 Follicle about to rupture
with follicle fluid (containing lots
of hyaluronic acid and progesterone)
3 Cloud of cumulus cells with oocyte
4 Loosened-up cumulus cells
5 Secondary oocyte
6 Corona radiata
7 Ovarian tissue
1 Spindle apparatus with
chromosomes that form the
metaphase plate
2 Arrested spindle apparatus in
the polar body
3 Perivitelline space
25
Ovulation
1 Fallopian tube cut open with the tube mucosa that lies in folds
2 Closely apposed fimbriae
3 Follicle fluid that has flowed out
4 Secondary oocyte with corona radiata
5 Ovary with follicles in various stages of development and atresia
6 Pellucid zone
7 First polar body
8 Secondary oocyte
9 Cells of the corona radiata
10 Arrested spindle apparatus
The oocyte now "waits" in the fallopian tube on fertilization by the sperm. The matrix of hyaluronic acid holds
it "captive" there, so to speak. After a number of hours the matrix liquefies more and more and the oocyte is
gradually transported towards the uterus by the ciliary beats of the tube's epithelium cells. Since after
ovulation the oocyte can only be fertilized within a few hours, the fertilization must almost inevitably take
place in the ampullary part of the fallopian tube.
26
Ovulation
27
27
Ovulation
28
Getting the spermatozoa ready
29
Getting the spermatozoa
ready
Spermatozoa maturation steps
1 Tail
2 Head
3 Acrosome
The maturation and activation of the spermatozoa occur in the following four steps:
Storage in the epididymis
Ejaculation
Ascension to the ovary
Near the oocyte
Maturation
Activation
Capacitation
Acrosome reaction
30
The ejaculation and the ejaculate
1 Testicle
1a Efferent ductules of the testis
2 Ductus epididymidis
2a Cauda epididymidis
3 Deferent duct / vas deferens
4 Ampulla of the deferens duct
5 Glandula vesiculosa / Seminal
gland
6 Ejaculatory duct
7 Prostate gland
8 excretory duct of the prostate
9 Bulbourethral gland
(Cowper's gland)
10 Urethral gland
(Littre's gland)
11 Urethra
The ejaculation is brought about through rhythmic contractions of the deferent duct that come in waves and
through supporting contractions of the pelvic musculature.
The purpose of the coital ejaculation is to deposit spermatozoa, which are largely immobile having come from
storage in the cauda of the epididymis, into the rear part of the vaginal cavity, i.e., near the external opening
of the cervix, the entrance to the uterus.
While the spermatozoa are pushed through the deferent duct and the urethra, a large volume of secretions of
various glands are mixed in. This fluid part of the ejaculate is known as the seminal plasma.
The ejaculate thus consists of up to 10% spermatozoa and 90% seminal plasma for a total volume of 2-6 ml.
31
Getting the spermatozoa
ready
The seminal plasma
The seminal plasma mediates the chemical function of the ejaculate.The mixing together of
the various glandular fractions leads to a coagulation of the fresh ejaculate in the rear
vaginal cavity within a minute. In this way a deposit of spermatozoa is formed in the vagina.
After about 15-20 minutes the coagulated ejaculate becomes a fluid again.
Due to its slight alkalinity (light alkaline buffer) it is also responsible for creating a milieu
beneficial for the spermatozoa in a vaginal surrounding that is normally maintained acidic.
The seminal plasma has to fulfil the following tasks:
Creation of an alkaline buffered milieu in the vagina
Coagulation of the ejaculate and creating a sperm deposit in the vagina
Coating the sperm cells with capacitation inhibitors
Activation and augmenting the motility of the sperm cells
Supplying nutrients for the sperm cells
Fluidizing the ejaculate after 15-20 minutes
32
The path of the sperm cells to
the oocyte - capacitation
33
The path of the sperm cells to
the oocyte - capacitation
1 Rear part of the vaginal cavity
2 Portio / cervix
3 Cervix canal
4 Isthmus
5 Ampullary part of the fallopian tube (ampulla)
6 Ovary with attached Fimbriae
7 Endometrium
8 Myometrium
9 Cavum uteri
10 Meeting place of the sperm cells with the oocyte
In order, though, that a sufficient number of sperm cells appear in the ampulla at the right time, a
large number of sperm cells must be present in the ejaculate. Of the roughly 200 million ejaculated
sperm cells only a few hundred are able to traverse the long way through the cervix, the uterus, and
past the fallopian tube isthmus to the tube's ampullary region to there meet oocyte.
Along the way whole groups of sperm cells can halt at certain places and enter a phase of reduced
activity. That is why a portion of the sperm cells can retain their fertilizing capability for up to 4 days.
34
The path of the sperm cells to
the oocyte - capacitation
The cervical canal
1 Sperm cells
2 Mucus fibers (strongly
meshed)
3 Crypt of a cervix gland
4 Mucus fibers (loosely meshed)
5 Portio entrance
Before the ovulation the cervical canal is narrow and the cervix mucus is strongly meshed (it forms
the so-called cervical barrier) that hinders the passage of sperm cells.
At the time of ovulation the cervix wall becomes looser and the canal wide. The folds of the mucosa
increase in number and let deeper and branched crypts come into being; there are then also more
cervix glands.
Under the influence of the estradiol that increases shortly before ovulation the cervix mucus is
restructured and the mucus barrier becomes passable for sperm cells.
