Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
DIABETIC KETOACIDOSIS MANAGEMENT PROTOCOL
Table of Contents
I.
Introduction ………………………………………………………………………... 2
II.
Goals ………………………………………………………………………………. 3
III.
General Evaluation ………………………………………………………………... 4
Physical signs/Coma scale …………………………………………………
Assessment of dehydration ………………………………………………...
Assessment of acidosis …………………………………………………….
Initial laboratory studies …………………………………………………...
Serial laboratory monitoring ……………………………………………….
IV.
4
6
7
8
9
Treatment ………………………………………………………………………….. 10
Fluid therapy ………………………………………………………………. 10
Glucose ……………………………………………………………………. 12
Bicarbonate ………………………………………………………………... 13
Sodium …………………………………………………………………….. 15
Potassium ………………………………………………………………….. 15
Phosphorous ………………………………………………………………. 17
Calcium …………………………………………………………………… 18
Magnesium …………………………………………………………………18
Insulin ………………………………………………………………………19
Continuous low dose insulin infusion …….……………………………19
Intermittent subcutaneous insulin …..…………………………………. 22
Intramuscular insulin ………………………………………………….. 24
V.
Follow-up ………………………………………………………………………….. 25
VI.
Complications of DKA therapy …………………………………………………… 27
Cerebral edema ……………………………………………………………. 27
Other ………………………………………………………………………. 29
VII.
Nuts and Bolts …………………………………………………………………….. 30
VIII.
Bibliography ………………………………………………………………………. 34
1
DIABETIC KETOACIDOSIS MANAGEMENT PROTOCOL
“The key to successful management of DKA is….CAREFUL ATTENTION TO DETAIL!”
I.
INTRODUCTION/DEFINITION:
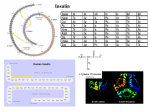
Diabetes Ketoacidosis is one of two serious, acute life-threatening complications of Type I,
insulin deficient diabetes mellitus (IDDM), or Type II, insulin insufficient diabetes mellitus,
the other being severe hypoglycemia. Diabetic ketoacidosis (DKA) may initiate the clinical
onset of Type I diabetes or may occur at any time during its subsequent course. About onequarter of persons with new onset IDDM will present in DKA. Rarely will patients with
Type II diabetes mellitus develop DKA.
Diabetic ketoacidosis is always caused by a relative or absolute insulin deficiency.
Biochemically, it is characterized by hyperglycemia of varying degree and:
Blood pH
Blood Glucose
HCO3
Ketonemia
< 7.30
> 250 mg/dl
< 15 mEq/L
> 1:2 dilution
Diabetic ketoacidosis in persons with established IDDM may occur as a consequence of the
person’s failure to administer the prescribed insulin or from environmental factors that
interfere with the action of insulin. Factors such as illnesses, infections and psychologic
stress result in the increased production and release of “stress” hormones such as
epinephrine, norepinephrine, cortisol, growth hormone and glucagon. These hormones not
only interfere with the peripheral action of insulin but also stimulate the release of hepatic
glucose (glycogenolysis) as well as the production of new glucose from endogenous
precursors (gluconeogenesis). Free fatty acids released by the increased rate of lipolysis
are metabolized in the liver into -hydroxybutyrate, acetoacetate and acetone (collectively
known as “ketones”). The resulting ketonemia raises plasma hydrogen ion concentration
(i.e. lowers pH) thus leading to the development of ketoacidosis. Simply speaking, in the
diabetic person already on insulin therapy, the stress-provoking environmental factors
cause a significant imbalance between the insulin effect and the counter-regulatory
hormones effects and results in a state of accelerated tissue catabolism that may progress to
DKA.
Ketonemia per se does not always result in metabolic acidosis. It does, however, indicate
that insufficient insulin is present and that the other metabolic changes associated with such
insufficiency (e.g. hyperglycemia) will result in increased fluid losses due to osmotic
diuresis. Under conditions of normal thirst sensation, the person will be able to keep up
with the increased fluid losses by drinking. When this compensatory response is interrupted
by nausea and vomiting, there can be a rapid progression to dehydration and metabolic
ketoacidosis. Correction of this metabolic decompensation state requires re-establishing
insulin balance and the proper replacement of fluid and electrolyte deficits.
2
Frequently, for any given episode of ketoacidosis the precipitating event remains unknown.
Although a careful screen for infection is appropriate, one should be aware that
leukocytosis, with counts as high as 30,000/mm³, is common with DKA as a result of the
associated leukemoid response to stress. The clinical picture can also, on occasion,
resemble appendicitis or an acute abdomen. However, abdominal pain, nausea and
vomiting are often the consequence of an acidosis-related increased prostaglandin (PGI2
and PGI3) production from adipose tissue. Failure to self-administer insulin is much more
common than generally appreciated and may be a manipulative event by the young patient
with diabetes, especially in the adolescent. It is worth noting that there is no evidence that
DKA will result SOLELY from dietary indiscretion. The amount of insulin required to
suppress lipolysis is approximately one order of magnitude (10 fold) less than the amount
required to adequately control plasma glucose levels.
Diabetic ketoacidosis is a serious complication and the mortality rate in pediatric hospitals
is STILL between 0.5 % and 2 %, mostly secondary to intra-cerebral crises. Patients
admitted with a diagnosis of DKA need to be monitored closely and aggressively until
clinically and biochemically stable and the acidosis and hyperglycemia are fully corrected.
The placement within the hospital of the child or adolescent with DKA is an important
management consideration. Careful and timely monitoring is mandatory and should be
done only by a trained professional observer at least every thirty minutes. If such
monitoring can be accomplished without undue burden on the staff, then admission to a
regular pediatric hospital floor is acceptable. If NOT, then the child with DKA MUST be
admitted to an intensive care setting that will facilitate the needed, close observation and
care.
II.
GOALS:
A.
Correct volume depletion
B.
Replace electrolyte losses
C.
Correct acidosis
D.
Abolish ketosis
E.
Treat precipitating factors:
1. infection
2. emotional stress
3. trauma
3
III.
GENERAL EVALUATION:
*
Admit patients with diabetic ketoacidosis only to a unit in which vital signs
and neurological status can be monitored frequently and glucose levels can
be measured hourly. All patients with a pH < 7.15 and/or any of the
following must be admitted ONLY to a pediatric Intensive Care Unit:
a.
b.
c.
d.
depressed or deteriorating mental status
blood glucose > 1000 mg/dl
age < 3 years
cardiovascular instability after 1st hour of fluid therapy
(i.e. required > 40 ml/kg IV bolus fluids)
e. respiratory insufficiency
*
Maintain constant cardiac monitoring until ketoacidosis resolves and patient
is clinically stable.
*
Keep precise and timely notes about the patient and his or her clinical
progress, including rationalization for therapeutic decisions.
*
Maintain a thorough flow sheet record of all laboratory and treatment
measures pertinent to the patient’s progress and therapeutic decisions.
A.
Physical Signs:
At presentation, assess ABCS for stability of patient’s status (A = airway;
B = breathing; C = circulation; S = sensorium/brain function)
1. Respiratory Status. If patient’s airway is compromised or if there are
signs of an impending compromise (i.e. respiratory fatigue, elevated
pCO2), use bag-valve-mask ventilation and consider intubation and
control of the airway.
2. Sensorium/Mental Status. Severe lethargy, drowsiness and somnolence are
common accompaniments of DKA and are due to the combined effects of
dehydration and acidosis. Semi-coma and coma may also occur and may
either be present at onset or develop during the course of treatment. A
thorough neurological evaluation must be performed on admission and at
regular intervals during treatment for DKA. Throughout the first 48 hours
the patient should be closely monitored for neurologic deterioration due to
cerebral edema.
4
a. To assess the level of consciousness in children 3 years of age, use the
Children’s Coma Scale:
Eye Opening
Spontaneous
Reaction to speech
Reaction to pain
No response
Best Motor Response
Spontaneous (obeys verbal commands)
Localizes pain
Withdraws to pain
Abnormal flexion response to pain
(decorticate posturing)
Abnormal extension response to pain
(decerebrate posturing)
No response to pain
Best Verbal Response
Smiles; oriented to sound; follows objects
and interacts appropriately
Crying
Interacts
consolable
inappropriate
inconsistently consolable
moaning
inconsolable
irritable; restless
no response
no response
Score
4
3
2
1
6
5
4
3
2
1
5
4
3
2
1
b. For children > 3 years of age:
Eye Opening
Spontaneous
Reaction to speech
Reaction to pain
No response
Best Motor Response
Spontaneous (obeys verbal commands)
Localizes pain
Withdraws to pain
Abnormal flexion response to pain
(decorticate posturing)
Abnormal extension response to pain
(decerebrate posturing)
No response
Score
5
4
3
1
6
5
4
3
2
1
5
Best Verbal Response
Oriented and converses
Disoriented but converses
Inappropriate words
Incomprehensible sounds
No response
Total Score Scale:
15
5
4
3
2
1
Normal, awake, conversive and oriented
12-13
Disoriented, localizes to pain, opens eyes to verbal
commands (<13 suggests the presence of cerebral edema)
8-10
opens eyes only to painful stimuli, shows flexor or extensor
response to pain (non-localized)
(<8 is considered a medical emergency)
3
Brain dead
3. Dehydration/Vascular Volume. Determine patient’s clinical hydration
status by examining vital signs (heart rate, blood pressure, pulse
pressure), the quality of the peripheral pulse quality and capillary refill
time. Weigh patient carefully. Fluid administration may be the most
important early treatment intervention.
4. Acidosis. Check for fruity-smelling breath and increased depth as ell as
rate of breathing. Classic “Kussmaul” respirations occur when the pH is
7.25. Shallow breathing may indicate a more severe degree of acidosis.
5. Infection. Screen for a source of infection. Severe leukocytosis may
occur with DKA and NOT be indicative of an underlying infection.
6. Monitoring. Monitor vital signs, including assessment of mental status
and overall state of hydration, at least hourly via a competent, professional
observer. Record intake and output accurately. Weigh patient every
24 hours.
B.
Assessment of Dehydration:
Severe
Moderate
Mild
% Dehydration
10-15%
5-10%
< 5%
The degree of dehydration observed in DKA is variable and, on occasion,
may be profound. The magnitude of the water deficit may be deceiving and
6
the extent of dehydration underestimated due to the fact that in DKA there is
a disproportionate loss of water from the intracellular fluid compartment
(ICF) in distinction to the extracellular fluid space (ECF). In fact, it is
unusual to see a patient in DKA who is initially shocky (hypotension,
decreased peripheral perfusion, pallor, mottling, delayed capillary refill)
since the high level of glucose in the extracellular fluid space usually protects
against this. Shock, if it occurs, does so late in the untreated course or in
response to the rapid movement of blood glucose into the intracellular
compartment. The presence of shock is an ominous sign and should be
treated vigorously and aggressively with isotonic fluid administration.
The person with acute DKA often has good color and may even appear
flushed from the vasodilatory effects of increased circulating levels of
prostaglandins. This situation is in marked contrast to the more common
types of dehydration secondary to vomiting and diarrhea seen in pediatrics
where the loss of fluid is predominantly from the extracellular compartment.
Sine most physicians use various clinical signs of dehydration that reflect
extracellular fluid deficits, it is not surprising that the degree of dehydration
in DKA, the classic example of intracellular dehydration, is often
underestimated.
The degree of dehydration may be estimated by considering the solute:water
ratio of the extracellular fluid (i.e. osmolality). This may be either measured
or estimated from the following formula:
Serum osmolality = [2 x (sodium concentration)] + blood glucose (mg/dl) + BUN
18
2.8
C. Assessment of Acidosis:
PH
Severe
< 7.10
Moderate 7.10-7.30
Mild
> 7.30
HCO3
< 5 mEq/L
5-10 mEq/L
> 10 mEq/L
The metabolic acidosis in DKA is primarily related to the elaboration of
hydrogen ions as a consequence of fatty acid breakdown from the exaggerated
catabolic rate. The concomitant dehydration produces a decrease in renal
perfusion limiting the body’s normal attempts at elimination of non-volatile,
organic and ketoacids.
At presentation, arterial pH in DKA is commonly in the range of 7.00 to 7.10
with serum bicarbonate concentrations below 10 mM/L. Insulin is required to
reverse the fatty acid breakdown and appropriate fluid replacement is essential
to reestablish kidney’s normal excretory function. Without the latter, the
kidney cannot excrete the acid end products of lipid and protein metabolism.
7
Excess acetone, however, is still excreted through the lungs and gives many
patients a characteristic fruity odor to their breath.
D.
Initial Laboratory Studies:
1. Blood Glucose. Bedside capillary blood sugar testing results should be
confirmed intermittently with serum samples run by the laboratory to
ensure technical competence by the nursing/medical staff doing the
bedside monitoring. Caution: Initial blood glucose levels may exceed the
limits of most capillary blood glucose monitors.
