Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
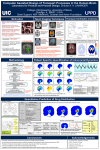
Case History o 29 year old Caucasian Female o Chief complaint: Headaches occurring 2-3 times per week, with recent increase in frequency to almost daily. She also complained of transient loss of vision upon waking, onset 6 months ago o Medical History Morbid Obesity: BMI 48.32 kg/m2 o Ocular History High Myopia o Current Medications Advil as needed for headaches Pertinent Findings o Comprehensive Eye Exam and Follow Up Examinations Best Visual Acuity with Refraction Right Eye -9.50 -1.50 178 20/25 Left Eye -9.00 -0.75 125 20/20-2 Pupils round and reactive to light, without afferent pupillary defect Anterior Segment Health: unremarkable Posterior Segment Bilateral asymmetric optic disc edema (Fundus photography performed) Choroidal folds in the left eye adjacent to optic nerve head Blood Pressure: 121/78 mmHg Seated Visual Field Results Right Eye: Mildly enlarged blind spot with scattered temporal defects Left Eye: Enlarged blind spot in with temporal defects o Neurology Consult MRI results: No space occupying lesions, empty sella, enlargement of optic nerve sheaths Labs Thyroid stimulating hormone (TSH) 1.53uU/L (normal) Glycosylated hemoglobin: HbA1C 6.1% (High) Lumbar Puncture and Labs Opening Pressure 260 mm, with the following labs performed on CSF Abnormal Normal RBC count: 1 cell (high) White Blood Cell Count Glucose 96mg/dL (High) Serum Bands CSF Bands Olig Bands Interpretation Cells Counted: 100 Lymphocytes: 58% Monocytes: 42% Protein 21mg/dL VRDL: Non-Reactive ACE: 1.7 U/L Lyme: Negative Differential Diagnosis o Primary: Idiopathic Intracranial Hypertension o Intracranial Mass or lesion o Malignant Hypertension 1. Reierson o Neuroretinitis Papillitis1 Diagnosis and Discussion o Idiopathic Intracranial Hypertension is unique because it is a diagnosis of exclusion. No definitive test gives a positive result to IIH therefore, all differential diagnosis of optic nerve head edema must be ruled out7 o Epidemiology of IIH Most common demographic: overweight women of child bearing age Incidence increases by percent overweight 0.9-1.07 per 100,000 in the U.S. 13-14.9 per 100,000 in patients 10% over ideal body weight 15-19 per 100,000 in patients greater than 20% over ideal weight2 Symptoms observed in IIH Headaches found in 84-92% Transient visual obscurations: recovery within seconds seen in 68-72% Double vision associated with abducens palsy occurred in 18-38% Photopsia seen in 48-54% Visual field loss occurred in 26- 32% Pulsatile tinnitus found in 52-60% of patients, which seems to be the most diagnostic symptom of IIH3 Ophthalmic Clinical Signs Optic nerve head edema Visual Field Loss Unilateral or bilateral abducens palsy2 o Imaging Magnetic Resonance Imaging of Brain and Orbits Rule out secondary cause of increased intracranial pressure o Hydrocephalus o Intracranial Mass or lesions o Causes of over-production or decreased outflow of cerebral spinal fluid o Venous outflow obstruction4 Possible MRI findings in IIH o Empty sella tursica o Flattening of posterior aspect of globe o Distention of perioptic subarachnoid space o Transverse venous sinus stenosis2 Magnetic Resonance Venography (MRV) Rule out venous conditions not well defined with MRI o Venous sinus occlusions o Cerebral venous sinus thrombosis o Arteriovenous fistulas2 o Lumbar Puncture with Cerebral Spinal Fluid (CSF) Analysis Opening pressures measurements indicating increased CSF ≥200mm in adults ≥250mm in obese adults ≥280mm in children2 CSF Analysis to rule out other causes of increased intracranial pressure o 2. Reierson CSF composition Protein levels Abnormal cytology Causes of infection5 o Other diagnostic testing Blood Pressure: should be taken to rule out malignant hypertension Blood testing may not be necessary depending on the tests performed on the CSF analysis. Lyme Testing (if in endemic area) CBC with Differential –infectious causes Fasting blood sugar –diabetic papillitis ACE – sarcoidosis VDRL- syphilis ANA – auto immune 1 o Diagnosis of IIH follows Modified Dandy Criteria Signs and symptoms of increased intracranial pressure Absence of findings on neurological evaluation7 exception 6th nerve palsy2 Absence of deformity, displacement, or obstruction of the ventricular system except for evidence of increase cerebral spinal fluid pressure. No other abnormal evidence on imaging except for empty sella turcica, optic nerve sheath with filled out CSF space, and smooth walled non flow related venous sinus stenosis or collapse. Awake and alert patient No