35
The path of the sperm cells to
the oocyte - capacitation
• Capacitation is a functional maturation of the spermatozoon.
The changes take place via the sperm cell membrane in which it
may be that receptors are made available through the removal of a
glycoprotein layer. The area of the acrosomal cap is also so altered
thereby that the acrosome reaction becomes possible.
Through the membrane alterations, the motile properties of the
spermatozoon also change. Discharging whipping movements of
the tail together with larger sideways swinging movements of the
head take place. This type of motility is designated as hyperactivity.
One can therefore say that the visible consequences of capacitation
consist in hyperactivity of the spermatozoon.
• Since it cannot be determined ahead of time when the exact
moment is that the oocyte and spermatozoon will meet, the
maturation mechanisms are so configured that various groups of
sperm cells are able to keep their chances of fertilization upright
over a relatively long time after cohabitation. For this purpose the
ejaculated sperm cells do not all end their capacitation at the same
time, thus creating heterogenous groups of sperm cells.
36
The sperm cells meet the oocyte the acrosome reaction
37
The sperm cells meet the oocyte the acrosome reaction
Penetrating the cumulus cells
1 Center of the oocyte
2 Corona radiata (surrounds and
partly covers the oocyte)
3 Head of the spermatozoon
Normally, the acrosome reaction of the spermatozoa takes place first when they
encounter the pellucid zone. In a small percentage of the sperm cells, though, the
acrosome reaction occurs spontaneously, just as when a small percentage of the
cells experience capacitation immediately following ejaculation. This circumstance
assures that a small amount of hyaluronidase is present from the very beginning
and, when the wave of sperm cells meets the oocyte, a few of them are thus assisted
in making their way to the pellucid zone. Upon arriving at the pellucid zone, these
sperm cells themselves undergo an acrosome reaction and a further amount of
hyaluronidase and other enzymes are released. In this way, the throng of cumulus
cells is further loosened up and more and more sperm cells obtain the possibility38of
undergoing the acrosome reaction themselves at the pellucid zone.
The sperm cells meet the oocyte the acrosome reaction
The contact with the pellucid zone
1 Pores
2 Emerging of the acrosomal contents
3 Inner acrosomal membrane
4 Acrosomal content (enzyme)
5 Outer acrosomal membrane
6 Cell membrane
7 Membrane residues dropping behind
8 Post-acrosomal membrane region
A Head
B Neck
C Mid-piece
A prerequisite for the success of the acrosome reaction
is the previous binding of the spermatozoon to the
pellucid zone.
The enzymes that are released in the immediate vicinity
of the pellucid zone by the acrosome reaction dissolve it
locally and thus create a way through it for the sperm
cells. A number of enzymes that have been released
are involved. The best known are the already mentioned
hyaluronidase and acrosin, whereby the acrosin
makes it possible for the spermatozoa to get through the
pellucid zone.
39
The penetration of the
spermatozoon into the oocyte
40
The penetration of the
spermatozoon into the oocyte
The docking mechanism of the spermatozoon onto the
oocyte (the key-lock principle)
1 Post-acrosomal region
2 Oolemma with microvilli
3 Perivitelline space
4 Pellucid zone
5 Cortical vesicle at the
surface of the oocyte
The docking triggers a cascade of events with the
following goals:
-Polyspermy block: The penetration of further sperm cells
should be hindered
-Hardening of the pellucid zone as a mechanical
protection of the embryo
-Entry of the spermatozoon into the oocyte
Termination of the 2nd meiosis of the oocyte with
expulsion of the 2nd polar body
-Preparation at the molecular level of the oocyte for
unpacking the paternal DNA
41
The penetration of the
spermatozoon into the oocyte
The polyspermy block
1 Pellucid zone
2 Perivitelline space
3 Cortical vesicle
4 Oolemma
The docking triggers a rapid wave of depolarization in the oolemma, leading
to changes in the membrane surface.
The depolarization wave then also causes small cortical vesicles, found on
the inside of the oolemma, to empty out their contents into the perivitelline
space
The entry of the spermatozoon into the
oocyte (impregnation)
1 Oolemma
2 Cell membrane of the
spermatozoon
3 Kinocilium
4 Nucleus (compact) of the spermatozoon
5 Centrosome of the spermatozoon
The genetic material, lying in the nucleus and coming from the father, is unpacked and is used for building the
paternal pronucleus. In what follows, the centrosome plays an important role in the convergence of the two
pronuclei. Later - after the subsequent division - it will also be responsible for building the first division spindle of the
new creature. All centrosomes in the bodily cells of a human originate from that of the father.
Other sperm components transferred to the oocyte cytoplasm, like the kinocilium, are dissolved. Effective processes
also exist for eliminating sperm mitochondria from the cytoplasm of the oocyte.
Thus, all mitochondria in the bodily cells of an individual normally derive from the mother alone
42
The penetration of the
spermatozoon into the oocyte
The termination of the second meiosis of the oocyte
1 Mitotic spindle with chromatids
2 1rst polar body
3 Pellucid zone
4 Perivitelline space
5 Cell membrane of the
spermatozoon
(Remainder as appendage)
6 Kinocilium
7 Nucleus (compact) of the
spermatozoon
8 Proximal centrosome of the
spermatozoon
1 1rst polar body
2 Nucleus (slightly unpacked) of the
spermatozoon
3 Proximal centrosome of the
spermatozoon
4 2nd polar body (being formed)
5 Remainder of the mitotic spindle
with maternal chromosomes 1n,1C
The termination of the second meiosis implies the division of the secondary oocyte (1n,2C) into a mature oocyte (1n,1C)
43
by the expulsion of the 2nd polar body (1n,1C) into the perivitelline space.