2. Venous or Arterial pH and pCO2. Unless there is concern with the
patient’s ventilatory status, initial arterial or arterialized venous blood
samples may be used to assess pH. Subsequent determinations may be
done from non-tourniquet venous blood since only the pO2 will be
markedly affected. At presentation, plasma pH values in the range of 7.00
to 7.10 are common with HCO3 concentrations below 10 mM/L.
3. Serum Acetone/-hydroxybutyrate
4. Na/K/Cl/CO2. The initial sodium concentration is usually low due to the
movement of free water into the extracellular fluid compartment and the
loss of sodium in the urine as well as from vomiting. Potassium is usually
high-normal to high. CO2 is characteristically low.
5. BUN/Creatinine. BUN in DKA is initially a better measure of renal
function than creatinine since the presence of ketonemia, specifically
acetoacetate, may interfere with the laboratory measurement of serum
creatinine levels. Caution: Although an elevated BUN in DKA most
frequently reflects a decrease in extracellular fluid volume and a decrease
in glomerular filtration rate (GFR), the BUN may alternatively be
increased secondary to excess protein breakdown.
6. Calculated Serum Osmolality
Note: serum osmolality = 2(Na) + BUN (mg/dl) + Glucose (mg/dl)
2.8
18
[Normal: 275-295]
7. Anion Gap
Note: anion gap = Na (Cl + HCO 3)
[Normal: 8-16 mEq/L]
8
8. Calcium/Phosphorus/Magnesium. If readily available, ionized calcium
results are preferred while the patient is acidotic because of the known
effect of acid-base imbalance on calcium binding (i.e. calcium binding
increases thereby decreasing the ionized calcium concentration, as pH
increases).
9. Complete Blood Count with differential. Leukocytosis is common in
DKA but does not necessarily imply the presence of an underlying
infection. The elevated white blood cell count may be secondary to a
stress response. Alternatively, fever may be absent in patients whose
DKA is triggered by infection.
10. If patient is a new onset IDDM, obtain the following lab before the
administration of any insulin:
a.
b.
c.
d.
e.
E.
insulin (2 cc’s blood in a red top or “tiger” tube)
C-peptide (2 cc’s blood in a red top or “tiger” tube)
Islet cell antibodies (1 cc blood in a red top or “tiger” tube)
Anti-GAD antibodies (2 cc’s blood in a red top or “tiger” tube)
Hemoglobin A1C (3 cc’s blood in a purple top tube)
Serial Laboratory Monitoring:
1. Glucose. Obtain hourly glucose determinations for as long as insulin is
being given. These should be done at the bedside with intermittent
confirmation (i.e. every 4 hours) of the accuracy of results by the hospital
laboratory on concurrently obtained serum samples.
2. Electrolytes. Sodium, potassium, chloride and CO2 should be monitored
every two hours during the initial phase of DKA therapy. Subsequent
frequency of testing will depend on the patient’s clinical progress and state
of recovery. Calculate osmolality and anion gap concurrently with each
set of electrolyte results.
3. Venous pH and pCO2. Venous blood gases should be checked every two
hours until pH 7.25. Subsequent monitoring of acid-base status can be
effectively achieved via serum HCO3 levels found in most electrolyte
panels.
4. Ketones. Urine ketones may be checked once every 8 to 12 hours until
clear. Serum ketone determination should be done initially to confirm a
diagnosis of ketoacidosis. Subsequently, serum ketones should be checked
only when serum CO2 is > 20 to document the complete eradication of
ketosis. Repetitive measurements of serum ketones (acetate and
acetoacetate) are NOT helpful for monitoring the patient’s therapeutic
progress unless -hydroxybutyrate results can be rapidly measured. Under
9
normal circumstances, -hydroxybutyrate is converted to acetate and
acetoacetate. As a result, ketosis may seem to paradoxically worsen as the
patient gets clinically better because of increased conversion when vascular
circulation is reestablished and tissue oxygenation is restored. In the
absence of readily available -hydroxybutyrate results, the KEY parameters
to follow are the serum pH, the calculated anion gap and the total HCO3
since these give a more accurate assessment of therapeutic progress.
5. BUN and Creatinine levels should be monitored every 8 to 12 hours.
6. Ca/Phos/Mg should be checked every 8 to 12 hours as indicated by prior
results. If the patient is hypophosphatemic or hypocalcemic, calcium and
phosphorous levels will need to be monitored more frequently.
7. EKGs should be performed only if hypo- or hyperkalemia is clinically
indicated.
F.
IV.
DKA Flow Sheet (see appendix)
TREATMENT:
A.
