Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
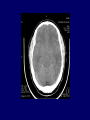
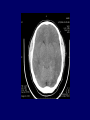
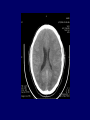
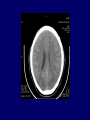
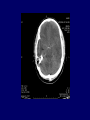
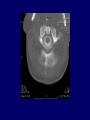
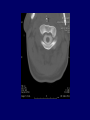
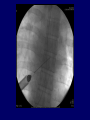
Case Presentation: Neurology/Neurosurgery Grand Rounds February 28, 2006 Gabriel Zada, MD Christopher Aho, MD Neurosurgery Blue LAC-USC Medical Center Patient G.P. • • • • • • • • • • History of Present Illness: 44-year-old Latino man Complains of progressive headache x 2-3 months Headache worse throughout course of day Developed nausea/vomiting 1-2 weeks prior to admission Intermittent double vision, dizziness Hit head while working 6 months ago, but symptoms developed much later No sensory or motor complaints Denies fevers, chills Denies seizures History (continued) • Past Medical History: None • Past Surgical History: None • Medications: Tylenol, Ibuprofen for Has • Allergies: None known • Social History: – Works for pool chemical company – Smokes ~ 5 cigarettes/day – Denies alcohol or other drugs Physical Examination Mental Status: – Awake, alert, oriented to person, place, time, and situation. Speech fluent. Cranial Nerves: – Right partial 3rd nerve palsy (x 1 day) • Pupil 75mm, sluggish. • Partial ptosis. • No oculomotor deficit. – Left pupil 53mm, brisk. – Face symmetric – Cranial nerves otherwise intact. Physical Examination • Motor: – Tone Normal – No pronator drift – Power 5/5 in all extremities • Reflexes: – 2+, symmetric throughout – No Hoffman’s sign – Toes downgoing bilaterally • Sensory: – Sensation intact in all extremities. • Cerebellar/Gait: – Finger-nose-finger normal. Gait exam deferred. Head CT Initial Hospital Course • Developing concern that patient had increased intracranial pressures and brainstem herniation • Mannitol trial Right 3rd nerve palsy improved • Emergent neurosurgery consult requested • Initial concern per neurosurgery for subarachnoid hemorrhage and ruptured P-Comm aneurysm • Nimodipine + increased intravenous fluids started empirically • Emergent cerebral angiogram no aneurysm, AVM • Hospital day 3: Right 3rd palsy recurred, now with altered mental status and lethargy CT Scan: Final Report • High density material within confines of Circle of Willis, concerning for possible SAH. • Left frontal subdural collection (subacute or chronic SDH) • Rule out empyema, meningitis, SAH. Brain MRI MRI: Final Report • • • • Bilateral SDH Evidence of SAH Diffuse meningeal enhancement Decreased caliber of right ICA and MCA, may be suggestive of vasospasm. Hospital Course (continued) • • • • Lumbar Puncture felt to be contraindicated Right ventriculostomy placed on HD#5 ICPs range: -6 to 4 CSF studies: – RBCs 485, WBCs 0, Glucose 59, Protein 8 – PMNs 84, Lymphocytes 10 • No improvement in neuro status. • Patient became progressively more obtunded and developed additional left 3rd nerve palsy,. MRI: Final Report • Interval placement of R frontal ventriculostomy • Left greater than right SDH Hospital Course (continued) • Discussion over intracranial hypertension versus hypotension began. • Patient started on trial of IV caffeine, supine position. • ICP Monitor (Bolt) placed to recheck ICPs • ICP range: -7 to 5 • That night, patient developed rapid progression of bradycardia to the 40s + apneic episodes • Emergent CT myelogram ordered Diagnosis • Spontaneous Intracranial Hypotension (SIH) secondary to Cervical and Thoracic CSF leak • CSF Leak at C1-C3 Left epidural space • Additional leak from T6-T10 ventrally • Patient started on IV caffeine drip • Placed in Trendelenburg position with increase in ICPs to 10-18 range and improvement in mental status Treatment • Anesthesia contacted for emergent epidural blood patch • Case done in IR suite under fluoroscopic guidance • C2 region received 8 cc autologous blood patch • T6-7 region received 21 cc blood patch • Immediate relief of headaches and increased ICPs to 15-19 (flat) Post-treatment Course • Post-patch day 1: Patient awake, alert x 2. Complete resolution of 3rd nerve palsies • Bolt removed • Sat up post-patch day 2 • Patient home day 7 following procedure, completely intact Spontaneous Intracranial Hypotension (SIH) • Patient Demographics: – Often occurs in middle-aged patients – Mean age ~40 years – Female preponderance – Higher incidences in patients with Marfan’s disease, other connective tissue diseases, and weightlifters Spontaneous Intracranial Hypotension (SIH) • Clinical findings: – Orthostatic headache • similar to post-lumbar puncture spinal HA – Exacerbated by