In vitro fertilisation
44
The fertilization is complete.
The formation of the zygote
45
The fertilization is complete.
The formation of the zygote
Introduction into the creation and development of the pronuclei
1 Paternal pronucleus
2 Maternal pronucleus
3 Centrosome brought in by
the spermatozoon
4 Group of polar bodies
The maternal pronucleus is next to the polar bodies. The paternal one forms
near where the sperm cell entered and is almost always some distance from
the polar bodies.
46
The fertilization is complete.
The formation of the zygote
Approach of the pronuclei
1 Paternal pronucleus
2 Maternal pronucleus
3 Paternal centrosome
4 "Inner bodies"
5 Maternal astral microtubule
47
The fertilization is complete.
The formation of the zygote
The formation of the zygote
1 Nucleic membranes of the
pronuclei, as they are dissolving
2 Microtubules of the mitotic spindle
After the two pronuclei have come as close
together as they can, no merging of them takes
place, i.e., a fitting together of the chromosomes
of the two pronuclei within a single nucleic
membrane does not happen. It is much more
accurate to say that the nucleic membranes of
both pronuclei dissolve and the chromosomes of
both align themselves on the spindle apparatus at
the equator.
48
Preimplantation
• The cleavage divisions and the migration
of the embryo through the tube
49
Preimplantation
The cleavage divisions and the migration of the embryo through the tube
The cleavage divisions up to the morula stage
50
Preimplantation
51
Preimplantation
How a blastocyst is engendered
1 Embryoblast
2 Pellucid zone
3 Trophoblast
4 Blastocyst cavity
Around the end of the fifth day the embryo frees itself from the enveloping
pellucid zone. Through a series of expansion-contraction cycles the embryo
bursts the covering. This is supported by enzymes that dissolve the pellucid
zone at the abembryonic pole. The rhythmic expansions and contractions
result in the embryo bulging out of and emerging from the rigid envelope. This
"first birth" is called hatching
52
Preimplantation
53
Preimplantation
Blastocyst morphology
Proposal for a universal minimum
information convention for the
reporting on the derivation of human
embryonic stem cell lines.
Stephenson EL, Braude PR, Mason C.
Regen Med. 2006 Nov;1(6):739-50.
54
Preimplantation
The emergence of the blastocyst (hatching)
1 Pellucid zone
2 Trophoblast (outer cell mass)
3 Hypoblast (part of the inner cell
mass)
4 Blastocyst cavity
5 Epiblast (part of the inner cell mass)
55
Preimplantation
The migration of the embryo through the fallopian tube
1 Ovary
2 Fallopian tube
3 Endometrium
4 Myometrium
5 Uterine cavity
A Spermatozoon penetrates into
the oocyte (conception), day 0
B Two-cell stage, day 1
C Four-cell stage, day 2
D Eight-cell stage, day 3
E Morula (16-32 cells), day 4
F Free blastocyst (following
hatching), day 6
56
Embryogenesis and sexual
differentiation II
• Implantation
• Embryonic disk
• Embryonic phase
• Fetal phase
57
Implantation
• Role and functional anatomy of the
endometrium
• Implantation stages
58
Role and functional anatomy of the
endometrium
1 Single-layered prismatic
2 epithelium
3 Basal lamina
4 Uterine glands (glandulae uterinae)
5 Connective tissue
6 Blood vessels
A Superficial, functional layer
B Basal layer
C Myometrium
Endometrial functions
-Cyclic alterations of the uterine glands and blood vessels during the course of
the menstruation, as preparation for the implantation
-Location where the blastocyst is normally implanted
-Location where the placenta develops
59
Role and functional anatomy of the
endometrium
Cyclic hormonal alterations of the endometrium
The menstruation phase
A Functional layer
B Basal layer
C Myometrium
1 Uterine cavity with epithelial cells, blood
corpuscles and remainders of the expulsed mucosa
2 Intact and partially expulsed uterine glands
3 Intact epithelial cells
4 Basal membrane
5 Uterine stroma
6 Blood corpuscles
7 Free cells of the connective tissue
The menstruation phase (1st to the 4th day) distinguishes the beginning of each
menstruation cycle. When an implantation does not occur, the back-formation of
the yellow body (corpus luteum) lowers the amounts of circulating estradiol and
progesterone hormones, which leads to the expulsion of the functional layer of the
60
endometrium.
Role and functional anatomy of the
endometrium
The follicular or proliferative phase
1 Glandular epithelium
2 Endometrium that is a little
developed
3 Uterine glands
4 Myometrium
5 Stroma of the endometrium
6 Epithelial cells of the uterine glands
1 Glandular epithelium
2 Endometrium during the
proliferation
3 Uterine glands
4 Myometrium
5 Stroma of the endometrium
(mitosis)
6 Epithelial uterine gland cells with mitotic figures
During the proliferative or follicular phase (4th to 14th day) the secretion of estrogen through the growing ovarian follicle
is responsible for the proliferation of the endometrium (intensive mitosis in the glandular epithelium and in the stroma).