Fluid Therapy. The following guidelines for management of the DKA patient
must be individualized to fit the clinical picture. Adequate support staff care
is the sine quo non of successful DKA treatment. This requires the constant
presence of a competent professional observer, especially in the early hours of
therapy.
1. Successful management of DKA is dependent upon the proper selection
and administration of sufficient intravenous fluids as determined by close,
serial monitoring of:
a. the patient’s clinical response (sensorium, blood pressure, pulse
pressure, heart rate, respiratory rate, capillary filling time)
b. plasma glucose, pH and electrolytes including CO2
c. strict recording of intake and output and serial body weight
measurements on admission and every 24 hours. Unless the patient’s
sensorium is significantly depressed, avoid bladder catheterization as
the risk of secondary infection substantially outweighs the potential
benefits.
Restoration of vascular perfusion will increase glucose utilization in
peripheral tissues, increase urinary glucose and ketone excretion and
reverse the progression of acidosis.
10
2. Intravenous fluids can be calculated on the basis of existing fluid deficits,
clinical evidence of hypovolemia or shock, ongoing fluid losses and
expected maintenance requirements. Ongoing losses may be marked and
are due to the osmotic diuresis and the increased fluid demands of
persistent tachypnea and hyperventilation.
a. initial loading dose of normal saline at 10-20 ml/kg body weight
over 20-30 minutes. Additional boluses may be administered based
on patient’s clinical hydration status such as blood pressure, pulse
pressure, rate and quality of peripheral pulses and capillary filling
time.
b. following initial fluid resuscitation, give the rest of the total calculated
fluid requirements/replacement over the subsequent 48 hours.
*
Maintenance fluids:
1500 ml/m²/24 hrs.
OR
0 - 10 kg. = 100 ml/kg/24hrs.
10 - 20 kg. = 1000 ml + [(weight in kg. 10) x 50]
> 20 kg. = 1500 ml + [(weight in kg. 20) x 20]
*
Deficit fluids:
Percent Dehydration
5%
10 %
15 %
Deficit
50 ml/kg
100 ml/kg
150 ml/kg
c. Calculate total fluids required for rehydration over 48 hours. Rate
of fluid administration should be kept at < 4000 ml/m²/day or less than
250 % of maintenance unless patient’s clinical status dictates otherwise.
A few studies have suggested that limiting total fluid administration to
4000 ml/m²/day may lessen the risk of developing cerebral edema.
*
calculate the required IV fluid rate for the first 24 hours of
rehydration as follows:
Rate/hr = Daily Maintenance Fluids + ½(Calculated Fluid Deficit)
24 hours
24 hours
11
*
calculate the required IV fluid rate for the second 24 hours of
rehydration as follows:
Rate/hr = Daily Maintenance Fluids + ½(Calculated Fluid Deficit)
24 hours
24 hours
When administering calculated fluid requirements, it is imperative that the patient’s
clinical hydration status and intake/output be frequently assessed. Changes in the rate of
fluid administration must be urgently instituted to compensate for persistent,
symptomatic fluid deficits (tachycardia, hypotension, decreased pulse pressure) or
iatrogenic fluid overload (eyelid, extremity or lumbar edema, pulmonary rales).
3. Crystalloid Solutions
a. give the initial fluid bolus(es) as isotonic (0.9 %) Normal Saline or
Lactated Ringer’s
b. limit volume to 1 liter per bolus
c. continue calculated fluid replacement (deficit plus maintenance) as 0.9
% Normal Saline until Dextrose added to IV solution. Then change to
D5 ½ (0.45 %) Normal Saline with potassium supplement as indicated
by lab/clinical findings.
d. If glucose falls 250 mg/dl while on D 5 ½ (0.45 %) Normal Saline as a
result of insulin administration and the resolution of the acidosis, change
IV to D10 ½ (0.45 %) Normal Saline with potassium supplement to
maintain desired glucose:insulin ratio.
e. A hypernatremic state at DKA presentation suggests the need for even
slower and more careful correction of the patient’s fluid deficit.
B.
Glucose
The blood glucose at the time of DKA presentation is quite variable and may
range from the low 200’s to well over 1000 mg/dl. The degree of acidosis bears
little relationship to the degree of hyperglycemia. DKA may occur with a
serum glucose as low as 300 mg/dl if the patient is having problems with
recurrent emesis OR as a result of a decreased carbohydrate intake in the face of
additional doses of subcutaneous insulin given at home. However, although the
height of the blood glucose is NOT a good index of the severity of the patient’s
illness, extremely high serum glucose concentrations tend to be often associated
with a more severe degree of dehydration and, thereby, with an increased
morbidity and mortality.
