Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
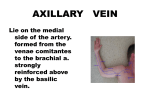
A posterior approach to the elbow joint S. A. Shahane, D. Stanley From the Northern General Hospital, Sheffield, England e describe a posterior approach to the elbow which combines the advantages of both splitting and reflecting the triceps. It gives protection to the ulnar nerve and its blood supply during the operation while providing excellent exposure of the distal humerus. During closure, the triceps muscle can be tensioned, thereby improving stability of the elbow. This approach has particular relevance to unlinked total elbow arthroplasty allowing early rehabilitation of the joint. W J Bone Joint Surg [Br] 1999;81-B:1020-2. Received 2 December 1998; Accepted after revision 23 April 1999 Many surgical approaches to the elbow have been described, of which the posterior is the most common. It provides excellent access for the fixation of fractures of the distal humerus and olecranon, and is the approach used 1-4 In the most commonly for total elbow arthroplasty. 3,5,6 posterior approach the triceps is either split or reflec4,7 1,8 ted or the olecranon is divided. Osteotomy of the olecranon is particularly valuable in the treatment of comminuted distal fractures of the humerus involving the articular surface. It cannot be used, however, for total elbow arthroplasty since this requires an intact ulna for the fixation of the distal component of the prosthesis. Techniques in which the triceps is split or reflected can be used for fixation of fractures and for total elbow arthroplasty, but they give a less satisfactory exposure of the distal humerus than can be achieved by olecranon osteotomy when fractures of the distal humerus are comminuted and involve a significant portion of the articular surface. We describe an approach in which the triceps is both split and reflected. S. A. Shahane, MS Orth, MCh Orth, FRCS G (Orth), Orthopaedic Specialist Registrar D. Stanley, BSc, FRCS, Consultant Orthopaedic Surgeon Orthopaedic Department, Northern General Hospital, Herries Road, Sheffield S5 7AU, UK. Correspondence should be sent to Mr D. Stanley. ©1999 British Editorial Society of Bone and Joint Surgery 0301-620X/99/69696 $2.00 1020 Operative technique The anaesthetised patient is placed in the lateral decubitus position. A sterile tourniquet is applied high on the arm which is supported so that it is horizontal, with the forearm hanging vertically and freely. A posterior incision is made in the skin beginning 8 cm proximal to the olecranon, extending distally, skirting the ulnar aspect of the tip of the olecranon, and continuing for a further 8 cm along the subcutaneous border of the ulna. The ulnar nerve is identified and decompressed superficially. The medial border of the belly of the triceps is identified. An incision is then made proximally in the triceps tendon so that 75% of the muscle lies laterally and 25% medially (Fig. 1). This incision is deepened through the triceps to the tip of the olecranon and continues distally to split the superficial fascia of the forearm for about 6 or 7 cm. The medial triceps, with the superficial fascia of the forearm and the periosteum over the medial aspect of the olecranon, is then reflected medially as a single unit (Fig. 2). Care is taken to maintain the continuity of the extensor envelope where the triceps blends into the fascia of the forearm. The elbow is slightly extended at this stage to relieve the tension at this tenuous junction. The dissection extends subperiosteally, deep to the ulnar nerve and over the tip of the medial epicondyle. The lateral 75% of the triceps is then reflected from the tip of the olecranon. The dissection is extended laterally according to the needs of the procedure being undertaken. The anconeus is then reflected subperiosteally from the proximal ulna to expose the radial head. The posterior capsule is reflected with the triceps, exposing the entire joint (Fig. 3). The dissection is carried out deep to the ulnar nerve which is safely mobilised with its deep soft tissues and blood supply, reducing the risk of postoperative ulnar neuritis. The distal humerus and elbow are exposed entirely, allowing fixation of fractures or total elbow arthroplasty to be carried out safely. At the end of the procedure, reconstruction of the soft tissues is undertaken. Drill holes are placed in the olecranon through which the triceps is reattached to the bone. The medial portion of the triceps is brought back to the olecranon and the ulnar nerve is seen to fall into its