Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
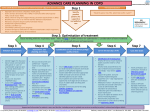
END OF LIFE CARE PLANNING IN HEART FAILURE Some specific disease related indicators of poor prognosis · · · · · · · · · · The Surprise Question Step 1 Advanced age Dependent for more than 3 activities of Daily Living NYHA Class III/IV heart failure, severe valve disease or extensive CAD Refractory symptoms despite optimal tolerated theraoy Resistant hyponatraemia Cardiac cachexia Serum alb <25g/l ≥3 hospital admissions with decompensation in <6 months Experiencing multiple shocks from Implantable Cardioverter Defibrillator (ICD) Comorbidity conferring a poor prognosis eg. terminal cancer “Would it surprise me if this patient dies within 1year?” Identify possible patients for supportive and palliative care KEY Bold underline = hyperlink to more information Step 2: Optimisation of treatment If appropriate, refer via CICS to heart failure services for optimisation / consideration of new treatment options PROCEED IF CONFIRMED END STAGE HEART FAILURE Step 3 Assessment, care planning and review Discussions as end of life approaches · · · · · · · · Identify triggers for discussion Open, honest communication with patient +/- carer of clinical deterioration and palliative status +/- prognosis Begin discussions surrounding preferred place of care and death Identify ICD patient and discuss future deactivation Discuss and document CPR/ DNAR status · · · · · Coordination of care and delivery of high quality services Discuss and document care preferences – regularly review as can change over time Monitor psychological status Regular assessment and review of carer/family needs Document agreed treatment escalation plan – may include use of IV diuretics Medication review – discontinue non-essentials Liaison with Community Heart Failure Nurse Specialists Primary Care management of general symptom control · · Welfare review of benefits and advice Refer to local specialist palliative care services IF complex needs and meets criteria · Anticipatory prescribing · Step 6 Step 5 Step 4 Consent for entry onto Coordinate My Care (CMC) Create CMC record Care in the last days of life · Identification of the dying phase · Priority GP visit to ensure expected deaths avoid need for Post Mortem Review needs and preferences for place of death and accomodate accordingly – may need to update CMC record · Ensure CMC record complete and finalised · Use Gold Standards Framework and include heart failure patients on GP palliative registeres Involve wider MDT and review appropriate health and social care services to meet identified patient and carer needs Ensure patients and carers have the opportunity at all stages of care to discuss issues of sudden death and living with uncertainty · · Symptom control and care for the dying palliative guidelines · · Access to palliative care expertise · Local hospices · · Step 7 · · · Support for patient and carer Consider implementing best supportive care – stop inappropriate interventions Medication review – discontinue non-essentials and consider alternative routes of administration NB absorption of subcutaneous medication given into oedematous tissue may be poor Care after death · Timely verification and certification of death or referral to coroner · Alert undertaker to risk of shock if ICD in situ · Bereavement support for care and family · Update CMC record with date and place of death · Could use GP Gold Standards Framework meetings to reflect and review selected cases as a learning process Bereavement preparation and information for carers about registering a death Support and information for patients, carers and families, including access to spiritual care services according to patient’s cultural and religious beliefs References: For queries please contact Dr Mcdaid: [email protected] (EOLC Lead) Dr Sinha: [email protected] (HF/COPD lead) Pathway created: March 2014 Last Reviewed in: Mar 2016 Review Date: Feb 2019 KEY Bold underline = hyperlink to more information GUIDELINES FOR SYMPTOM CONTROL IN END STAGE HEART FAILURE GENERAL ADVICE · · · · · · Continue symptom control alongside optimised active cardiological management until such becomes inappropriate Ensure patient concordance with medication (eso diuretics) to optimise symptom control AVOID contraindicated medications Treat reversible precipitants of symptoms if patient deteriorates (LRTI, non-compliance, anaemia, thyrotoxicosis, MI, arrthymia) as appropriate MDT approach – physio, OT, social worker, spiritual care services, pharmacist Seek advice from specialist palliative care · · · PAIN · · · · · · · · · Up to 80% of patients with heart failure experience pain 1 Assess all pain and treat accordingly Investigate further – where appropriate Screen for concomitant psychological factors – low mood, anxiety, meaning of disease progression, fears