12
C.
*
No dextrose infusion if initial blood glucose is > 500 mg/dl
*
Add 5 % dextrose to the intravenous fluids when blood glucose is
400 mg/dl or decreasing at 100 mg/dl/hour. Caution: The rate of
decrease of serum glucose is sometimes greater in the first hour of
rehydration as the intravascular volume expands and GFR (glucosuria)
increases.
*
Administered glucose to insulin ratio (grams of glucose per hour : units of
insulin per hour) should be between 4:1 and 6:1. Increase glucose to insulin
ratio when blood glucose is 200 mg/dl to maintain serum glucose in the
200-250 mg/dl range.
*
Avoid blood glucose levels 150 mg/dl. Signs and symptoms of
hypoglycemia include somnolence, headache, confusion, fatigue, seizures,
loss of consciousness, anxiety, tremors and diaphoresis. Maintain serum
glucose in the 200 - 250 mg/dl range until plasma ketones are cleared and
ketoacidosis resolves
*
Plasma glucose invariably falls more rapidly than plasma ketones and
correction of the acidosis. Insulin should not be stopped because plasma
glucose concentrations approach the normal range; rather glucose infusion
rates should be increased and insulin infusion continued until the ketosis has
cleared. Maintain serum glucose in the 200 – 250 mg/dl range.
Bicarbonate
Indicated only when initial pH 7.10, pCO2 < 40 torr and repeat pH fails to
improve after initial fluid bolus(es) resuscitation (repeat pH still 7.10 one hour
after initial results). Give ½ mEq HCO3 per kilogram of body weight
intravenously over 1-2 hours. Intravenous bolus bicarbonate is very rarely, if
ever, indicated except under a full cardiorespiratory arrest situation.
*
The fluid rate of the bicarbonate infusion should be determined by the
patient’s calculated fluid requirements
*
Give bicarbonate continuously either via separate venous access or
piggybacked into the main IV line. Do NOT administer the bicarbonate in
the same intravenous line containing calcium. Do not mix the bicarbonate
directly into the insulin infusion IV bag.
*
Do NOT give bicarbonate if the patient is hypokalemic.
13
*
Overcorrection, or too rapid correction, of pH with bicarbonate may result
in:
a. hypokalemia. Bicarbonate causes a shift of the serum
potassium into the intracellular fluid compartment.
b. paradoxical CSF acidosis. Bicarbonate results in the
production of CO2. The produced CO2 crosses the blood-brain
barrier more readily than bicarbonate and can cause a
paradoxical lowering of CSF pH.
c. impaired oxygen-hemoglobin dissociation. Bicarbonate
shifts the oxygen-hemoglobin dissociation curve to the left
leading to an impaired oxygen release to the tissues and an
increased production of lactate.
d. deterioration of mental status
e. increased tonicity. The administration of bicarbonate
concurrently infuses the patient with a high sodium load and
may result in a hyperosmolar serum.
f. alkalosis. Alkalosis may result either from too much
bicarbonate administration (overshoot alkalosis) or can occur
as ketoacids and lactate are metabolized to bicarbonate
during insulin therapy (rebound alkalosis).
Administration of bolus bicarbonate therapy has been related to worsening
of the mental status/sensorium. Do NOT give bicarbonate if unable to
adequately ventilate the patient since the administered bicarbonate can cause
an increase in pCO2 and an acutely rapid decrease in serum pH.
*
Correction of acidosis. Often during the improving phase of DKA
treatment, the pH rises and the anion gap narrows even though the plasma
bicarbonate (HCO3) remains low. The persistently low bicarbonate is most
likely a consequence of the hyperchloremia that develops during DKA
treatment as a result of the rapid or excess infusion of sodium (NaCl) or
potassium chloride (KCl) and the loss of bicarbonate from the blood either
via the urine as ketones or through its exchange with intracellular buffers.
However, if the anion gap remains elevated and the pH remains persistently
low by 4 to 6 hours after treatment was initiated, this indicates insulin
resistance or a persistent insulin insufficiency and requires aggressive
increases in the amounts of administered insulin and fluids.