laughing, coughing, Valsalva, physical exertion – Often refractory to analgesic agents – Nausea/vomiting, anorexia, neck pain/rigidity, dizziness, diplopia are common – Cranial nerve palsies (often VI) – Diverse presentation: Hearing changes, galactorrhea, facial numbness, radicular symptoms, parkinsonism, seizures, coma, death have been reported SIH: Diagnosis – Often misdiagnosed (94% in one series) – 14% misdiagnosed as SAH and underwent cerebral angiography – Diagnostic delay: 4 days to 13 years (mean 20 days) – CT Scan often misleading – Lumbar Puncture: • Opening pressures usually < 60 mm H20 in SIH • (normal 150-400 mm H20) – “Sucking noise” reported with LP on occasion, indicating subatmospheric pressure – CSF studies: • increased protein, lymphocytic pleocytosis,xanthochromia SIH: Radiographic Findings • CT Scan: – Effacement of basal cisterns – Subdural hygromas/hematomas – Pseudo-SAH: (10%) • Hyperdensity in basal cisterns (? obliteration of cisterns with arterial + venous engorgement) • MR Imaging: – Diffuse meningeal enhancement (pachymeninges, not leptomeninges) – Venous sinus engorgement – Pituitary gland enlargement/hyperemia – Downward displacement of brain/ tonsillar ectopia – Subdural fluid collections and hematomas, often without mass effect (50%) SIH: Radiographic Findings • CT Myelography – – – – – Study of choice for localizing leaks Lower cervical and thoracic region most common Often reveals CSF leaks and meningeal diverticula Better localization than spinal MR imaging Sensitivity: 67% in one study • Radionuclide Cisternography – – – – Radioactive tracer injected into lumbar subarachnoid space Normally, CSF travels upwards and is absorbed into sinuses Can detect CSF leaks Sensitivity: 60% for actual CSF leak, 90% for “abnormal study” • Doppler Flow Imaging • • • • Superior ophthalmic vein engorgement on TCDs Sensitive/specific in 26 of 26 patients (100%) Compared to healthy volunteers Improved with treatment SIH: Pathophysiology • Brain weighs approximately 1500g • Intracranial weight is ~ 48g because of suspension in CSF • Brain otherwise supported by meninges, veins, cranial nerves (esp. CNs V, IX, X) • Depletion of CSF in SIH causes downward pressure on these structures with traction on cranial nerves • Monro-Kellie Hypothesis: Decreased CSF leads to venous engorgement and cerebral edema/hyperemia. SIH: Treatment Options • Symptomatic relief (Conservative Management) – Often successful as first-line therapy – Supine position – Caffeine or theophylline (IV or PO) effective in ~75% of cases (vasoconstriction resulting in decreased CBF) – Fluid restoration: Increased IV/oral hydration, salt intake, CO2 inhalation • No proven efficacy for these therapies SIH: Treatment Options • Epidural Blood Patch – – – – – Technique developed by Gromley 85-90% efficacy for first trial Up to 98% efficacy with repeat patches Most effective if placed within 1 level of the leak If leak site undetectable, may place patch in lumbar spine and place in trendelenburg position (up to 9 level efficacy in models) – Immediate relief often observed (90%) • Initial relief: gelatinous seal over hole • Long-term: Collagen deposition, fibroblast activity, scar formation SIH: Treatment Options • Surgical repair of CSF leak: – For refractory cases – Especially for meningeal divertcula – Treatment with ligation of diverticula – Meningeal tears show less success with surgical repair – Fibrin Glue reported with success SIH: Long term Outcomes • Berroir S, Neurology, 2004: – 30 patients receiving early epidural blood patch – Follow-up time 1-4 years – 77% of patients cured with epidural blood patch • 57% after 1 patch • 20% after 2nd patch • Kong DS et al, Neurosurgery, 2005: – – – – 13 patients treated with nonsurgical measures Mean follow-up 51 months One recurrence (8%) Six patients with persistent HAs (4 mild, 2 moderate) References • 1. Paldino M et al. Intracranial hypotension Syndrome: a comprehensive review. Neurosurgical Focus 15 (6). 2003, 1-8. 1. • 2. Schievink WI et al. Pseudo-subarachnoid hemorrhage: A CT finding in SIH. Neurology 2005;65: 135-137 • 3. Schievink WI et al. Misdiagnosis of spontaneous intracranial hypotension. Arch Neurol. 60 (12). 2003. 1713-18. • 4. Inenaga C. Diagnostic and surgical strategies for intractable SIH. J Neurosurg. 94(4). 2001. 914-916. • 5. Schievink WI et al. SIH mimicking aneurysmal SAH. Neurosurgery. 48(3). 2001. 516-517. • 6. Rai A et al. Epidural Blood Patch at C2: Diagnosis and Treatment of SIH. AJNR. 26. 2005. 2663-2666. • 7. Berroir S et al. Early epidural blood patch in SIH. Neurology 63; 1950-1951, 2004. • 8. Kong, DS et al. Clinical features and long-term results of SIH. Neurosurgery. 57(1). 2005. 91-96. Thank You