Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
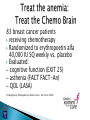
Ana Maria Lopez, MD, MPH, FACP Associate Professor of Clinical Medicine and Pathology Define “chemo brain”/cognitive dysfunction Identify chemotherapy’s effects on cognitive function Understand potential causes Outline patient concerns and usual care Discuss self management strategies for “chemo brain” Identify symptoms that would necessitate medical attention Number of patients receiving dose-intense chemotherapy for breast cancer has increased Number of breast cancer survivors has increased Number of survivors who are experiencing long term side effects has increased Cognitive dysfunction is one of these late effects Children with cancer: at risk for academic underachievement due to: side effects of treatment, school absences, and anxiety related to their disease. “chemo brain” Impairment of cognitive function related to cancer and/or cancer treatment May present as dementia or delirium Characterized by slower memory retrieval, reduced information retention, and difficulty concentrating Reasoning, problem solving, and talents are not affected “I have chemo brain. I can’t concentrate.” “I used to teach and lecture. Now, I have trouble putting sentences together.” “I’ve lost my focus. I can’t even keep track of the characters in a movie!” Cancer and cancer treatment can raise the risk for both Greater risk of experiencing dementia and delirium with increased age Delirium most often caused by specific ailment Dementia often caused by more general conditions Dementia: Definition: Loss of mental function that affects daily living Onset: Gradual over months and years Causes: Brain tumor, stroke, Alzheimer’s, Huntington’s disease, vascular dementia Symptoms: Difficulty completing familiar tasks, disorientation, language problems, memory loss, disruptive/inappropriate behavior, fragmented sleep Delirium: Definition: Acute confused state Onset: Sudden (within hours/days) with fluctuating symptoms Causes: Medication (such as chemotherapy), infections, fever, anemia, malnutrition, dehydration Symptoms: Reduced ability to focus, sustain or shift attention, reduced awareness, impaired memory, agitation, apathy, affected sleep Symptoms associated with dementia and delirium Reduction in information recalled and absorbed at once Things take longer to do, require more mental effort Similar to Attention Deficit Disorder (ADD) Noticeable difference in carrying out tasks when compared to pre-cancer cognitive state Here are a few examples of what patients experience with chemo brain: Forgetting things: short-term loss Difficulty concentrating, focusing attention Trouble remembering details like names, dates Trouble multi-tasking: cognitive flexibility Taking longer to finish things: information processing speed Trouble finding the right words to say Feeling in a “chemo fog” Yes, chemo brain is real, but there is not a single cause Postulated mechanisms of chemotherapy-associated cognitive changes Vardy, J. et al. Ann Oncol 2007 0:mdm500v1-500; doi:10.1093/annonc/mdm500 Copyright restrictions may apply. Many physicians attribute pt’s cognitive concerns to: ◦ Menopause ◦ Depression ◦ Anxiety The cancer itself Chemotherapy drugs Other drugs used as part of treatment Patient age (greater chance over age 60) Stress Low blood counts/anemia Stress/depression – can impede concentration Medication to aid side effects/pain meds - can cause severe drowsiness Hormonal changes – can cause cognitive changes Low blood counts – can cause fatigue, which may make it difficult to concentrate 20-30% of people undergoing chemotherapy for any type of cancer will experience cognitive impairment Often breast cancer patients are more likely to have symptoms of chemo brain One study found 35% of women with breast cancer had memory problems before starting chemotherapy* * www.chemobraininfo.org Tx Arm N Cognitive impairment (%) Odds ration P-value CMF 39 28% -- -- Control 34 12% 6.4 .013 Not affected by anxiety, depression, fatigue or time since treatment. Cancer 1999 47 cancer patients with metastatic cancer and significant prior chemotherapy, at least 3 weeks post treatment 34% had cognitive deficits. 53% had memory deficits 47% had frontal dysfunction 33% had attention difficulties Therefore, neurobehavioral abnormalities should be considered when determining the risks and benefits of cancer treatment. 