Alternatively, some patients may demonstrate a persistent anion gap despite
clinical improvement and a rising pH. In this situation, the unmeasured
14
anion is presumably derived from tissue buffers and the anion gap
persistence does NOT indicate insulin resistance or insufficiency especially
if present in the face of clinical improvement and a rising pH.
D.
Sodium
The serum sodium (Na) concentration at onset is variable but total body sodium
is almost always depressed by 10 mEq per kilogram of body weight. Serum
Na may be as low as 120 mEq/L yet, this does NOT generally require specific
management since the hyponatremia is predominantly dilutional. Such falsely
depressed serum sodium concentrations are caused by the solute Na being
diluted by free water drawn from the intracellular fluid compartment as a result
of an elevated serum glucose concentration. The corrected serum sodium can
be calculated as follows:
Corrected Sodium = (Na in mEq/L) + {([Glucose in mg/dl] – 100) x 1.6}
100
A quick method for calculating the corrected sodium is to add 1.6 mEq/L for
every 100 mg/dl of serum glucose above 100 mg/dl. Put another way, for each
100 mg/dl increase in serum glucose above 100 mg/dl, the serum Na decreases
by 1.6 mEq/L.
Note: Hyponatremia usually self-corrects as the blood glucose falls as a result
of fluid replacement and insulin therapy. High or high-normal serum sodium
levels at DKA presentation are worrisome and have been associated with the
development of cerebral edema. A hypernatremic state suggests the need for
even slower and more careful correction of the fluid deficit.
Note: In some laboratories, factitious hyponatremia may also be caused by
hyperlipidemia.
E.
Potassium
Serum potassium (K) will often be initially elevated due to the acidosis. Much
of the increase in the extracellular hydrogen ion concentration is buffered
within the cells by the intracellular proteins, phosphates and amino acids. To
maintain the electrical neutrality of the cell, the major intracellular cation, K,
moves out from the intracellular into the extracellular fluid compartment. As
such, the usual and expected finding at DKA presentation is an elevated serum
potassium concentration, the degree of elevation being principally dependent
on the degree of acidosis. Plasma concentrations of potassium in the range of
5-7 mEq/L are therefore expected and require no specific treatment if renal
function is normal and the EKG is unremarkable.
15
Despite the actual serum potassium concentration, the patient in DKA is
usually total body potassium depleted upon initial presentation. Hypokalemia
is thereby often a management problem if not anticipated and treated
accordingly.
Serum potassium levels will decrease with each of the following:
a. administration of both glucose and insulin
b. correction of acidosis
c. rehydration which promotes an increased renal function with an
increased renal potassium excretion
If, in the presence of severe acidosis (i.e. pH 7.20), the child presents with a
low, or even low-normal potassium, prompt treatment must be immediately
instituted to prevent severe hypokalemia from developing later. When initial K
is 3.0 mEq/L, potassium should be given in the initial expansion fluids
without waiting for demonstration of renal function and insulin therapy should
be held until the initial treatment fluids have been infused. It is crucial to know
the patient’s initial serum potassium status either by blood sample or EKG Twave changes.
If there is EKG or clinical evidence of hypokalemia and the serum potassium
concentration is NOT known, provide KCl as an infusion of 0.5 mEq. per
kilogram of body weight over one hour (maximum dose: 10 mEq. per hour;
maximum potassium concentration: 1 mEq. per 5 cc’s). Avoid rapid infusions
of potassium since these can result in cardiac dysrthymias.
*
Supplemental potassium is NOT given until the patient’s functional renal
status is known. If functional renal status is a concern, wait until urine
output is adequate and the serum K (potassium) is NOT elevated (i.e. < 5.5
mEq/L). If the initial serum potassium is 5.5 mEq/L, follow serum
potassium concentrations hourly until the level is 5.0 mEq/L.
*
Do NOT add potassium to the IV fluids if any of the following conditions
are present:
a. oliguria or anuria
b. acute renal failure
c. cardiac arrest
*
Once serum K 5.0 mEq/L and renal status acceptable (BUN/Creat. Ratio
< 20), give 20–40 mEq/L of potassium intravenously. The lesser
concentration should be used initially in the treatment regimen when the
fluid rate is highest. Alternatively, in the face of hypokalemia,
concentrations of IV potassium considerably in excess of the above range
may be therapeutically necessary.
16
*
Guidelines for potassium replacement.
