Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
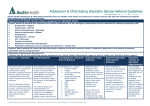
Leeds Dental Institute – Periodontology Referral Form Please refer to the guidelines overleaf before completing this form – COMPLETE ALL SECTIONS PRACTICE DETAILS Referrer Name: Date of Referral: Practice Address: Tel: Fax: Postcode: Email: Type of referral: Routine Urgent PATIENT DETAILS Name: DOB: Sex: Male Female Contact Address: Tel (Home/Work/Mobile): Postcode: NHS no/ Hospital no: Medical History: Smoking status: BPE scores: Please select referral category: Chronic periodontal disease (BPE scores 4) where appropriate primary care treatment has been unsuccessful Aggressive disease, judged by severity of periodontal destruction relative to age or rate of periodontal breakdown Need for surgical management (e.g. mucogingival procedures for recession, open flap debridement, regenerative procedures, crown lengthening) Increased risk of periodontal disease due to a medical condition (e.g. poorly controlled diabetes, drug induced gingival overgrowth) Risk of complications from periodontal treatment (e.g. bleeding disorders, immunocompromised) Requirement for complex restorative planning Other (provide details)………………………………………………………………………………. Reason for referral: PLEASE CONFIRM THAT THE FOLLOWING TREATMENT HAS BEEN PROVIDED IN PRIMARY CARE (see referral protocols for guidance, patients who have not had this treatment will not be accepted for treatment in the hospital) Smoking Cessation Advice (if applicable) Oral Health Education Full Mouth Scaling and Subgingival Debridement THIS REFERRAL INCLUDES Relevant Radiographs Periodontal Charts: with Local Anaesthetic Pre-treatment Post treatment If this information is not included please detail why: Signed: Document1 Date: