Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
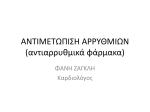
CLINICAL MONITORING OF ANTIARRHYTHMICS IN CRITICAL CARE By Jean-Luc Beaumont, nurse-clinician specialized in cardiovascular and respiratory nursing Antiarrrhytmics are an important pharmacological class of drugs used in cardiology. The objective of this article is in particular to provide a greater understanding of the mechanisms of action of antiarrhythmics and, consequently, the clinical monitoring of expected outcomes. This article is divided into two parts. The first part, electrophysiology, illustrates the relationship between the action potential of the myocardial fiber and the point of impact of antiarrythmics. The second half, antiarrythmics, provides a classification of antiarrhythmics as well as the mechanisms of action of each class of antiarrythmics and their particularities, including clinical monitoring. PART ONE: ELECTROPHYSIOLOGY In the myocardium, there is a system of specialized fibers which differ from contractile fibers. Those fibers make up the nodal tissue and are composed of two types of cell populations. Automatic cells generate cardiac impulses (automaticity). Conductive cells propagate impulses through the conduction system (conductivity). The set of cells reacts to a stimulus (excitability). These three properties make up the core of the cardiac intrinsic nervous system (CINS). In addition, certain afferent fibers (sensitive) connected to the electrical conduction system of the heart have an influence over cardiac electrophysiology. The sympathetic system, under the influence of adrenaline, and the parasympathetic nervous system, activated by acetylcholine, make up the extrinsic nervous system and allow it to regulate the functioning of the heart. The electrical activity of the heart is generated by strong ionic concentrations disseminated throughout the cell membrane. A significant disruption in transmembrane ionic transfer is a precursor of arrhythmias. The electric potential, the work and rest activity of the cell, is recorded using micro-electrodes placed across the cellular membrane. The electric potential produces a typical image called an action potential (Figure 1). 1 Figure 1: Phases of the action potential and transmembrane ionic flow Source: J.-L. Beaumont (2006) The action potential is subdivided into five phases (Figure 1). Phase 0, the first phase, corresponds to cell activation or depolarization. The impulse is propagated to neighbouring cells thanks to an avalanche of sodium ions (Na+) which penetrate the cell and favour automaticity. Those ions rapidly circulate along the Na+ rapid-response fibers through specific channels. This type of fiber which emits a sodium current mainly serves to activate the functioning of the atrium, the His-Pukinje system and the ventricular muscle fibers (Figure 2). The medications which are likely to inhibit Na+ entry (phase 0) into the cell belong to Class 1 antiarrythmics, also known as sodium channel blockers (Table 1). Phase 0 corresponds to the QRS complex on the surface ECG (Figure 3). Phases 1 and 2, the second and third phases, of the action potential correspond to the initial repolarization of the cell. Sodium inactivation leaves room for calcium entry into the cell. During these phases, the speed at which repolarization occurs diminishes because of the intracellular exit of potassium channelling outside the cell. This calcium current influences in particular the functioning of slow response fibers located in the sinoatrial node and in the atrioventicular node (Figure 2). During supraventricular tachychardia, the calcium blockers are choice indicators 2 because those arrhythmias arise along the boundaries of fibers whose calciumtype action potential significantly influences the heart rate for the sinoatrial node and the atrioventicular (AV) conduction for the AV node. The medications which are likely to inhibit Ca+ entry (phase 0) into the cell belong to Class 4 antiarrythmics, also known as calcium channel blockers (Table 1). Phases 1 and 2 of the action potential correspond to the ST segment on the surface ECG (Figure 3). Phase 3, the fourth phase of the action potential, corresponds to the terminal repolarization of the cell. This phase results from an outward potassium (K+) current which increases the duration of the action potential. At this stage, the fiber recovers its initial rest charge. This phase corresponds to the T wave on the surface ECG (Figure 3). Certain conditions may occasionally