Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
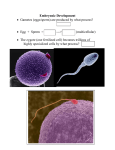
Chapter 4 Third Week of Human Development 解剖學科 鄭授德 本教材圖片取自於 The Developing Human (9th ed) Moore, Persaud and Torchia • • • The 3rd week (the 5th week after the day one of LNMP) is the beginning of embryonic period. The 8th week is the end. Important events 1. Formation of the primitive streak 2. Notochord 3. Three germ layers • Cessation of menstruation (~ 5 weeks after LNMP) is the first indication of pregnancy. 3.5 wk, umbilical vesicle Gastulation: Formation of Germ Layers • Gastrulation: embryonic disc from bilaminar develops into trilaminar; the embryo is gastrula. • Each layer of trilaminar develops into specific tissues and organs – Embryonic ectoderm: epidermis, nervous system, and others – Embryonic mesoderm: smooth muscular coats, connective tissue, and vessels; also blood cells and born marrow, skeleton, striated muscles, reproductive and excretory organs. – Embryonic endoderm: epithelial linings of respiratory and GI tracts and glandular cells Primitive Streak • At the beginning of the 3rd week, thickened linear band of epiblast on the dorsal caudal aspect of embryonic disc. • Primitive node (and pit) is on its cranial end. • Primitive groove on the primitive streak (Fig. 4-2) Primitive Streak • Mesenchyme from inward turning of epiblast cells through primitive groove forms (intra)embryonic mesoderm, and displacing hypoblast forms (intra)embryonic endoderm. • Epiblast now can be called (intra)embryonic ectoderm. Fate of Primitive Streak • • • The process of forming mesoderm through primitive streak slows down after the early 4th week degenerates by the end of 4th week in the sacrococcygeal region of embryo. Sacrococcygeal teratoma developed from the remnants of primitive streak Notochordal Process and Notochord • • Notochordal process - mesenchymal cells migrate cranially from primitive node and form a cellular cord until it reaches the prechordal plate (mouth region in future). Prechordal plate serves as a signaling center for controlling development of cranial structures. Notochordal Process and Notochord • • The lumen within it is called notochordal canal. Mesenchymal cells extend laterally and cranially to the margin of embryonic disc and continuous with extraembryonic mesoderm. Notochordal Process and Notochord • Some mesenchymal cells migrate cranially alone the sides of notochord process and meet at cardiogenic area. Fate of the Notochord • • • It is the structure around vertebral column in the future, and degenerates as nucleus pulposus in the intervertebral disc. Notochord induces the development of neural plate (future central nervous system). A small passage, neuroenteric canal connects amniotic cavity with yolk sac, but will be sealed after notochord completes. • Cloacal membrane--caudal to primitive steak, the future sites of anus. • Oropharyngeal membrane--remains bilaminar, ectoderm and endoderm fuse there. • Mesoderm separates ectoderm and endoderm, except at cloacal membrane, oropharyngeal membrane and notochord. Formation of the Notochord • The notochord defines the primitive axis of the embryo and indicate the future site of vertebral column. Allantois • • • It appears on day 16 as a sausagelike outpouch from caudal end of yolk sac into connecting stalk. It is involved with early blood formation and associated with urinary bladder development. It becomes urachus and remains as median umbilical ligament. Neurulation: Formation of Neural Tube • The formation of neural plate and neural folds and the closure of these folds to form the neural tube. • It is completed by the end of the 4th week. The embryo is called neurula during neurulation. Neural Plate and Neural Tube • Neuroectoderm— – neural plate induced by notochord and develops into CNS (brain and spinal cord) • Neural plate broadens and extends as far as oropharyngeal membrane and beyond notochord. • • Invagination of neural plate forms neural groove with neural folds on both sides. Cranial enlargement of neural fold is the first sign of brain development. • • • End of the 3rd week, neural folds fuse and neural plate into neural tube. Both ends of neural tube are rostral and caudal neuropores. Both close during 4th week when neurulation completes. Neural Crest Formation • • • • The crest of each neural fold detaches when neural tube forms. These flattened mass is called neural crest, which will forms sensory ganglia of spinal (dorsal root ganglia) and cranial nerves (V, VII, IX, X). Also, it forms the Schwann cells, pia mater, arachnoid, pigment cells, adrenal medulla, and several skeletal and muscular components in the head. Congenital defects: – meroanencephaly (anencephaly) (p.400). – spina bifida cystica (p.401). Development of Somites • • Both lateral sides of notochord mesoderm forms a paraxial mesoderm. Lateral to it are the intermediate and lateral mesoderms. Somites - by the end of the 3rd week, paraxial mesoderm develops into 38 pairs of cuboidal bodies (days 20 to 30). End of 5th week, 42 to 44 pairs. 