The uterus epithelium clothes the surface again. In this stage a certain number of epithelial cells equipped with cilia can be
recognized.
The glands grow longer and the spiral arteries wind themselves lightly into the stroma. At the end of the proliferative phase the
estradiol peak (released by the growing follicles) triggers a positive feedback mechanism at the level of the pituitary and the
ovulation commences 35 to 44 hours after the initial LH increase (cyclic hormonal changes).
61
Role and functional anatomy of the
endometrium
The luteinizing or secretory phase
1 Glandular epithelium
2 Thickened endometrium
3 Uterine glands, curled
4 Myometrium
5 Stroma of the endometrium
6 Epithelial uterine gland cells with
glycogen collections at the basal
pole
1 Glandular epithelium
2a Stratum compactum
2b Stratum spongiosum
2c Stratum basale
3 Curled uterine glands
4 Myometrium
5 Stroma of the endometrium
6 Epithelial cells of the uterine glands with
glycogen collections at the apical pole
NB 2a + 2b = Stratum functionale
During the secretory or luteinizing phase (14th to 28th day) the endometrium differentiates itself due
to the influence of progesterone (from the corpus luteum) and attains its full maturity. The glands and
arteries begin to entwine. The connective tissue stroma becomes the place of edematous changes.
62
The time period of the maximal reception ability for the blastocyst lies between the 20th and the 23rd
day. This phase of the endometrium lasts 4 days and is usually termed the "implantation window" .
Role and functional anatomy of the
endometrium
Normal implantation zone
1 Uterine cavity
2 Isthmus of the tube
3 Uterine tube (tuba uterina)
4 Uterine cervix (cervix uteri)
In order that implantation can take its normal course, the blastocysts and the
uterine mucosa must be able to interact. These two, independent structures must,
therefore, undergo synchronous changes. The implantation normally takes place in
the superior and posterior walls of the uterine body (corpus uteri) in the functional
layer of the endometrium during the secretory phase of the cycle.
extra-uterine pregnancy
Placenta praevia
63
Role and functional anatomy of the
endometrium
Adhesion of the blastocyst to the endometrium
A Menstruation
B Proliferation
C Secretion
D Implantation window
After the apposition of the free blastocyst at the
uterine epithelium the microvilli on the surface of
the outermost trophoblast cells interact with the
epithelial cells of the uterus. In this stage the
blastocyst can no longer be eliminated by a
simple flushing out. The adhesion of the blastocyst
on the endometrium arises through cell surface
glycoproteins, the specific mechanisms of which,
though, are not yet well understood.
64
Implantation stages
65
Implantation stages
1 Syncytiotrophoblast (ST)
2 Cytotrophoblast (CT)
3 Epiblast
4 Hypoblast
5 Blastocyst cavity
6 Maternal blood capillary
7 Amniotic cavity
8 Amnioblasts
9 Fibrin plug
10 Trophoblast lacunae
11 Multiplying hypoblast
1 Epithelium of the uterine mucosa
2 Hypoblast
3 Syncytiotrophoblast
4 Cytotrophoblast
5 Epiblast
6 Blastocyst cavity
1 Hypoblast growing ventrally
2 Eroded maternal capillaries
3 Extraembryonic reticulum
4 Heuser´s membrane
5 Amniotic cavity
6 Cytotrophoblast
7 Syncytiotrophoblast
8 Lacunae, filled with blood
In the periphery the syncytiotrophoblast forms a syncytium, i.e., a multi-nucleic layer without cell
boundaries that arises from the fusion of cytotrophoblast cells. The syncytiotrophoblast produces lytic
enzymes and secretes factors that cause apoptosis of the endometrial epithelial cells. The
syncytiotrophoblast also crosses the basal lamina and penetrates into the stroma.
Numerous "implantation factors" are known:
Interleukin 1 (IL-1), the inhibition factor for leukocytes (LIF), the colony-stimulating factor (CSF), as well
as the epithelial growth factor (EGF) and its receptors (EGF-R).
66
Embryonic disk
• The bilaminar germ disk (2nd week)
• The trilaminar germ disk (3rd week)
67
Embryonic disk
Development during the 2nd embryonic week
1 Extraembryonic mesoblast
2 Amniotic cavity
3 Primary umbilical vesicle
In the bilaminar primordium of the embryo (hypoblast or primary endoderm and epiblast) one recognizes in the epithelium
of the epiblast a fluid-filled space, the first primordium of the amniotic cavity.
Ventrally, the roof of the still incompletely uncovered primary umbilical vesicle (previously the blastocyst cavity) is
formed by the hypoblast.
Schematically, amniotic cavity and primary umbilical vesicle together form two hemispheres with two layers (epi- and hypoblast)
lying close to one another, thus representing the first embryonic primordium.
However, only the epiblast is responsible for forming the embryo. The hypoblast develops into a part of the extraembryonic
appendages.