require controlling the exits of intracellulaar potassium. This has the effect of extending the duration of the action potential and, consequently, of the QT interval on the surface ECG (Figure 3). The medications which alleviate the exits of K+ in the cell make up Class 3 antiarrythmics known as potassium blockers (Table 1). Phase 4, the fifth phase of the action potential, is the time interval between two action potentials. At this stage, the cell has recovered its rest potential or membrane potential linked to the role of sodium and potassium. Enzymes help provide the cell with the necessary energy for transmembrane ion exchanges. Schematically, a heart beat can be superimposed over an action potential. Phase 4 of the action potential determines the heart rate. The shorter a phase 4 action potential, the greater the action potential in a minute and the greater the number of heart beats per minute. By comparing the action potentials of pacemakers (sinoatrial node, bundle of His and the Purkinje fibers), the phase 4 of the sinoatrial node is the shortest, which explains the dominance of the sinoatrial node, hence the expression sinusal rhythm. Phase 4 corresponds to the end of the T-wave and the beginning of the QRS complex on the surface ECG (Figure 3). The sympathetic and parasympathetic systems interfere directly on the heart rate and on AV conduction. Medications acting on phase 4 of the action potential make up class 2 antiarrythmics, known as beta-adrenergic receptor blockers or beta blockers (Figure 1). 3 Figure 2: Electrical conduction system of the heart Figure 3: Correlation among transmembrane ion movements, the action potential and the surface ECG 4 PART TWO: ANTIARRYTHMICS Antiarrythmics act one way or another on the phases of the action potential by modifying the permeability of the myocardial membrane to sodium, calcium and potassium ions. They are subdivided into four classes according to the Vaughan Williams classification (Table 1). Even though digitalis and adenosine have antiarrythmic properties, they will be the subject of a complementary presentation. Class I: Sodium Channel Blockers Sodium current fibers activate the depolarization of the atrial fibers, of the His-Purkinje system and of the ventricular fibers. The substances which are likely to reduce the depolarization of those fibers are the key elements of this pharmacological class. The common substances belonging to this class include procainamide (Pronestyl®) and flecainide (Tombocor®). Procainamide (Pronestyl®) is a choice indication for the pre-excitation syndrome which is symptomatic of types such Wolff-Parkinson-White (WPW). During this syndrome, the pulse circumvents the nodohisian pathway (His node) to reach the ventricles via abnormal/accessory pathways which may favour major ventricular arrhythmias. Procainamide slows depolarization down and, consequently, the conduction of accessory pathways, which protects the ventricles. Clinical monitoring of the intravenous administration principally aims to detect any reduction in the heart output, checking the vital signs, and monitoring arrhythmias for emergency treatments. The effect on cell repolarization can lead to an increase in the intervals of the QRS complex and the QT interval. Any duration of the QRS complex that is superior to its initial value by 25% and any duration of the QT interval which is superior by 0.44 seconds must be reported. Flecainide (Tambocor®) is the most powerful antiarrhythmic of this class. Its effects are an extension of cell depolarization time (phase 0) of the atrium, Purkinje network and ventricle. A reduction in intraventricular conduction velocity can be observed. Flecainide is particularly efficient in the absence of coronary artery disease for treating frequent premature ventricular contractions (PVC) Clinical monitoring involves the checking of vital signs, detecting the extension of the QRS interval on the ECG, and monitoring major arrhythmia events. Increased surveillance is required when a bundle branch block occurs. Flecainide is counter-indicated among people suffering from coronary disease because it favours PVCs and ventricular tachycardia. 