Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
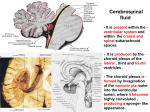
BIOMATERIAL DEVICES And the Epithelium Pulmonary BBB PULMONARY PHYSIOLOGY Functions Ventilation/Conduction Conduction Pathway The relaxation/contraction of circular smooth muscle lining these “airways’” determines how easily airflow can occur (bronchodilation vs. bronchoconstriction). Most gas exchange occurs in the ~8,000,000 alveolar sacs. Functions of Conduction Pathway Alveolar/Capillary Structural Relationship Abundance of pulmonary capillaries Ventilated air is brought into close proximity to the “pulmonary” blood Efficient and thorough gas exchange between the air and the blood. Extensive branching of alveoli: Increased surface area for exchange between air and blood. Alveolar and capillary walls: Thin Permit rapid diffusion of gases Airflow in the lungs: Ventilation. [AIR] EXCHANGE [BLOOD] Gases exchange by diffusion. Bloodflow through the pulmonary capillaries is driven by the contraction of the right ventricle. PULMONARY DRUG DELIVERY Pulmonary drug delivery. Part I: Physiological factors affecting therapeutic effectiveness of aerosolized medications N. R. Labiris & M. B. Dolovich Table 1 Advantages of pulmonary delivery of drugs to treat respiratory and systemic disease. Treatment of Respiratory Diseases Treatment of Systemic Diseases Deliver high drug concentrations directly to the disease site Minimizes risk of systemic side-effects Rapid clinical response I Bypass the barriers to therapeutic efficacy, such as poor gastrointestinal absorption and first-pass metabolism in the liver A noninvasive ‘needle-free’ delivery system. Suitable for a wide range of substances from small molecules to very large protein[20, 21] Enormous absorptive surface area (100 meters squared) and a highly permeable membrane(0.2–0.7micrometer thickness) n the alveolar region [22, 23]. Large molecules with very low absorption rates can be absorbed in significant quantities; the slow mucociliary clearance in the lung periphery results in prolonged residency in the lung [72]. Achieve a similar or superior therapeutic effect at a fraction of the systemic dose. For example, oral salbutamol 2–4 mg is therapeutically equivalent to 100–200 Microgram by MDI A less harsh, low enzymatic environment that is devoid of hepatic first-pass metabolism. Reproducible absorption kinetics. Pulmonary delivery is independent of dietary complications, extracellular enzymes and interpatient metabolic differences that affect gastrointestinal absorption [21]. LUNG IS THE ONLY ORGAN THROUGH WHICH THE ENTIRE CARDIAC OUTPUT PASSES BASIC FACTS ABOUT INHALED DRUGS • Optimal site of deposition depends upon infection being treated • Sometimes difficult to deliver to target site due to obstructions resulting from pathologies • • • • Inhalation of drugs for asthma, chronic obstructive pulmonary disease, cystic fibrosis, chronic bronchitis-Common place Inhalation of drugs for diabetes, cancer, migraines, hepatitis C, pain management-In development Therapeutic effect of aerosolized therapies depends upon dose deposited and distribution Surface concentration of drug affects response • Particle size affects deposition • Small particles penetrate more deeply into lung • Larger particles filtered out of upper airways OPTIMAL SITE OF DEPOSITION • • Historically aerosol drug delivery limited to topical therapy for lung and nose Major contributing factor was inefficiencies of available inhalation devices that deposit only 10-15% emitted dose in lung • • • Adequate for doses of steroids and bronchodilators Inadequate for systemic therapies-Systemic therapies require large amounts of drug in order to achieve therapeutic drug levels Design of more efficient systems • MDI • Metered dose inhalers • Pressurized hand-held devices • Use propellants • DPI • Dry powder inhalers • • LPI Advair Diskus • Liquid dose inhalers AEROSOL PARTICLE SIZE • Defines dose and distribution of drug • Heterodispersity • Fine aerosols deposit on peripheral airways but deposit less drug per unit surface area • Larger particle aerosols deposit on central airways and deposit more drug per unit surface area INHALATION OF PROTEINS • 1925-Demonstration that insulin can be absorbed from lung • Macromolecules <40kDa (,5-6nm in diameter) rapidly appear in