68
Embryonic disk
The trilaminar germ disk (3rd week)
Formation of the primitive streak
1 Primitive groove
2 Primitive pit
3 Primitive node
4 Oropharyngeal membrane
5 Cardial plate
6 Sectional edge of amniotic membrane
7 Mesoderm
8 Endoderm
9 Future cloacal membrane
1+2+3 primitive streak
Primitive groove
2 Epiblast
3 Extraembryonic mesoblast
4 Definitive endoblast
5 Invading epiblastic cells forming
the intraembryonic mesoblast
6 Hypoblast
The bilaminar germ disk differentiates itself further into a trilaminar embryo, in that the cells flow in over
the primitive streak between the two already existing germinal layers and so form the third embryonic
germinal layer (mesoblast/derm). This phenomenon is also termed epithelio-mesenchymal transition
(gastrulation in lower vertebrates). During this period the embryo experiences profound alterations.
Afterwards, one speaks of the dorsally lying ectoblast/derm (and no longer of an epiblast/derm),
from intermediate mesoblast/derm, as well as from ventrally lying endoblast/derm, which replaces the
hypoblast. In order to have a better overview, the developments of the third week should be divided into 69
several phases. One must keep in mind, though, that these do not always follow each other - they can
just as easily take place concurrently.
Embryonic disk
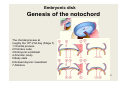
Genesis of the notochord
The chordal process at
roughly the 19th-21st day (Stage 7)
1 Chordal process
2 Primitive node
3 Embryonic endoblast
4 Amniotic cavity
5 Body stalk
6 Extraembryonic mesoblast
7 Allantois
70
Embryonic disk
The chordal process at roughly the 23rd day (Stage 8)
1 Fused chordal process
2 Prechordal plate
3 Pharyngeal membrane
4 Embryonic endoblast
5 Amniotic cavity
6 Neural groove
7 Canalis neurentericus
8 Intraembryonic mesoblast
9 Cloacal membrane
10 Umbilical vesicle
11 Allantois
71
Embryonic disk
The chordal process at roughly the 25-28th day (Stage 9-10)
1 Chordal process
2 Embryonic endoderm
3 Amniotic cavity
4 Neural groove
5 Body stalk
6 Intraembryonic mesoblast
7 Prechordal plate
8 Pharyngeal membrane
9 Cloacal membrane
10 Aortae
11 Umbilical veins
12 Cardiogenic plate
13 Allantois
Summary:
the notochord determines the longitudinal axis of the embryo. It defines the future
situation of the vertebral body and induces the ectoblast in its differentiation to 72
become the neural plate.
Embryonic disk
Location of the epiblast cell target and the development of the
primitive streak
Dorsal view of the primitive
1 Primitive streak
streak at around the 17th day
2 Prechordal plate
3 Primitive node
4 Neural plate
5 Cloacal membrane
6 Chordal process
1 Primitive streak
2 Primitive node
3 Neural tube
4 Cloacal membrane
5 Prechordal plate
6 Chordal process
21st day
19th day
23rd day
73
Embryonic disk
Induction of the neural plate - neurulation
Neural plate: 19 – 23rd day
Neural plate at roughly
the 25th day
1 Neural plate
2 Primitive streak
3 Primitive nodes
4 Neural groove
5 Somites
6 Cut section of the amnion
7 Neural folds
The neural tube at roughly The neural tube at roughly
the 29th day
the 28th day
1 Neural tube
2 Neural fold
3 Neural groove
4 Somites
5 Neural crest
6 Protrusion of the pericardium
7 Cranial neuropore
74
8 Caudal neuropore
Embryonic disk
The forming neural crest (neural plate stage)
A Neural plate stage
B Neural groove stage
1 Epiblast
2 Neural groove
3 Neural crest
Migrating neural crest cells
(neural groove stage)
Neural crest after
a completed detachment
(neural tube stage)
1 Epiblast
2 Neural fold
3 Migrating neural
crest cells
4 Neuroepithelium
5 Central canal
6 Neural tube
75
Development of the umbilical
cord
Body stalk at around the 3rd week
Formation of the umbilical cord at
around the 3.5th week
A Body stalk
B Stem of umbilical vesicle
C Umbilical cord
1 Amniotic cavity
2 Umbilical vesicle
3 Chorionic cavity
4 Villous chorion
5 Allantois
The body stalk and the yolk stalk are now united
and form the umbilical cord. Through increasing
secretion of amniotic fluid the chorionic cavity
becomes obliterated. Here at around the 4.5th
week: The chorionic cavity is reduced in size
Flexing of the embryo at around the 8th
week with expansion of the amnion that
encircles the body stalk and the ductus
omphalo-entericus, the umbilical coelom
and the umbilical vessels
76
Embryonic phase
• The Carnegie stages
• Congenital abnormalities
• Embryopathies
77
The Carnegie stages
The embryo can be classified according to its age, its size or its morphologic characteristics.
The correlation between these three criterias will allow identifying the embryonic Carnegie
stages.
This separation into stages was originally developed by Streeter (1942) who termed the various
organizational stages "horizons". Later this scheme was completed by O'Rahilly and Müller
(1987) who spoke more simply of embryonic stages or Carnegie stages.
Taking into consideration various external and internal landmarks of embryonic development, it
was decided to divide the 8 embryonic weeks (56 days) into 23 Carnegie stages.
The fetal period that begins after the 8th week is characterized by the growth and maturation
of the organs. The inner and outer morphologic alterations are less noticeable. For this reason
78
one no longer divides the fetal period into Carnegie stages.
The Carnegie stages
Stage 1
Approx.
1rst day
0.1 0.15
mm
1 Male pronucleus
2 Female pronucleus
3 Doubled paternal centrosome
4 "Inner bodies"
Stage 11
Approx.