1 Class II: Beta-Adrenergic Receptor Blockers or Beta-Blockers These substances are an efficient competitor of catecholamines (noradrenaline, epinephrine, adrenaline) because they occupy the receptor sites of these chemical mediators. These receptors are subcategorized into Beta-1 and Beta-2. The Beta-1 adrenergic receptors are found in significant numbers in the heart; consequently, they have a positive influence on automaticity, conductibility, excitability and contractility. Beta-2 are predominant in the airway smooth muscle whose dominant effect is bronchodilation. The principal action mechanism of beta blockers consists in inhibiting the cardiac stimulation of the beta-adrenergic receptors (sympatholytic effect) This action is carried out by an extension of the phase 4 of the action potential. The sympatholytic effect on the heart leads to a decrease in the heart rate (negative chronotropic effect), an extension of the conduction time (negative dromotropic effect), a lower contraction force (negative inotropic effect). In addition, automaticity is also altered (negative bathmotropic effect). All beta blockers are essentially identical as regards cardiovascular therapeutic effects. Certain beta blockers are cardioselective, meaning that they specifically act on Beta-1 receptors while inhibiting as little as possible the Beta-2 receptors, an important advantage for clients suffering from bronchopneumopathies. The following beta blockers share this property: acebutolol (Sectral®), atenolol (Tenormin®), bisoprolol (Monocor®), metoprolol (Lopressor®). Considering the depression effect on the sinus, the AV node and the ventricular functioning, the side effects of beta blockers could be exacerbated when combined with substances whose negative bathmotropic, chronotropic and dromotropic effects are similar such as: amiodarone (Cordarone®), diltiazem (Cardizem®), flecainide (Tambocor™) and verapamil (Isoptin®). Clinical monitoring is mainly based upon detecting symptomatic bradycardia, signs and symptoms of low output syndrome and the extension of the PR interval. It remains essential to check the vital signs. Concomitant medication deserves special attention because it favours excessive bradycardia. 2 Class III: Potassium Channel Blockers Pharmacological substances belonging to this class block the intracellular exits of potassium during phase 3 of the action potential. Repolarization thereby being extended, certain re-entry arrhythmias associated with scar tissue can be inhibited because the refractory or protection period is increased (Figure 3). The outcome of this action mechanism leads to an increase in the QT interval. Substances belonging to this class include: amiodarone (Cordarone®) and sotalol (Sotacor®). Amiodarone (Cordarone®) is a powerful antiarrhythmic which prolongs the refractory period and the repolarization of all cardiac tissues including the accessory pathways during the pre-excitation syndrome. Because this substance groups together four classes of antiarrhythmics, amiodarone indeed is the star of antiarrhythmics. It is the drug of choice for ventricular tachychardia in cardiac emergencies. The decrease in the heart rate (Class IV); the extension of the PR (Class II) QRS (Class I) and, especially, QT (Class III) intervals are predictable electrocardiographic effects of amiodarone. Sinus bradycardia conjugated with the extension of the QT interval make up the pro-arrhythmic factors which are likely to favour torsades de pointes (lit. “twisting of the points”). Clinical monitoring consists of checking the vital signs and detecting any extension of the PR, QRS and QT intervals. Amiodarone potentializes the effect of warfarin (Coumadin®) and doubles the plasmatic concentration of digoxin. By its iodine content, it can affect the functioning of the (hypo – hyper) thyroid gland. Potentially significant side effects include liver damage, the formation of corneal micro-deposits (perception of halos around lights), photosensitivity and a risk of developing pulmonary fibrosis. Sotalol (Sotacor®) also has the properties of a non-selective beta-blocker. It is administered orally in the treatment of supra-ventricular and ventricular arrhythmias without heart injury. The torsade de pointes effect is reported in the range of 4%. 