blood (15-60 minutes after inhalation) • Macromolecules >40kDa are slower to adsorb (hours) MECHANISMS OF DEPOSITION • Inertial impaction • • • • • • • Gravitational sedimentation • • • First 10 generations of lung Tracheobroncial region and bends and bifurcations Air velocity is high Airflow is turbulent Particles >10 microns deposited in oropharyngeal region Delivered by DPI, forward velocity MDI Last 5-6 generations of lung Air velocity is low Diffusion (Brownian motion) • • Alveolar region Air velocity is negligible Hygroscopic drugs swell as they come in contact with humidified air in lung (99.5%) Large porous particles (LPPs) are a drug delivery platform that manipulates particle properties by increasing geometric diameter and lowering particle mass density while maintaining an aerodynamic diameter that allows for entry and deposition in the lungs. LPPs disperse more readily than classical small dense particles of inhaled pharmaceutical formulations, allowing efficient delivery of large drug masses from a relatively simple inhaler. These dry powders are also manufactured inexpensively and at large commercial scales using processes such as spray drying. The result is a free-flowing powder that is shelf-stable and easily delivered in large doses. Drugdeliverytech.com CLEARANCE MECHANISMS • Inhaled drugs (once deposited) are cleared from lungs, absorbed into systemic circulation, enzymatically degraded • Particles deposited in conducting airways removed by mucociliary clearance or absorbed through epithelium (passive diffusion, extracellular pathways, endocytosis) into blood or lymph • • Goblet cells • Submucosal glands • Impaired in lung diseases such as CF and asthma Vanderbilt.edu Particles deposited in alveolar region phagocytosed and cleared by alveolar macrophages or absorbed into systemic circulation • Rate of absorption of proteins is size dependent Nanomedicine BARRIERS TO ABSORPTION • Drug absorption regulated by alveolarvascular permeable barrier • Number of alveoli-200600 million • Enormous surface area • Barriers to absorption • • • • • • Lung surfactant Surface lining fluid Epithelium Interstitium Basement membrane Endothelium MECHANISMS FOR DELIVERY TO BLOODSTREAM • Cell absorptive transcytosis (adsorptive/receptor mediated) • Paracellular transport (bijunctions, trijunctions) • Large transitory pores • Bioavailability of macromolecules deposited in lung 10-200 times greater than nasal or GI values • Due to enormous surface area and very small diffusion distances, slow surface clearance CENTRAL NERVOUS SYSTEM BLOOD BRAIN BARRIER THE BRAIN AND SPINAL CORD WHY IS IT SO DIFFICULT TO TREAT PATHOLOGIES IN THE BRAIN/CNS? Blood Brain Barrier VASCULATURE OF THE BRAIN Blood vessels in human brain. A plastic emulsion was injected into brain vessels and brain parenchymal tissue was dissolved (photo on left). Zlokovic & Apuzzo: Neurosurgery 43(4):877-878, 1998. (provided by permission from Lippincott Williams & Wilkins) Alzheimer’s Assoc. Org. BLOOD-BRAIN BARRIER BASIC ANATOMICAL BARRIER • CNS blood capillaries structurally different from blood capillaries in other tissues • Barrier between blood within brain capillaries and extracellular fluid • Capillaries lack pores that allow rapid movement of solutes from circulation into tissue • Endothelial cell lining lacks fenestrations • Endothelial cells lining vessels are joined by tight junctions • High transendothelial electrical resistance BBB BBB • Micro-vessels make up 95% of total surface area of BBB • • • • 650km, total surface area 12 meters squared Intercellular clefts, pinocytosis, fenestrae- nonexistent Exchange must be trans-cellular Only lipid-soluble solutes can passively cross • Drugs used to treat virtually all brain-related pathologies have been lipidsoluble if administered IV • Exception-lipophilic anti-cancer agents have difficulty entering interstitium due to efflux mechanisms (discussed in later slides) • Areas adjacent to the ventricles have microvessels similar to those found in periphery • • • Circumventricular organs- ex. choroid plexus, neurohypophysis Exchange between cerebrospinal fluid and brain extracellular fluid Enzymes • Endothelial cells contain large numbers of enzymes • Rapidly degrade most peptides THE BBB PRESENTS THE SAME EFFLUX MECHANISM AS THE GI TRACT • Multi-drug