29th day
2.5 4.5
mm
1 Neural tube
2 Caudal neuropore
3 Rostral neuropore that is just closing
4 Somites
5 2. pharyngeal arch
6 1. pharyngeal arch
Stage 22
Approx.
53rd day
23 28
mm
1 Umbilical cord with physiologic hernia
2 Nose
3 Subcutaneous vessel network of the head
4 Ear
5 Elbow
6 Pronation of the hands
7 Knee
8 Supination of the feet
9 Well-developed toes
10 Remainder of the embryonic tail
79
Inherited or congenital
abnormalities
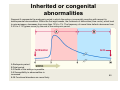
Segment A represents the embryonic period in which the embryo is especially sensitive with respect to
developmental abnormalities. Within the first eight weeks, the incidence of deformities (blue curve), which lead
to miscarrieages, decreases from more than 10% to 1%. The frequency of neural tube defects decreases from
2.5% to 0.1% (green curve) by the end of the embryonic period.
A Embryonic period
B Fetal period
0-3 Death of the embryo is possible
3-8 Susceptibility to abnormalities is
increased
8-38 Functional disorders are more likely
80
Classification of the congenital
abnormalities
•Primary abnormality:
Defect (genetic anomaly) in the structure of an organ or a part of an organ that can be traced back to an anomaly in its development
(spina bifida, cleft lip, congenital heart defect).
•Secondary abnormality ("disruption"):
Interruption of the normal development of an organ that can be traced back to outer influences. Either teratogenic agents
(infection, chemical substance, ionizing radiation) or a trauma (amniotic bands, which led to an amputation) are involved.
The most widespread infectious agents are the rubella virus, the cytomegaly virus and the toxoplasmosis parasite (toxoplasma
gondii). To the chemical, teratogenic agents belong thalidomide, warfarin, chloroquine (malaria medicine) and lithium.
It is important to understand that a congenital abnormality is not necessarily inherited.
•Deformation:
Anomalies that occur due to outer mechanical effects on existing normal organs or structures.
•Dysplasia:
Abnormal organization of the cells in a tissue (e.g., osteogenesis imperfecta). Numerous dysplasias are genetically caused (e.g.,
achondroplasia).
•Agenesia:
The absence of an organ due to a development that failed to happen during the embryonic period.
•Sequence:
When one, single factor results in numerous secondary effects, leading to several anomalies, one speaks of a sequence (e.g.,
Potter's sequence: not enough amniotic fluid because urine was not produced in large enough quantities. This leads to an
oligoamnios. The fetus is crushed, the face is contused, the hips are shifted, and the lungs are smaller than normal [hypoplasia]).
•Syndrome:
A syndrome comprises a group of anomalies that can be traced to a common origin (Down syndrome occurs due to a trisomia of the
21rst chromosome and leads to a number of characteristic anomalies).
81
Primary abnormalities
•Gene aberrations:
Gene aberrations account for roughly 7.5% of congenital abnormalities. Either
monogenetic mutations or polygenetic mutations are involved that can be
further inherited in accordance with Mendel's laws.
•Chromosomal aberrations:
•One also distinguishes here two kinds: structural and quantity aberrations.
They comprise roughly 0.5 % of the congenital abnormalities.
•Multifactorial anomalies:
They can be traced back to several genes and can be influenced by
environmental factors (medications, chemical products). To this group belong all
abnormalities of the neural tube, harelips and cleft palates, as well as cardiaccirculation-disorders, dysplasia of the hips, and cryptorchism.
82
Secondary abnormalities
-They are due to the influence of teratogenic factors on an individual who was originally normal.
Secondary abnormalities depend on the health of the mother, on the moment at which the
violation occurred, on the nature of the responsible agent and on the genetic predisposition of the
child.
- There are numerous teratogenic factors that can be put into the following order:
Infectious agents
Medications, hormones and chemical products
Physical agents (ionizing radiation)
Other factors (metabolites, toxic substances)
- Teratology (teras: monster) is concerned with congenital abnormalities.
Teratogenesis is the area of embryology that studies the causes, the mechanisms and the
models of developmental anomalies. One of the concepts of teratogenesis is that certain periods
during the development are more susceptible to teratogenic agents than others.
In order to examine a potentially teratogenic substance one has to pay attention to several points:
The vulnerable phase of the forming organ
The dose of the teratogenic substance and how it is applied
The genotype of the embryo
The environment
- Studies of potentially teratogenic substances can be performed in two ways. In the first
method epidemiologic criteria are involved. Here one examines the relationship between the
frequency of the anomalies that occur and a prenatal exposure to an agent.
As an alternative, based on animal experiments, substances can also be tested concerning their
teratogenic potential. The results cannot, though, always be transferred to humans directly (e.g.,
thalidomide). The examination of the teratogenic potential of a substance is made more difficult by
the fact that most congenital abnormalities are multifactorial. For the resulting pathology the
genetic structure of the individual also plays an important role.This is why a teratogenic substance
can have catastrophic consequences for one individual while for another there are no effects.
83
Viral pathogens
•
•
•
•
•
Rubella virus:
The rubella virus (that causes German measles) is a typical example of a teratogenic pathogen.
When the mother is infected the virus can pass through the placental barrier thereby infecting the embryo or the
fetus. It is thus very important to vaccinate women during childbearing years.