3 Class IV: Calcium Channel Blockers Phase 2 of the action potential corresponds to the plateau of the action potential. During this phase, the calcium current leaves its mark in particular on the fibers of the sinoatrial node and of the AV node by inhibiting the entry of calcium ions, which slows down depolarization. The most dominant effects are a reduction in the heart rate and in AV conduction; furthermore, the calcium blockers are cardiodepressive. Antiarrhythmics belonging to this class include diltiazem (Cardizem®) and verapamil (Isotopin®). These medications are used in the symptomatic treatment and/or diagnosis of symptomatic supra-ventricular tachycardia. The negative chronotropic and dromotropic effect of these substances is desirable. Hypotension arises from the relaxation of the smooth musculation of vessels. Diltiazem has an elimination half-life of 3 to 7 hours and a reduction in the heart rate appears within 2 to 7 minutes following bolus administration. The elimination half-life of verapamil may vary from 3 to 7 hours and the negative dromotropic effect occurs within 2 minutes following the bolus administration of the medication and lasts for 15 to 20 minutes. The bolus administration of these medications must be made at the proximal site and followed by a bolus of 20 ml of NaCl. Clinical monitoring consists of checking the vital signs and monitoring cardiac arrhythmias which are predictable owing to the bradycardia and the extension of the PR interval. The detection of cerebral hypoperfusion signs and symptoms must be reported. Other Antiarrhythmics: Digoxin (Lanoxin®) and Adenosine (Adenocard®) Even though digitalis is known for its antiarrhythmic properties and its sympatholytic activity, it is a cardiotonic agent which is primarily indicated for heart failure. Adenosine exists in every cell of the organism and is not related to the antiarrhythmics presented herein. Intravenous administration increases potassium currents which also impede the entry of calcium into the heart muscle. Adenosine is an antagonist of the sympathetic system as regards the action potential of the ventricular myocardium. The negative chronotropic and dromotropic effects on AV conduction are the major effects of this medication. 4 Adenosine is a primary choice of intervention for symptomatic surpraventricular tachycardia. The post-administration therapeutic response can be evaluated within 30 seconds. The elimination half-life inferior to 10 seconds and the complete excretion of the medication within 30 seconds are among the significant advantages of this medication. Adenosine is counter-indicated among asthmatic patients. Clinical monitoring requires rapid administration, 1 to 2 seconds, because a slower administration may trigger reflex tachycardia. The bolus administration of this medication must be made at the proximal site and followed by a bolus of 20 ml of NaCl with the member elevated. The checking of vital signs and the detection of arrhythmias, in particular pauses and conduction anomalies consecutive to sinoatrial node depression and the extension of AV conduction, are essential. The heart rate and PR interval must be recorded as well as any medicine-related post-administration symptom such as: hot flashes, histamine flush, dyspnea and tightness of the chest. These symptoms generally do not exceed one per minute. Understanding, on the one hand, the action mechanisms which regulate the action potential of the cardiac fiber and, on the other, the impact points of antiarrhythmics justifies an optimal clinical monitoring of the clientele which responds to the indications of this pharmacological class which is widely used in cardiology. References Beaumont, J.L. (2006). Les arythmies cardiaques un guide clinique et thérapeutique (5e édition). Montréal : Chenelière Éducation. * We hereby thank Dr. Marcel Gilbert, cardiologist and rhythmologist, of the Institute de cardiologie de Québec, for supervising this article. 5 FIGURE 4: CLASSIFICATION OF ANTIARRHYTHMICS CLASS ACTION MECHANISMS CLASS I Sodium channel blockers CLASS II Beta-adrenergic receptor blockers or beta blockers CLASS III Potassium blockers CLASS IV Calcium channel blockers Blocks the rapid entry of sodium Acts on phase 0 of the action potential Slows down the depolarization and amplitude of the action potential in rapid-conduction cells: Atrium, His-Purkinje system and ventricular muscle Raises the equilibrium potential Sympatholytic effect Extends: phase 4 of the action potential the refractory period of the AV node Decreases: Sinusoidal rate AV conduction Blocks the potassium current Acts on phase 3 of the action potential Prolongs repolarization Potential pro-arrhythmic effect Blocks the entry of calcium Acts on phase 2 of the action potential, in particular on the sinoatrial node and the AV node Reduces the conduction velocity in the AV node Slows down the heart rate MEDICATIONS Procainamide: Pronestyl® Flecainide: Tambocor® Acebutolol: Sectral® Atenolol: Tenormin® Bisoprolol: Monocor® Metoprolol: Lopressor® Amiodarone: Cordarone® Sotalol: Sotacor® Diltiazen: Cardizen® Verapamil: Isoptin® 6