transporters • P-glycoprotein (Pgp) active-drug-efflux-transporter protein • Multi-drug resistance protein (MRP) • Multi-specific anion transporter • Luminal membranes of cerebral capillary endothelium • Efflux of drug molecules from endothelial cell cytoplasm before entering brain parenchyma • Active efflux via specific transporters • Efflux of lipid-soluble molecules • Restricting efflux may increase brain exposure to drugs • Co-administration of a competitive or non-competitive inhibitor of the efflux pump together with desired drug • Co-administration of Pgp blocker, valspodor, improves therapeutic effect of paclitaxel in mice. EFFLUX MECHANISM P-GLYCOPROTEIN (PGP) ACTIVE-DRUG-EFFLUXTRANSPORTER PROTEIN BLOOD-CEREBROSPINAL BARRIER CEREBROSPINAL FLUID BATHS THE BRAIN TISSUE AND PROVIDES YET ANOTHER BARRIER TO TRANSPORT INTO BRAIN PARENCHYMA FROM THE BLOOD • Regulation of passage of blood-borne molecules into CSF • Found in epithelium of choroid plexus • Choroid plexus and arachnoid mater act together as barrier between blood and CSF • Choroid plexus very vascular, forms CSF and regulates contents of CSF • Passage of substances from blood through arachnoid membrane prevented by tight junctions • Ependymal cells (choroidal epithelial cells) form continuous sheet around the ventricles • Microvilli, basolateral interdigitations, abundant mitochondria Three layers of meninges Dura mater Arachnoid mater Pia mater CSF located within the ventricles and within sub-arachnoid space Surrounded by ependymal cells that are connected by tight junctions The choroid plexus and arachnoid mater provide barrier to transport between blood (circulating in vessels of arachnoid mater) and CSF in ventricles VENTRICLES OF THE BRAIN IN ADDITION TO MECHANICAL BARRIERS, THE CHOROID EPITHELIUM PRESENT MOLECULAR BARRIERS TO TRANSPORT • • • Fortification by active organic acid transporter system in choroid plexus capable of driving CSFborne organic acids into blood Therapeutic organic acids such as Penicillin, methotrexate (anti-cancer), zidovudine(anti-viral) are actively removed from CSF and are prevented from diffusing into brain tissue Substantial diffusion distance between CSF and brain parenchyma also hinders entry of molecules deep into brain tissue BLOOD-TUMOR BARRIER • CNS malignancies-BBB compromised • Physiological barriers prevent delivery of drugs via cardiovascular system • Inconsistencies in microvasulature of tumor results in spatially inconsistent drug delivery • Vascular surface area decreases as tumor size increases • Intracapillary distances within tumor increase • Increased hydrostatic pressure/interstitial tumor pressure inhibits transport of molecules into tumor GLIOMA DRUG DELIVERY TO THE BRAIN Chemistryworld/Issues INTERSTITIAL DELIVERY INJECTIONS, CATHETERS, PUMPS • • • Ommaya reservoir/implantable pump for intraventricular or intrathecal routes Continuous drug delivery Three pumps available • Infusaid pump • Vapor pressure of compressed Freon to deliver drug solution at constant rate • MiniMed PIMS system • Solenoid pumping mechanism • Medtronic SynchroMed system • Peristaltic mechanism • Epidural delivery device • Depofoam drug delivery system • Epidural delivery of morphine encapsulated in multivesicular liposomes INTERSTITIAL DELIVERY BIODEGRADABLE POLYMER WAFERS AND MICROSPHERES • Direct delivery to brain interstitium using polyanhydride wafers • Conjugation of polymerically delivered chemotherapeutic agents to a water-soluble macromolecule • Increases drug penetration by increasing drug retention • Hanes et al.-IL-2-loaded biodegradable polymer microspheres • Stereotaxic implantation of microparticles containing drug into specific areas of brain • Gliadel-Polymeric delivery system containing BCNU for treatment of glioma patients DELIVERY FROM BIOLOGICAL TISSUE • Implantation of tissue that synthesizes and secretes protein therapeutic agents Encapsulated Neural Grafts • Implantation of embryonic neural grafts for the treatment of Parkinsons Nature Nanotechnology Philip R. LeDuc, Michael S. Wong, Placid M. Ferreira, Richard E. Groff, Kiryn Haslinger, Michael P. Koonce, Woo Y. Lee, J. Christopher Love, J. Andrew McCammon, Nancy A. Monteiro-Riviere, Vincent M. Rotello, Gary W. Rubloff, Robert Westervelt & Minami Yoda Nature Nanotechnology 2, 3 - 7 (2007)