other cause of increased intracranial pressure present 3,7 o This patient meets all of the modified Dandy criteria to be diagnosed with IIH Treatment, Management o Weight Reduction by 5-10% decreases IIH symptoms Gastric Surgery: 90% of patients who lost weight with bariatric surgery noticed significant improvement or resolution of IIH symptoms 6 o Medications Acetazolamide: carbonic anhydrase inhibitor reduces CSF production Dosing 500 mg BID, and increased dosing as tolerated by patient and if symptoms aren’t improving up to 2-4 g per day3 Loop Diuretics: 20-40 mg/day Reduces ICP by decreasing sodium transport7 Topiramate: Titrate up to 150 mg daily No studies have proven topiramate to decrease ICP, but can help with headaches2 o Surgical Intervention Indication Patients don’t improve on medication alone Progressively visual field loss Visual Acuity Loss 5 Types of Surgical Intervention Optic Nerve Sheath Fenestration: Longitudinal slits are cut into the dura to relieve pressure on the retrolaminar portion of the optic nerve. o Preferred treatment for patients with visual field loss o 30-50% of patients showed improvement with headaches o Patients may need additional surgical intervention as they may progress6 Venous Sinus Stenting: A stent is placed inside the transverse venous sinus to help avoid the narrowing 3. Reierson o 90% of IIH patients have transverse cerebral venous sinus stenosis, it is unclear at this time the significance of this correlation o 15/16 patients in a clinic trial who received this surgery the papilledema either resolved or symptoms improved o Headaches were still a problem in these patients, but 80% saw a reduction in severity and frequency o Requires antiplatelet therapy post-surgery, but has low complication rate7 Shunting Ventriculo-Peritoneal or Lumbo-Peritoneal: A shunt is placed to redirect the cerebral spinal fluid, which decreases the ICP o 95% percent of people saw improvement in headaches after procedure but 86% of the shunts failed6 Cranial Decompression: A portion of the skull is removed to reduce ICP o Usually not performed until all other surgical options failed6 o The patient was told to lose weight and has titrated up to 2 g of acetazolamide over the past six months without improvement or resolution. Serial perimetry has been performed to monitor visual field changes, there has been no progression or improvement in visual field loss No improvement in headaches or decreased edema of the optic nerves Currently, she is being evaluated for bariatric surgery and has declined venous shunting procedures, she also is starting to have paresthesia as a side effect to the acetazolamide Bibliography 1. Friedman, Neil J., Peter K. Kaiser, Roberto Pineda, and Peter K. Kaiser. "Chaper 10 Optic Nerve and Glaucoma." The Massachusetts Eye and Ear Infirmary Illustrated Manual of Ophthalmology. 3rd ed. Philadelphia, PA: Saunders/Elsevier, 2009. Print. 2. Idiopathic intracranial hypertension. In DynaMed Plus. EBSCO Information Services. http://www.dynamed.com/#topics/dmp~AN~T114203/Idiopathic-intracranialhypertension#General-references-used. Updated June 16, 2014. Accessed Aug 10th, 2015. 3. Kattah, Jorge C., John H. Pula, Luis J. Mejico, Michael P. Mcdermott, Mark J. Kupersmith, and Michael Wall. "CSF Pressure, Papilledema Grade, and Response to Acetazolamide in the Idiopathic Intracranial Hypertension Treatment Trial." Journal of Neurology J Neurol (2015):. Springer. Web. 10 Aug. 2015. 4. Lee, Andrew G., and Michael Wall. "Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) Clinical Features and Diagnosis." UpToDate. Wolters Kluwer Health, July 2015. Web. 10 Aug. 2015. 5. Lee, Andrew G., and Michael Wall. "Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) Prognosis and Treatment." UpToDate. Wolters Kluwer Health, July 2015. Web. 10 Aug. 2015. 6. Spitze, Arielle, Amina Malik, and Andrew G. Lee. "Surgical and Endovascular Interventions in Idiopathic Intracranial Hypertension." Current Opinion in Neurology 27.1 (2014): 69-74. Lippincott Williams & Wilkins. Web. 10 Aug. 2015. (7) 7. Wall, Michael. "Idiopathic Intracranial Hypertension." Neurologic Clinics 28.3 (2010): 593-617. Clinical Key. Web. 10 Aug. 2015. Conclusion o In any case of disc edema where IIH is suspected, an MRI should be performed first, if normal, a lumbar puncture should be performed. o Idiopathic intracranial hypertension is a complex disease with multiple management techniques which all have risks and benefits o Each case has to be handled individually and tailor the course of treatment specifically for each patient 4. Reierson