Serum Potassium (mEq/L)
Fluid Composition
< 3.0 without EKG changes
30 mEq/L KCl plus
30 mEq/L KPO4
3.0 – 5.5
20 mEq/L KCl plus
20 mEq/L KPO4
> 5.5
Hold potassium
*
Give potassium as a mixture of ½ potassium phosphate (K2PO 4) and ½
potassium chloride (KCl). If patient is hypophosphatemic (i.e. serum
phosphorous < 1.5 mg/dl) give all of the potassium replacement as K2PO4.
Caution: if patient is hypocalcemic, consider giving the potassium
replacement as ½ potassium citrate or acetate in place of the phosphate or
all as KCl.
*
Monitor the patient’s lead II EKG continuously for electrical evidence of
hypo- or hyperkalemia.
Serum K (mEq/L)
< 2.5
F.
EKG Changes
Depressed ST segment
Diphasic T wave
Prominent U wave
> 6.0
Peaked T wave
> 7.5
Prolonged PR Interval
Wide QRS complex
Peaked T wave
> 9.0
Absent P wave
Sinusoidal wave
Ventricular Fibrillation
Asystole
Phosphorous
Despite the initial serum phosphorous level, a patient in DKA is usually total
body phosphorous depleted at presentation. Further, insulin therapy will drive
phosphorous intracellularly, thereby decreasing its serum (extracellular fluid
compartment) concentration.
17
Severe hypophosphatemia (< 1.0 mg/dl) can cause congestive heart failure,
respiratory failure, hemolysis, decreased 2,3-DPG concentrations leading to
tissue hypoxia from a leftward shift of the oxygen-hemoglobin dissociation
curve, thrombocytopenia, rhabdomyolysis, muscle weakness, CNS depression,
irritability and paresthesias. Moderate hypophosphatemia (< 1.5 mg/dl) can
cause weakness, malaise, anorexia, nausea and vomiting.
Administer phosphorous as K2 PO4. If serum phosphorous level is < 1.5 mg/dl,
then give all of IV potassium replacement as K2PO 4. Unless hyperphosphatemia
or hypocalcemia develops, maintain fluid potassium replacement as K2PO 4.
Adverse effects associated with phosphorous administration include
hypocalcemia, metastatic calcifications and hypotension. During treatment for
DKA, patients must be monitored for hypocalcemia as a complication of
phosphorous replacement/administration. Do NOT give phosphorous if there is
clinical evidence of hypocalcemia or if serum phosphorous is < 8.0 mEq/L.
G.
Calcium
Hypocalcemia can result in muscle twitching, muscle spasms (including
laryngospasm), seizures, Chvostek’s sign (spasm of the facial muscles elicited
by tapping the facial nerve in the region overlying the parotid gland) and
Troussea’s sign (wrist flexion with fingers drawn together when blood pressure
cuff is used to occlude brachial artery).
If patient is hypocalcemic at presentation or develops same as a complication of
phosphorous treatment for DKA (Calcium 7.5), change IV KPO 4 to KCL.
Give 100 mg of Calcium Gluconate per kilogram of body weight IV over
30-60 minutes. Monitor patient’s heart rate and rhythm during calcium
administration for evidence of bradycardia or heart block.
H.
Magnesium
The presence of hypomagnesemia can lead to tremors, tetany, seizures, apathy,
delirium, coma and various cardiovascular effects including congestive heart
failure, hypotension, ventricular dysrhythmias and EKG changes of a prolonged
PR, QT and QRS intervals and t wave inversion.
If initial, or subsequent, magnesium concentration is 1.6 mg/dl (normal range:
1.8 - 2.9), supplement with MgSO4 at 25-50 mg/kg/dose given IV every 4 to 6
hours. Magnesium supplementation may also be given by mouth as tolerated at
100-200 mg/kg/day divided q.i.d. (1 gram = 8 mEq.) Monitor patient closely
for hypocalcemia, hypotension, loss of deep tendon reflexes, prolonged cardiac
conduction time and respiratory paralysis.
18
I.
Insulin Administration
Regular or Humalog human insulins are the ONLY insulin types that should be
administered in the acute treatment of DKA. Except in situations where the
peripheral circulation is compromised, insulin is almost as effective given IM or
SQ as it is IV. Insulin is used to turn off ketone production through its
inhibitory effects on lipolysis and proteolysis. Insulin will also stimulate
glucose uptake and utilization into peripheral tissues. If the patient presenting
with DKA is an established diabetic, note the usual home insulin dosages and
whether they were given. If SQ insulin was administered at home a few hours
prior to admission for DKA, it may not have been fully absorbed due to the
associated dehydration. