Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
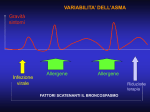
le urgenze pneumologiche in pronto soccorso Pavia, 24 novembre 2006 LA CRISI ASMATICA Angelo Corsico Clinica di Malattie dell’Apparato Respiratorio Fondazione IRCCS Policlinico S.Matteo Università di Pavia le urgenze pneumologiche in pronto soccorso Pavia, 24 novembre 2006 Premessa Gestione delle crisi asmatiche La gestione in Pronto Soccorso Altri trattamenti Six-part Asthma Management Program Part 5: Managing Severe Asthma Exacerbations Severe exacerbations are life-threatening medical emergencies Care must be expeditious and treatment is often most safely undertaken in a hospital or hospital-based emergency department Adult and child asthma emergency department rates, United States: 1992–2001 140 Children Rate per 10,000 120 100 80 Adults 60 40 20 0 92 Source: National 94 96 98 2000 Hospital Ambulatory Care Survey; National Center for Health Statistics During exacerbations: a linear decline of PEF over a period of a few days, a sharp point of inflection, then a linear increase. During poor asthma control: wide diurnal variability and bronchodilator reversibility. Reddel, Lancet 1999 EMERGENCY VISITS FOR ASTHMA Policlinico San Matteo, Pavia 2002 % OF SUBJECTS WITH ED ADMISSIONS BY CAUSES OF ASTHMA ATTACK Severe asthma 7% Poor asthma control (inadequate treatment) Clinical respiratory infections 64% 15% Acute exposure to allergens or other triggers 14% Cerveri et al. ATS 2004 CONSENSUS DEFINITION OF ACUTE SEVERE ASTHMA Rapid exacerbation characterized by one or more of the following features: Accessory muscle activity Paradoxical pulse exceeding 25 mmHg Heart rate > 100 beats/min Respiratory rate > 25-30 breaths/min Limited ability to speak PEF rate or FEV1 < 50% pred. Arterial oxygen saturation < 91-92% McFadden, AJRCCM 2003 Deaths Due to Asthma, United States, 1979-2001 age group 0 to 4 5 to 14 15 to 34 35 to 64 65 + 6000 5000 4000 3000 2000 1000 0 Year Source: Compressed Mortality Files Our study indicates that 1,499 deaths (33% of all 4,487 deaths from asthma in the United States in 2000) occurred in patients hospitalized for asthma exacerbations. Improvements in the management of asthma exacerbations before hospitalization (e.g., at home, during transportation to the emergency department) will have the greatest benefit in further reducing the overall risk of death. Krishnan, AJRCCM 2006 263 potential asthma-related athletic deaths between July 1993 and December 2000. The subjects were usually white male aged 10 to 20 years. Mild intermittent or persistent asthma by history was commonly identified. Sudden fatal asthma exacerbations occur in both competitive and recreational athletes and can be precipitated by sporting activity. The positive benefits to an active lifestyle cannot be negated by the risks outlined here. Becker, JACI 2004 le urgenze pneumologiche in pronto soccorso Pavia, 24 novembre 2006 Premessa Gestione delle crisi asmatiche La gestione in Pronto Soccorso Altri trattamenti Key Points Early treatment is best. Important elements: – A written action plan Guides patient self-management at home Especially important for patients with moderate-to-severe persistent asthma and any patient with a history of severe exacerbations – – Recognition of early signs of worsening asthma Prompt communication between patient and clinician about: Serious deterioration in symptoms or peak flow, or Decreased responsiveness to inhaled beta2-agonists, or Decreased duration of beta2-agonist effect Risk Factors for Death From Asthma Past history of sudden severe exacerbations Prior intubation or admission to ICU for asthma ≥2 hospitalizations for asthma in the past year ≥3 ED visits for asthma in the past year Hospitalization or an ED visit for asthma in the past month Use of >2 canisters per month of inhaled shortacting beta2-agonist Risk Factors for Death From Asthma (continued) Current use of systemic corticosteroids or recent withdrawal from systemic corticosteroids Difficulty perceiving airflow obstruction or its severity Comorbidity, as from cardiovascular diseases or chronic obstructive pulmonary disease Serious psychiatric disease or psychosocial problems Risk Factors for Death From Asthma (continued) Low socioeconomic status and urban residence Illicit drug use Sensitivity to Alternaria Six-part Asthma Management Program Part 5: Establish Plans for Managing Exacerbations Primary therapies for exacerbations: Repetitive administration of rapid-acting inhaled β2-agonist Early introduction of systemic glucocorticosteroids Oxygen supplementation Closely monitor response to treatment with serial measures of lung function Six-part Asthma Management Program Part 5: Establish Plans for Managing Exacerbations Treatment of exacerbations depends on: The patient Experience of the health care professional Therapies that are the most effective for the particular patient Availability of medications Emergency facilities le urgenze pneumologiche in pronto soccorso Pavia, 24 novembre 2006 Premessa Gestione delle crisi asmatiche La gestione in Pronto Soccorso Altri trattamenti Brief Physical Exam Assess severity: Alertness, distress, accessory muscle use, tachycardia, tachypnea, pulsus paradoxus, cyanosis Identify complications (e.g., pneumonia, pneumothorax, pneumomediastinum) Identify diseases that affect asthma (otitis, rhinitis, sinusitis) Rule out upper-airway obstruction Functional Assessment Measure FEV1 or PEF: Upon presentation (begin treatment as soon as asthma exacerbation is