re future and dying MDT approach – physio, OT, social worker, spiritual care services, pharmacist Pharmacological management – see pocket guide, WHO ladder and CPR NB NSAIDs can lead to increased fluid retention and worsening of heart failure Give patient information leaflet if starting opiate NB morphine undergoes renal excretion, monitor closely for toxicity – frequency/dose of morphine may need to be reduced, or use of alternative opioid – seek advice from specialist palliative care team Consider prophylactic laxatives · · · · · · · · Pharmacological management – see pocket guide NB Cyclizine may worsen heart failure References: NICE guidelines [NG31] Care of dying adults in the last days of life NHS England - Actions for End of Life Care 2014-2016 · · Pharmacological management – IF above measures not optimised symptoms, consider escalating heart failure medication, ask for a review by the community heart failure team · · · Morphine Sulphate IR (Oramorph) (10mg/5ml) starting dose 2.5mg PO 4hrly and PRN – seek specialist advice before initiating, give patient information leaflet re opiates, titrate dose every 48hrs according to effectiveness and tolerance, monitor for opiate toxicity For patients already on a strong opioid, intolerance to morphine, or with significant renal impairment (eGFR <30mL/ min or Cr >150micromol/L), contact the local specialist palliative care team for advice · Non-pharmacological management – explore concerns, ask about sleep (general anxiety and death phobias often worse at night), ask about mood, investigate current support networks, consider referral to OT/psychological support/ complementary therapy Pharmacological management – see CPR; Antidepressants – SSRIs 1st line, Fluoextine/ Citalopram 20mg PO OD AVOID TCAs in view of cardiotoxicity DON’T STOP/CHANGE established antidepressants if not causing harm Night sedation – if non-pharmacological management ineffective, see CPR Anxiolytics – Lorazepam 500mcg – 1mg (1mg tablet supply) S/L PRN (max dose 4mg/day) – regular monitoring as risk of sedation and addiction, seek advice from specialist palliative care team COUGH · · · · · Pharmacological management; 1st line: Codeine linctus 5-10mls PRN (max dose QDS, AVOID/STOP if already on an opiate) 2nd line: Morphine Sulphate IR (Oramorph) (10mg/5ml) starting dose 2.5mg PO 4hrly/PRN, AVOID if already on regular opiate Normal Saline nebulisers – on specialist palliative care advice, helps loosen tenacious mucus and aid expectoriation Assess for any underlying cause – oxygen, medication, PO thrush Treat reversible causes Sucking on ice cubes, chew sugar-free gum – stimulants Sip pineapple juice/suck chunks – if coated tongue IF ABOVE MEASURES INEFFECTIVE, BioXtra gel I TOP PRN · · · · CONSTIPATION · · · Causes – reduced PO intake, diuretics, poor mobility, opioids Address reversible factors if possible Pharmacological management – see pocket guide and CPR PERIPHERAL OEDEMA · · · Lorazepam 500mcg – 1mg (1mg tablet supply) S/L PRN (max dose 4mg/day) – regular monitoring as risk of sedation and addiction, seek advice from specialist palliative care Causes include underlying heart failure, ACE Inhibitors (only consider stopping if persistent cough, substitute with ARB – Losartan), other eg LRTI · MENTAL HEALTH · · NAUSEA/VOMITING Multiple causes – consider measuring U&Es and calcium Treat reversible factors – if appropriate May be due to disease progression – consider escalating heart failure medication in consultation with the heart failure team Iatrogenic – discontinue precipitant medication Consider other causes of breathlessness – psychological, concomitant medical problems (LRTI, COPD, anaemia, PE) and treat if/as appropriate Non-pharmacological management – consider referral to local hospice day therapy unit – relaxation and breathing exercises, lifestyle adjustments, psychological support, complementary therapies, open windows, handheld/bedside fan CACHEXIA AND ANOREXIA · · DRY MOUTH BREATHLESSNESS · · · Exclude potentially reversible causes eg n/v, depression, shortness of breath, uncontrolled pain Oedema can mask loss of lean body mass Regular assessment and referral to dietician if indicated STOP unnecessary medications to alleviate tablet burden · · · · Ensure fluid and salt intake not excessive Leg elevation Caution with compression bandaging – can cause skin damage and increase venous return Lymphorrhea – gentle bandaging and advice from Tissue Viability/District Nurses Scrotal supports – need referral by hospital consultant to Surgical Appliances Manage expectations and educate as to cause · Pharmacological management – diuretics, ensure concordance Skin care – regular emollients · · · · · Use of a syringe driver Terminal secretions Agitation Pain Breathlessness END OF LIFE CARE Pathway created: March 2014 Last Reviewed in: Mar 2016 see pocket guide Review Date: Feb 2019