39 patients and a control group 1.9 years post treatment. Impaired cognitive function: ◦ 28% patients and 12% control Cognitive impairment: ◦ Attention ◦ Mental flexibility ◦ Speed of information processing ◦ Visual memory ◦ Motor function High risk breast cancer patients randomized to high dose or standard dose chemotherapy compared to control Cognitive impairment: ◦ 32% high-dose ◦ 17% standard-dose ◦ 9% control Controlled for anxiety, depression, fatigue 2 years post treatment Certain complementary therapies can help counter the cognitive side effects of treatments. Women who exercise experience less of the cognitive dysfunction associated with Tamoxifen. It is thought that the release of endorphins help attenuate the neurotoxic effects of some chemotherapies. 83 breast cancer patients receiving chemotherapy Randomized to erythropoetin alfa 40,000 IU SQ weekly vs. placebo Evaluated: – cognitive function (EXIT 25) – asthenia (FACT FACT-An) – QOL (LASA) O’Shaughnessy O’Shaughnessy; Breast Cancer ; Res Treat, (2002) Patients undergoing CT and weekly epo ◦ maintained or improved Hb levels ◦ lessened cognitive decline ◦ lessened decline in QOL, energy, and activity Hb declines may correlate with cognitive dysfunction during CT Functional magnetic resonance images of 60-year-old identical twins during a working memory task with incrementally increasing levels of difficulty (left to right) Ferguson, R. J. et al. J Clin Oncol; 25:3866-3870 2007 Copyright © American Society of Clinical Oncology Fluid attenuated inversion recovery magnetic resonance images of white matter hyperintensities Ferguson, R. J. et al. J Clin Oncol; 25:3866-3870 2007 Copyright © American Society of Clinical Oncology How long does chemo brain last? ◦ Varies from person to person ◦ Once chemo treatment ends most gain back cognitive function within a year ◦ Approximately 20% of people affected by chemo brain say that they regain function to a certain extent and then plateau without full cognitive recovery What if I never return to my precancer cognitive function? ◦ Things can be altered in daily life to aid in helping manage chemo brain ◦ For example, take notes and write things down to help with remembering things ◦ Enlist the help of others to remind you of things and help you remember things ◦ People can retain their functionality, but it will take effort Use a detailed daily planner Exercise the brain: take a class, do word puzzles, or learn a new language Track and document difficulties Set up and follow routines Write reminder notes Get enough rest and sleep Get physical activity and eat a healthy diet Are there tests that measure brain changes? ◦ There have not been many pre-treatment, post-treatment studies ◦ There is no standard measure Is chemo brain a brain injury? ◦ Chemo brain may be considered a type of brain injury ◦ Carefully document all symptoms experienced and talk with your doctor about what you’re experiencing ◦ Doctors might recommend diagnostic testing to see what is causing symptoms and rule out other possibilities Series of memory aids In severe cases, neuropsychologists are recommended to assess to treat symptoms ◦ Neuropsychologists may recommend cognitive rehabilitation In general, cancer patients have fairly mild focused cognitive problems that respond well (Myers, 2000) Facilitates recovery of cognitive function and maximizes accommodation to current function If cognitive function gets severely, noticeably worse in a short time period If depression worsens or thoughts of suicide occur seek medical attention If headache will not go away or head pain feels sharp it might be a sign of another condition “Can chemotherapy affect my memory?” Nearly two-thirds of women treated with chemotherapy develop some level of cognitive problems Most recover on their own in the weeks or months after treatment stops As many as 20% to 25% of patients may develop lasting problems Cognitive neurorehabilitation techniques may help American Cancer Society www.cancer.org, search “chemo brain” (http://www.cancer.org/docroot/MBC/content/MBC_ 2_3x_Chemobrain.asp) Breast Cancer.org www.breastcancer.org, search “chemo brain” (http://www.breastcancer.org/treatment/planning/a sk_expert/2008_10/) National Cancer Institute www.cancer.gov, search “cognitive dysfunction” Chemo Brain Info www.chemobraininfo.org Mayo Clinic www.mayoclinic.com, search “chemo brain”