During the first trimester the danger of anomalies due to infection in the first month amounts to roughly 50%, but
decreases in the second month to 25% and in the third month to 15%. Symptoms of this form of embryopathy
include cardiac defects, cataracts and deafness. In addition microcephalia, mental deficiency, chorioretinitis,
glaucoma, microphtalmia and dental abnormalities are also diagnosed.
In the 2nd and 3rd trimesters the risk for the appearance of fetal abnormalities are smaller (roughly 10%).
Cytomegalovirus:
An infection with the cytomegalovirus (HHV-5, human herpes virus) is the most frequently occurring one during the
fetal period and affects roughly 3% of pregnant women.
One assumes that during the embryonic period this infection is lethal and leads to a spontaneous miscarriage
in the first trimester. Children that are infected in the early part of the fetal period are asymptomatic and are
detected thanks to special diagnostic techniques.
From the 2nd trimester an infection with the virus leads to the following disease pictures: retarded growth, changes
in the CNS (microcephalia, cerebral atrophy, hydrocephalia, cerebellary hypoplasia, chorioretinitis, atrophy of the
eyes) and hepatosplenomegalia.
Herpes simplex:
As a rule, an infection by the herpes simplex virus (HSV) occurs only in the late phase of the pregnancy. A fetal
infection leads to mental deficiency, microcephalia, myocardiopathy, spasticity, retinal dysplasis and characteristic
dermal wounds.
Often the baby gets infected during birth due to a genital herpes infection of the mother.
Around 50% of the children of infected mothers get infected during the birth process and half of them die from it.
Delivery via caesarian section can prevent this.
Varicella virus:
The varicella virus is responsible for congenital abnormalities that appear in the course of the first four months. To
these belong scarring, muscle atrophy, hypoplasia of the limbs and fingers, abnormalities of the eyes and the brain
(mental deficiency). The teratogenic risk has been established only up to the 20th week.
HIV (Human Immunodeficiency Virus):
The HIV is responsible for the acquired immunodeficiency syndrome (AIDS). In the past few years, HIV infection of
pregnant women has grown into a huge problem (worldwide 33.4 million people now carry the virus).
When the mother is seropositive, a third of the children that she gives birth to become infected.
The infection of the child occurs in utero in 1/3 of the cases. In 2/3 of the cases the infection occurs during
the delivery and one supposes that it occurs via the feto-maternal blood exchange shortly or during the delivery
or via contact with cervico-vaginal secretions and maternal blood during the passage through her genital
apparatus. A caesarian section and an antiviral treatment are recognized measures for reducing the risk of
infection. The congenital anomalies that occur due to an in utero infection can be retarded growth, microcephalia
84
and mental deficiency.
Non-viral pathogens
•
•
Toxoplasmosis:
The toxoplasmosis pathogen is an intracellular parasite (toxoplasma gondii), which gets
through the placenta and infects the embryo. Pregnant women should avoid household pets and
should consume no raw meat or non-pasteurized milk.
In the case of a first infection, the danger of infection at the beginning of the pregnancy is limited
but is elevated towards the end.
The earlier the infection occurs, the worse it is. The parasite lives in the blood, in the tissues, in
the epithelial cells and in the leucocytes. The consequences of an infection are extremely grave in
the course of the embryonic period: cerebral abnormalities (calcification) and ophthalmic
abnormalities (chorioretinitis), microcephalia, microphtalmia and hydrocephalus. If the infection
occurs at this point it is often lethal.
Congenital syphilis:
In Europe congenital syphilis is seldom encountered. In America, on the other hand, the disease
is becoming an increasingly larger problem (frequency of 0.1% as estimated by the US Preventive
Services Task Force organization, 1989).
The pathogenic agent is Treponema pallidum, which is transmitted via sexual intercourse. An
infected mother transfers the disease to her child. The treponema pallidum is always able to get
through the placenta barrier. Nevertheless, it seems the fetus is only threatened by an infection
after the 4th month. It is the first infection of the mother during pregnancy that causes a
congenital syphilis in the baby. This becomes worse the longer the infection lasts. A treatment
with antibiotics (penicillin) kills the microorganism. The early symptoms of an untreated congenital
syphilis are mental deficiency, hydrocephalus, deafness, blindness, bone malformations and
pathognomic abnormalities of the teeth (Hutchinson's teeth).
To the late symptoms number the Hutchinson triad: keratitis, deafness, "screwdriver teeth".
85
Physical agents
•
Ionizing radiation:
Ionizing radiation causes breaks in DNA strands and thus disturbs
replication. The effects it has on the embryo depends on the absorbed
dose (lethal dose: 150 cgy - centi Gray - in gonad dose), and on the
developmental stage of the embryo or fetus.
In Hiroshima and Nagasaki after the nuclear irradiation one determined that
especially injuries in the area of the nervous system and the eyes occurred
that resulted in psychomotoric retardation, microcephalia, spina bifida
cystica and ophthalmic abnormalities (cataracts).
Cerebral malformations were never diagnosed when an irradiation was
below 50 cGy. According to this data, during a pregnancy, the dose of
radiation, directed at the gonads, should never exceed 10 cGy.
During a radiodiagnostic examination 2 cGy are emitted. A single x-ray
should not, therefore, be grounds for an abortion.
Nevertheless, in pregnant women, for safety reasons, every radiodiagnostic
examination should avoid the pelvic region when possible.
