Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
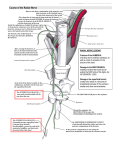
Musculoskeletal Imaging and Intervention Section Imaging Procedures LUMBAR AND SACRAL NERVE ROOT BLOCKS INDICATIONS Nerve Root blocks are commonly requested in patients with radicular symptoms for two broad general indications: 1. Diagnostic Injections: a. Imaging studies are normal do not show abnormality to explain the distribution of symptoms). b. Imaging studies show multiple levels of pathology so it is difficult to know which level(s) is responsible for the symptoms. c. Both hip and spine pathology are present and either or both may be the cause of the leg symptoms. 2. Therapeutic Injections: The anesthetic and steroid injection is desired to treat the pain generator. This will make the patient more comfortable and functional until the symptoms resolve or surgery is necessary. RISKS • Hematoma • Infection • Allergic reaction • Pain • Nerve injury • Reflex sympathetic dystrophy • Transient weakness or paresthesia MATERIALS • 4 x 4 gauze, alcohol, betadine, small steridrape • 5 cc syringe • 10 cc syringe (2) • Short iv hep lock connecting tubing • 1% lidocaine, preservative free • 25G 11⁄2” needle • 22G 31⁄2” needle • Omnipaque 300 • Celestone 6 mg/cc or Kenalog 40 mg/cc • Bupivacaine 0.5% preservative free PREREQUISITES • Patient must have driver to get home. • Review the patient’s cross sectional imaging studies. • Check request and be certain of the exact nerve root the referring clinician would like injected. Correlate with MRI findings. • Discuss the procedure with the patient: a. Explain that they will likely experience transient radicular pain as the inflamed nerve root is approached. b. Explain the diagnostic and therapeutic aspects of the procedure. c. Explain a “pain diary” for the patient to keep for their doctor. d. Obtain signed consent. TECHNIQUE - For Lumbar Nerve Blocks 1. Place patient in the prone position, no bolster is required. 2. Profile the disc at the level to be injected 3. Roll the tube toward the side to be injected until the inferolateral corner of the vertebral body is uncovered by the most lateral margin of the superior articular facet. Target 2 mm above the inferior endplate and 4 mm medial to the lateral cortical margin of the vertebral body (Figures 1 and 2) 4. Prep alcohol, betadinex3), small steridrape and towels, local 1% lidocaine, preservative free with 1 1⁄2” 25G needle. 5. Insert a 3.5” 22 G needle at the site marked. Advance in the AP view occasionally checking in the lateral view to determine depth and confirm proper craniocaudal angulation. 6. Once the needle tip reaches the posterior margin of the neural foramen, all additional advancement will be in the lateral view. 7. From this point the patient is asked to report any subsequent leg or buttock pain. The needle is incrementally advanced in 1 mm steps until the patient feels radicular pain. If the patient does not feel any pain, the end point on the lateral view is approximately 2 mm within the posterior cortex of the vertebral body. 8. In the true AP projection, the stylet is removed and a 5 cc syringe of Omnipaque 300 attached via short IV hep lock connecting tubing (capacity of tubing is 0.2 cc). A small amount of contrast is injected producing a neurogram extending inferolaterally from the neural foramen. Image pending Fig 1: Start position Image pending Fig 2: End position. Fig 3: L4 neurogram, AP. 9. Disconnect the syringe with contrast from the tubing. This minimizes any manipulation of the properly positioned needle tip. Shake the syringe with the therapeutic solution to resuspend the particulate steroid component before attaching to the tubing. 10.Inject 1.5 cc of equal parts Kenalog-40 and 0.5% preservative free Bupivacaine and take a spot film. It is not uncommon for the patient to report increased pain during the injection; this can usually be mitigated by a short waiting period or decreasing the rate of injection. If no neurogram is produced by the contrast injection, flood the area with 2.0 cc of the therapeutic solution for a perineural block. 11.Discuss a “pain diary” with the patient. Alternative Methods for Lumbar Nerve Blocks 1. Oblique tube about 45° until the superior articular process is about in the middle of the disc in the AP direction. Aim the needle with tower until tipis 2-3 mm inferior to the eye of the Scotty dog at the 6 o’clock position. Alternative method #1: 45o oblique. Direct needle directly down to the •, 2-3 mm beneath the 6 o’clock position of the pedicle, until paresthesias occurs. TECHNIQUE - Sacral Nerve Block 1. The S1 nerve root is the most common sacral nerve root we are asked to inject. 2. After exiting the spinal canal, the nerve travels in a common neural foramen which bifurcates into anterior and posterior branches. The portion of the nerve we wish to block is the anterior division. 3. Review the patient’s cross sectional study to see if it includes the S1 neural foramen on the affected side. Make note of the angle of entry into the posterior branch. Typically this will be between 10 – 20 degrees with 15 degrees being most common. 4. Position the patient prone without a bolster. 5. Roll the tube out to the predetermined angle and look for a faint circle just below the S1 pedicle representing the posterior neuroforamen (Figure 4) Fig 4: Sacral nerve block start position, slight larteral angulation 6. This is usually accomplished without cranialcaudal angulation as the posterior neuroforamen is oriented caudally but the upper sacrum is tipped dorsally about the same amount. 7. Target the center of the properly positioned neural foramen and place a 31⁄2” 22 G spinal needle. 8. On the lateral view the endpoint is 2-3 mm inside the anterior cortex of sacral canal (Figure 5). Fig 5: Sacral nerve block, lateral. 9. At this level, confirm positioning with a small injection of Omnipaque 300 in the true AP projection and take a spot film (Figure 6). Fig 6: Sacral nerve block, AP. 10.Flood the area with 1.5-2.0 cc of equal parts Kenalog-40 and 0.5% preservative free Bupivacaine and take a spot film. • For a sacral nerve block, angle the tube towards head 25-45° until the anterior and posterior aspects of the foramen form a well-defined circular lucency and mark the skin over the foramen superiorly, 2-3 mm under the pedicle.