recognized) At intervals depending on response to therapy Before discharge Monitor SaO2 in patients with severe distress or with FEV1 or PEF <50% predicted Brief History (after treatment is initiated) Time of onset and cause of exacerbation Severity of symptoms, especially compared to previous attacks All current medications and time of last dose Prior hospitalizations and ED visits, especially in past year Prior episodes of respiratory failure or loss of consciousness due to asthma Existence of comorbidities Laboratory Assessment Consider ABG in patients with suspected hypoventilation, severe distress, or with FEV1 or PEF <30% predicted after initial treatment CBC may be appropriate in patients with fever or purulent sputum Serum theophylline concentration Serum electrolytes, chest x-ray, ECG in special circumstances Emergency Department and Hospital Management: Goals Correction Rapid of significant hypoxemia reversal of airflow obstruction Reduction of likelihood of recurrence Initial Treatment Oxygen to achieve O2 saturation >90% FEV1 or PEF >50%: Inhaled beta2-agonist by metered-dose inhaler or nebulizer, up to three treatments in first hour FEV1 or PEF <50%: Inhaled high-dose beta2-agonist and anticholinergic by nebulization every 20 minutes or continuously for 1 hour Oral corticosteroids Repeat assessment (symptoms, physical exam, PEF, O2 saturation, other tests as needed) Initial Treatment (continued) Impending or Actual Respiratory Arrest Intubation and mechanical ventilation with 100% O2 Nebulized beta2-agonist and anticholinergic Intravenous corticosteroid Admit to hospital intensive care Treatment After Repeat Assessment • Physical exam: moderate symptoms • FEV1 or PEF > 50% predicted or personal best • Inhaled short-acting beta2agonist every 60 minutes • Systemic corticosteroid • Continue treatment 1 to 3 hours, provided there is improvement • Physical exam: severe symptoms at rest, accessory muscle use, chest retraction • History: high-risk patient • FEV1 or PEF <50% predicted or personal best • No improvement after initial treatment • Oxygen • Inhaled short-acting beta2agonist hourly or continuously + inhaled anticholinergic • Systemic corticosteroid Emergency Department and Hospital Management Not generally recommended: Methylxanthines Antibiotics (except for patients with pneumonia, bacterial sinusitis) “Aggressive” hydration Chest physical therapy Not recommended: Mucolytics Sedation Good Response • No distress • Physical exam: normal • FEV1 or PEF >70% • Sustained response @ 60 min after last treatment • Discharge Home Incomplete Response • Mild-tomoderate symptoms • FEV1 or PEF 50% to 70% Poor Response • Physical exam: symptoms severe, drowsiness, confusion • PCO2 >42 mm Hg • FEV1 or PEF <50% • Individualized decision: hospitalization • Admit to hospital or intensive care Hospitalization Consider: Duration and severity of airflow obstruction Course and severity of prior attacks Medication use Access to care Home conditions and support Comorbidities Admit to Hospital Intensive Care • Inhaled beta2-agonist hourly or continuously + inhaled anticholinergic • IV corticosteroid • Oxygen • Possible intubation and mechanical ventilation • Admit to hospital ward Emergency Department Discharge Criteria If FEV1 or PEF 70% predicted and symptoms are minimal, discharge If FEV1 or PEF >50% but <70% predicted and symptoms are mild, decision is individualized If response is prompt, observe for 30 to 60 minutes before discharging Emergency Department and Hospital Discharge Actions Prescribe sufficient medication and instructions for use Schedule follow-up or referral visit within 3 to 5 days – Consider referral to specialist if patient has history of life-threatening exacerbations or multiple hospitalizations Teach correct inhaler use and trigger avoidance Hospital Discharge Actions (continued) Discharge medications should include: – Short-acting beta2-agonist – Sufficient oral corticosteroid to complete course of therapy (3 to 10 days) or to continue therapy until followup appointment – If inhaled corticosteroids are prescribed, start before course of oral corticosteroids is completed le urgenze pneumologiche in pronto soccorso Pavia, 24 novembre 2006 Premessa Gestione delle crisi asmatiche La gestione in Pronto Soccorso Altri trattamenti Intravenous magnesium (MgSO4) Is effective at improving airflow and reducing admissions in very severe asthma exacerbations (eg, 40% of predicted PEF). Has few adverse effects, is inexpensive, and is easy to administer. Rapid adoption of this therapy in North American EDs. Intravenous leukotriene modifiers Data on intravenous montelukast suggest that leukotriene modifiers have important bronchodilating effects and that this adjunct therapy may prove useful. The relatively slow onset of action of oral agents will limit their usefulness in the management of truly severe exacerbations. Intravenous epinephrine In some Australian EDs is commonly used to treat the acute bronchospasm, initiate adequate antiinflammatory treatment, and avoid the risks and complications associated with intubation. Theoretically it may control airway edema but its use needs to reflect a balance between clinical efficacy and safety. Evidence on therapeutic safety is difficult to collect and research. Epinephrine should not be the first step in treating these patients. PEF ~ 70% PEF ~ 50% EMERGENCY VISITS FOR ASTHMA Policlinico San Matteo, Pavia 2002 Without previous admission With frequent admission 40% 60% With one previous admission Cerveri et al. ATS 2004