86
Further factors
• Maternal diabetes:
Maternal diabetes leads to a disorder of embryonic and fetal
development.
Especially in the embryonic period a badly controlled diabetes with
continuous hyperglycemia and an associated ketosis can
increase the risk for congenital abnormalities by two or three times.
Besides a macrosomia (size) and the holoprosencephalia (error
in the separation of the brain into two hemispheres), one also
observes an increase in heart diseases and the "caudal atrophy
syndrome"
• Phenylketonuria (PKU):
Maternal phenylketonuria is a potential, metabolic teratogenic
factor that increases the risk of abnormalities of the CNS and heart.
These abnormalities can be prevented when the mother holds to a
phenylalanin poor diet.
87
Summary
• Spontaneously, around 2 to 3% of the children are born with a
visible abnormality.
At the time of delivery many anomalies are not yet
recognizable. One assumes that up to 10% of the newborns have
congenital anomalies.
•
•
•
•
•
The distribution of these abnormalities and their causes is as
follows:
Multifactorial, inherited origins: 10 - 20%
Chromosomal origins: 3 - 5%
Connected with irradiation: >1%
Connected with medications or chemical substances: 4-5%
Unknown origin: 65 - 70%
88
Fetal phase
89
Fetal phase
In obstetrics the pregnancy weeks (PW) are normally reckoned from the date
of the Last Menstrual Period (LMP). This is a point in time that many women
can easily remember. Computed this way, the pregnancy lasts 40 weeks and
the embryonic period - accordingly - 10 weeks. Caution is advisable, though,
when wishing to calculate the moment of ovulation - and thus fertilization,
closely connected with it - because the moment of ovulation can vary and
depends on many factors (conditioned by the environment and psychological
aspects). In embryology the temporal indices (i.e., the PW), therefore, always
refer to the moment of fertilization even though in practical midwifery the time
following the LMP is still used for computations.
90
Fetal phase
•
After the 8th week, the fetus takes on typical human features, even though at the end of the first
trimenon, the head is still relatively large in appearance. The eyes shift to the front and the ears
and nasal saddle are formed.
The eyelids are also clearly recognizable now. On the body, fine lanugo hairs are formed, which
at the time of birth are replaced by terminal hairs. The physiologic umbilical hernia that arises in
the embryonic period 15-20 has mostly disappeared. In the second trimenon the mother feels the
first movements of the child. In the last trimenon the subcutaneous fatty tissue is formed and
stretches the still wrinkled skin of the fetus. The skin becomes covered more and more with
vernix caseosa. This is a whitish, greasy substance und consists of flaked off epithelial cells
and sebaceous gland secretions. In neonatology this vernix caseosa is an important criterion for
judging the maturity of the child. If the birth occurs post-term, it disappears again.
Stage 23
Approx. 56th
day
1 Umbilcal cord with hernia
2 Nose
3 Eye
4 Eyelid
5 Ear (a: tragus, b: antitragus )
6 Mouth
7 Elbow
8 Finger
9 Toes
10 Atrophied embryonic tail bud
27 31
mm
Telencephalon
Diencephalon
Mesencephalon
Metencephalon
Myelencephalon
Spinal cord
91
Fetal phase
Development of the form and position of the fetus
•
In the fetal period large changes of the form no longer take place. It is a period of
growth. With the increase in size, especially of the inner organs, and with the overall
growth of the fetus it stretches itself out again and takes on its typical shape.
Normally, it positions itself so it is aligned with the longitudinal axis of the mother and,
96 % of the time, with its head downwards (head presentation). Probably, the pearshaped form of the uterus is responsible for this, in that the head fits better into the
narrower lower part than the lower extremities do.
92
Fetal phase
Weight development
•
The following hormones are responsible for the intrauterine growth of
the child:
- Growth hormone (somatotropin), produced in the adenohypophysis, and
insulin-like factors from the liver stimulate the growth and metabolism of
cartilage, bones and muscles.·
- Glucocorticoid (e.g. ACTH), produced in the adrenal cortex, accelerates fetal
maturation.
- Thyroid hormones (T3 and T4) released by the thyroid gland have an influence
on fetal growth.
- Insulin is an endocrine regulator of prenatal growth.
- Local growth factors influence tissue growth and development.
- Placental hormones have a large influence on the child's growth. The placenta 93
produces factors that are partly protective and partly stimulating.
Acknowledgments
Physicians
Dr. med. R. Moffat
Dr. med. G. Sartorius
Dr. med. A . Raggi
Dr. Astrid Ahler
Clinical Researcher
Dr. Maria De Geyter
Dr. Sofia Forte
Researchlab
Dr. Hong Zhang
Dr. Anne-Catherine Feutz
Schneider Brigitte
PhD Student
Nadira M'Rabet
Xiaoli Shen
Flurina Pletscher
Wang Xinggan
Prof. Dr. med. Christian De Geyter
Technicians
Helga Grässlin
Kornelia Weber
Nicole Crisante
Nadja Kuratli
Mylène Eby
Nurses
Sandra Brodbeck
Jacqueline Amstutz
Simone Gänser
Britta Bernauer
Caroline Bamert
Lorenza Tinelli
Evelyne Dold
Administration
Florije Gashi
Secretary
Hanna Flükiger
94
Swiss Center of Applied Human Toxicology