anatomical THE JOURNAL OF BONE AND JOINT SURGERY A POSTERIOR APPROACH TO THE ELBOW JOINT 1021 Fig. 1 Diagram of the posterior view of the elbow showing the incision through the triceps and the line of incision to decompress the ulnar nerve. Fig. 2 Diagram showing the medial 25% of the triceps with the superficial fascia of the forearm and the periosteum reflected medially as a single unit, deep to the ulnar nerve. Fig. 3 Diagram showing the retraction of the entire triceps exposing the back of the elbow. position. Reattachment of the triceps to the olecranon allows adjustment of soft-tissue tension. Balancing of the two components of the triceps mechanism can be undertaken so that the risk of postoperative dislocation for unlinked surface replacement arthroplasties is minimised. VOL. 81-B, NO. 6, NOVEMBER 1999 Clinical experience Since 1993, we have undertaken 86 total elbow arthroplasties and reconstructed 20 distal fractures of the humerus using this approach, encountering only one case of post- 1022 S. A. SHAHANE, operative neurapraxia of the ulnar nerve. Spontaneous recovery occurred in this patient after eight weeks. Dehiscence of the triceps was seen on one occasion in a patient who had undergone several previous surgical procedures through posterior approaches after an infected comminuted distal fracture of the humerus. Discussion 5 Campbell described the posterior split of the triceps muscle in the midline, and continued the exposure distally in the forearm by elevating the anconeus and flexor carpi 3 ulnaris. Steiger et al modified this approach by raising 6 osteoperiosteal flaps from the olecranon. Van Gorder created an inverted ‘V’-shaped flap of the triceps mechanism to expose the distal humerus. In all of these approaches there is considerable mobilisation of the ulnar nerve. Petalling of the olecranon, described in the Gschwend approach, can be difficult to achieve safely in patients with rheumatoid arthritis who have marked bony erosion of the ulna. 9 The technique, described by Boyd, involves reflecting the entire triceps mechanism from the lateral to the medial side. 7 Bryan and Morrey used a similar technique but with reflection of the triceps from medial to lateral, beginning at the medial intermuscular septum. The triceps was reflected in continuity with the fascia of the forearm and the periosteum. The advantage of this approach is that the muscle is neither split nor violated and continuity of the extensor mechanism is maintained with the forearm fascio-ulnarperiosteal complex. Ten out of 80 total elbow arthroplasties 2 carried out by Morrey et al had ulnar neuropathies, eight temporary and two permanent. They presumed that the D. STANLEY cause was traction or pressure on the nerve during the operation. Our technique allows the raising of the major part of the triceps in continuity. Protection of the ulnar nerve by the medial part of triceps reduces the possibility of damage to its blood supply and at the end of the operation it can glide and slide in its original position. The availability of the two segments of the triceps muscle for the repair allows satisfactory balancing of the medial and lateral sides of the elbow, reducing the risk of postoperative dislocation. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. References 1. MacAusland WR. Ankylosis of the elbow, with report of four cases treated by arthroplasty. J Am Med Assoc 1915;64:312-8. 2. Morrey BF, Bryan RS, Dobbyns JH, Linscheid RL. Total elbow arthroplasty: a five-year experience at the Mayo clinic. J Bone Joint Surg [Am] 1981;63-A:1050-63. 3. Steiger JU, Gschwend N, Bell S. GSB elbow arthroplasty: a new concept and six years’ experience. In: Kashiwagi D, ed. Elbow joint. Amsterdam: Elsevier Science Publishers BV (Biomedical Division), 1985:285-94. 4. Wolfe SW, Ranawat CS. The osteoanconeus flap: an approach for total elbow arthroplasty. J Bone Joint Surg [Am] 1990;72-A:684-8. 5. Campbell WC. Incision for exposure of the elbow joint. Am J Surg 1932;15:65-7. 6. Van Gorder GW. Surgical approach in supracondylar ‘T’ fractures of the humerus requiring open reduction. J Bone Joint Surg 1940;22: 278-92. 7. Bryan RS, Morrey BF. Extensive posterior exposure of the elbow joint: a triceps sparing approach. Clin Orthop 1982;166:188-92. 8. Muller ME, Allgower M, Willenegger H. Manual of internal fixation: technique recommended by the AO group. New York: SpringerVerlag, 1970. 9. Boyd HB. Surgical exposure of the ulna and proximal third of the radius through one incision. Surg Gynecol Obstet 1940;71:86-8. THE JOURNAL OF BONE AND JOINT SURGERY