18-day 20-day 21-day • • Somites are so prominent as to be a criteria for determining the age of embryo in 4th and 5th weeks. Somites appears first at occipital region at the end of the 3rd week and give rise to axial skeleton (bone of head, neck and trunk), associated musculature and dermis of skin. 18-day 20-day 21-day Development of the Intraembryonic Coelom • Intraembryonic coelom (cavity)--fusion of isolated coelomic spaces in the lateral mesoderm and cardiogenic mesoderm into a horseshoe-shaped cavity. • During the 2nd month, intraembryonic coelom is divided into 3 body cavities: 1. 2. 3. Pericardial cavity Pleural cavities Peritoneal cavity Lateral mesoderm divided into: • Parietal layer— – together with extraembryonic mesoderm covering amnion and ectoderm called somatopleure, embryonic body wall (upper side) • Visceral layer— – together with extraembryonic mesoderm covering yolk sac and endoderm is called splanchnopleure, embryonic gut wall (lower side) Early Development of Cardiovascular System • • • • Blood vessel formation (angiogenesis) occurs at the beginning of the third week in the extraembryonic mesoderm covering yolk sac, connecting stalk, and chorion. Without significant amount of yolk, the embryo needs blood vessels to supply nutrition and oxygen. At the end of the 2nd week the embryo obtains nutrition from maternal blood through diffusion; During the 3rd week it develops a primitive placental circulation. Vasculogenesis and Angiogenesis Developing of blood vessels and blood in the embryo and extraembryonic membranes during the third week 1. Blood island – angioblasts (a kind of mesenchymal cell) aggregate in isolated cluster with cavities 2. Primitive endothelium – angioblasts flatten to form endothelial cells around cavity 3. Network – cavities fuse together 4. Vessels extend to fuse with vessels in adjacent area Primitive blood cells and plasma • • • develop from endothelial cells of vessels in umbilical vesicle and allantois at the end of the 3rd week. It occurs in embryo (liver first, than spleen, bone marrow and lymph nodes) in the 5th week. Fetus and Adults – erythrocytes are derived from different hematopoietic progenitor cells. Primitive Cardiovascular System • • • heart and great vessels are developed from cardiogenic area. Heart tube is fused from endothelial heart tube by the end of the 3rd week. Heart tube joined by vessels in the embryo, connecting stalk, chorion, and yolk sac form a primitive cardiovascular system. Primitive Cardiovascular System • • Heart beats and blood circulation start on 21st or 22nd day (5 weeks after LNMP). Cardiovascular system is the first organ system to reach a functional state. Further Development of Chorionic Villi • • • • Primary chorionic villi--at the end of the 2nd week Secondary chorionic villi--the early 3rd week, with mesenchymal core in the branching villi covering all surface of chorionic sac Tertiary chorionic villi--day 15 to 20 arteriocapillary venous networks develop villi The end of the 3rd week blood flow starts; oxygen, nutrients in the maternal blood exchange with CO2 and waste in embryonic blood by diffusing through the wall of villiplacental membrane. Primary Secondary Tertiary Cytotrophoblastic shell • Cytotrophoblasts extend through syncytiotrophoblastic layer forming a shell to attach the chorionic sac to the endometrium. • Main exchange site— – stem (anchoring) villi and their branch villi Abnormal Growth of the Trophoblast • Hydatidiform moles – Without vasculization in tertiary villi; – Form cystic swellings; produce excessive hCG; – 3~5% of them form choriocarcinomas, which may spread to lungs, vagina, liver, bone, intestine, and brain through bloodstream.. Chapter 5 Fourth to Eighth Weeks of Human Development 解剖學科 鄭授德 本教材圖片取自於 1. The Developing Human (9th ed) Moore, Persaud and Torchia 2. Human Anatomy (6th ed), Marieb, Mallatt, and Wilhelm Phases of Embryonic Development 1. Growth - increase in size. 2. Morphogenesis - development of form 3. Differentiation - maturation of physiological processes • Teratogens - agents (drugs or virus) that produce or increases the incidence of birth defects. • Exposure of embryo to the teratogen within the 4th to 8th weeks may cause major congenital defects. Folding of the Embryo • Foldings in median and horizontal planes change the flat trilaminar embryo disc into a cylindrical embryo. • Folding of the Embryo in the Median Plane – Head and tail move ventrally • Folding of the Embryo in the Horizontal Plane – Lateral folding rolls the sides of embryo disc and turns part of endoderm into embryo as midgut – the rest left outside (yolk stalk) and will be incorporated into umbilical cord. 22-day Beginning of 4-wk 26-day End of 4-wk 28-day The Head Fold • Septum transversum (transverse mesodermal septum), primordial heart, pericardial coelom, and oropharyngeal membrane line from cranial to caudal in the head region of trilaminar embryonic disc. • Septum transversum develops into the central tendon of the diaphragm. • The end of the 3rd week, primitive brain protrudes into amniotic cavity. Later, it grows crainally and hang over oropharyngeal membrane and developing heart. The longitudinal infolding turns endoderm inward as foregut (primordium of pharynx, etc.). 21 days 26 days The Tail Fold • Cloacal membrane on the caudal end of primitive streak develops into future anus. • Neural tube growing over cloacal membrane causes infolding and turns part of endoderm into embryo as hind gut. • Connecting stalk turns to ventral surface, and allantois is incorporated into embryo. Beginning of 4-wk End of 4-wk Germ Layer Derivatives Ectoderm • CNS • PNS • Sensory epithelial of eye, ear, and nose • Epidermis and hairs and nails • Mammary glands • Pituitary gland • Subcutaneous glands • Enamel of teeth Neural crest cells • Cells of spinal, cranial nn. and autonomic ganglia • Ensheathing cells of PNS • Pigment cells of dermis • Muscle, connective tissues, and bone of pharyngeal arch origin • Suprarenal medulla • Meninges of brain and spinal cord. Germ Layer Derivatives Mesoderm • Connective tissue • Cartilage • Bone • Striated and smooth muscles • Heart • Blood and lymph vessels • Kidneys • Ovaries • Testes • Genital ducts • Serous membranes lining pericardial, pleural, and peritoneal cavities • Spleen • Cortex of suprarenal glands Germ Layer Derivatives Endoderm • Epithelial lining of GI and respiratory tracts • Parenchyma of tonsils, thyroid and parathyroid glands • Thymus • Liver • Pancreas • Epithelial lining of urinary bladder and most of urethra • Epithelial lining of tympanic cavity, tympanic antrum, and pharyngotympanic tube Control of Embryonic Development Embryonic development is essentially a process of growth and increasing complexity of structure and function. • Genetic plan in chromosomes • Environmental factors • Development is growth and increasing complexity • Interaction between tissues during development (induction) 1. 2. • • optic vesicle induces the formation of lens uteric bud induces the formation of tubules in the metanephric mesoderm. Molecular mechanism of induction from relating tissue Intracellular signal transduction pathway Fourth Week Early 4th wk Straight embryo Middle 4th wk Neural tube, widely opened neuropores 24 days Mandibular (1st) arch - mandible & maxillary Hyoid (2nd) arch Slightly curves (head and tail folds) Heart prominence 26 days Pharyngeal (branchial) arches Rostral neuropore closes Forebrain elevation C-shaped curvature 26 or 27 days Upper limb buds and otic pits show Lens placodes, attenuated tail are visible End of 4th wk 4th pair arches and lower limb buds show Caudal neuropore closed Fourth Week Early 4th week Middle 4th week Straight embryo Neural tube, widely opened neuropores 22-day 23-day Fourth Week 24 days 24 days Mandibular (1st) arch - mandible & maxilla Hyoid (2nd) arch Slightly curves (head and tail folds) Heart prominence Fourth Week 26 days 26 days Pharyngeal (branchial) arches Rostral neuropore closes Forebrain elevation C-shaped curvature Fourth Week 26 or 27 days End of 4th week 28 days Upper limb buds and otic pits show Lens placodes, attenuated tail are visible 4th pair arches and lower limb buds show Caudal neuropore closed 28 days 28 days Fifth Week Brain rapid grows; face contacts heart prominence Hyoid (2nd) arch overgrows 3rd and 4th arches Forms cervical sinus on lateral sides Upper limb with elbow and hand plate Mesonephric ridges indicate the sites of kidneys Spontaneous movements 33 days Digital rays in hand plates 32 days 32 days Sixth Week • • • • • • Rapid growth of upper limbs Elbow, wrist show; hand plates with digital rays Groove between 1st and 2nd arch develops (external acoustic meatus) Swelling around it (auricular hillocks) Heart prominence against face Respond to touch 42 days Seventh Week • • • Notches between digital rays of hand Only omophaloenteric duct left communicating between primitive gut and umbilical vesicle Prominent umbilical herniation with intestine 48 days Eighth Week • • • • • Final week of embryonic period Webbed digits of hand Notches between digits of foot Tail still present Scalp vascular plexus appears near the vertex (crown) of head. 52 days Eighth Week End of 8th week – All regions of limbs apparent; limbs move – Digit lengthened and separated – Distinct human characteristics – Head takes half of the embryo length – Neck established – Eyelid are obvious – Intestine is still in the umbilical cord – Sexual difference exists but sex still can not be told 56 days 56 days Estimation of Embryonic Age 1. Onset of LNMP (gestational age) 2. The probable time of fertilization 3. Measurements of the chorionic sac and embryo 4. External characteristic of embryo • Spontaneous aborted embryos can be estimated by the appearance of developing limbs. Methods of Measuring Embryos 1. Greatest length (GL) – 2. 3. 3rd and early 4th weeks, straight embryo Crown-rump length (CRL) or sitting height – neck-rump measurement Crown-heel length (CHL) or standing height for 8-wk embryo 4.5-wk CRL 4.8 mm 5-wk CRL 2.09 cm amnion 7-wk CRL 2.14 cm Ultrasound Scanner 6-wk 4th ventricle Chapter 6 Ninth Week to Birth: The Fetal Period 解剖學科 鄭授德 本教材圖片取自於 The Developing Human (9th ed) Moore, Persaud and Torchia • A notable change of the embryo to fetus period relatively slow down in the growth of head compared with the rest of body. • Viability – the ability of fetuses to survive in the extrauterine environment. • Immature infants (extremely low birth weight, ELBW) – less than 500 gm, usually do not survive, but with expert postnatal care some may survive • Low-birth-weight babies – full term but caused by intrauterine growth retardation. • Premature infants (1500 to 2500 gm) most may survive but with difficulties. Estimation of Fetal Age • By ultrasonic measurements to determine the size of infant • To provide the expected date of confinement (EDC) the calculation of age is done by: 1. Gestational age – the onset of the last normal menstrual period (LNMP), used clinically 2. The estimated day of fertilization (used in this book); the month is by calendar month 9-week Trimester of Pregnancy • Trimester – each last for 3 calendar months • The end of the first trimester – all major systems develop – crown-rump length (CRL) is used for measuring • The end of the second trimester – may survive if born prematurely • At 35 weeks – fetus weighed 2500 gm, usually survives if born prematurely Measurements and Characteristics of Fetuses Measuring with ultrasonography and weight in the second and third trimesters: 1. Biparietal diameter (BPD) 2. Head circumference 3. Abdominal circumference 4. Femur length 5. Foot length 6. Fetal weight (may have discrepancy when mother has diabetes mellitus) Nine to Twelve Weeks • Beginning of 9th week – Head = 1/2 CRL – Legs are short, thighs are small • End of 9th week External genitalia show difference • 11th week Intestines return to abdomen • 12th week Fetal form of ext. genitalia established Nine to Twelve Weeks • End of 12th week – Head < 1/2 CRL – Primary ossification center appears – Erythropoiesis site transfer from liver to spleen • Between 9th to 12th week – Urine forms and discharge to amniotic fluid, which is swallowed by fetus 11-week 9-week 12-week Thirteen to Sixteen Weeks 13-week • 14th week – – – – – Rapid growth Coordinated limb movement Active ossification of skeleton Eye movements occur Scalp hair pattern determined • Beginning of 16th week – Bones can be seen on radiographs • 16th week – Ovaries differentiated and contain primordial follicles Seventeen to Twenty Weeks • • • • Fetus grows 50 mm within period Fetal movements (quickening) felt by mother Delivery day is 147 ± 15 days after first movement. Skin is covered and protected by vernix caseosa. 17-week Seventeen to Twenty Weeks 20-week • 20th week – Covered by lanugo (fine downy hair) – Eyebrows and head hairs are visible – Testes begin to descend. • 17th to 20th weeks – Brown fat is the heat production site. • 18th week – Canalization of vagina begins. 18-week Twenty-one to Twenty-five Weeks • Substantial weight gain • Skin wrinkles and is translucent, pink to red • 21st week 25-week fetus – Rapid eye movements begin • 22nd to 23rd weeks – Responds to noise (blink-startle responses) • 24th week – Type II pneumocytes secrete surfactant – Fingernails appear 25-week newborn • 22nd to 25th weeks – Born prematurely may survive under intensive care Twenty-six to Twenty-nine Weeks • Can breathe air by functioning lungs • CNS controls rhythmic breathing and body temperature • 26th week – Eyes reopen – Toenails are visible – Subcutaneous fat flattens wrinkled skin • 28th week – Spleen has been an important site of hematopoiesis – It shifts to bone marrow by the end of 28th week 29-week 26-week 28-week Thirty to Thirty-four Weeks • 30th week – Pupillary light reflex • 32nd week – Born prematurely usually survive – Born as normal weight (premature by date) – White fat = 8% body weight 34-week Thirty-five to Thirty-eight Weeks 36-week • 35th week – Grasp, spontaneous orientation to light • 37th to 38th weeks – Nervous system is mature for integrative functions. • 36th week – Circumference of head is equal to that of abdomen. – CRL 360 mm, weight 3400 gm – Slow growing before birth – White fat = 16% body weight • 38th week – Add 14 gm per day in last week • Full term – Bluish-pink skin; Testes in scrotum 37-week Expected Date of Delivery • 266 days (38 weeks) – Expected time of birth – EDC (expected date of confinement) • 1 to 2 weeks late – 12% of babies • 3 weeks late – 5 to 6% 38-week Factors Influencing Fetal Growth • • • • • Cigarette smoking Multiple pregnancy Alcohol and illicit drugs Impaired uteroplacental and fetoplacental blood flow Genetic factors and growth retardation Procedures for Assessing Fetal Status Perinatology Fetus of 26th week after fertilization to newborn infant of 4 weeks after birth. 1. Ultrasonography – – – Primary imaging modality, a major tool for prenatal diagnosis of fetal abnormalities Measuring placental and fetal size, multiple births, and abnormal placental shape and presentations Wide availability, low cost, and lack of known adverse effects. 3-D Ultrasonogram 28-week 4.5-wk CRL 4.8 mm 5-wk CRL 2.09 cm amnion 7-wk CRL 2.14 cm Ultrasound Scanner 6-wk 4th ventricle Procedures for Assessing Fetal Status 2. Diagnostic amniocentesis – – A common technique for detecting genetic disorder After 14 weeks there is about 200 ml amniotic fluid, and 15-20 ml can be safely withdrawn under real-time ultrasonography. Who may need amniocentesis? • • • • • • > 38 years of maternal age previous birth of a trisomy child chromosome abnormality in either parent a X-linked recessive disorders carrier neural tube defects in the family carriers of inborn errors of metabolism 3. Alpha-fetoprotein (AFP) Assay – – 4. neural tube defects (NTDs; e.g. spina bifida) ventral wall defects (VWDs; e.g. gastroschisis and omphalocele) Spectrophotometric studies – 5. for erythroblastosis fetalis, maternal antibodies destruct fetal blood cells Chorionic villus sampling (CVS) – – – 6. trophoblasts obtained by needle through mother's abdominal and uterine wall under ultrasound guidance Risk of fetal loss: 1% Risk of limb defects if done too early. Sex chromatin patterns – sex-linked hereditary diseases, e.g. hemophilia and muscular XXX XX dystrophy XY XY indicates condensed X chromosome. by cresyl echt violet staining indicates condensed Yq. by quinacrine mustard staining 7. Cell cultures and chromosomal analysis – – 8. for fetal sex and chromosomal aberrations. Also, inborn errors of metabolism Fetal transfusion – for hemolytic disease of the newborn (HDN), blood transfusion through peritoneal cavity or umbilical cord puncture Fetoscopy – few used 9. 10. Percutaneous umbilical cord blood sampling (PUBS) – – sampling blood after 18 weeks for aneuploidy, fetal growth restriction, fetal infection, and fetal anemia. Treating fetal anemia by transfusion packed RBC 11. Computed tomography (CT) and Magnetic resonance imaging (MRI) – – providing more information for treatment MRI has high soft-tissue contrast and resolution 12. Fetal monitoring – for fetal heart rate monitoring (fetal distress-abnormal heart rate) MRI Establishment of openings of the ureters into the bladder at a 21-week fetus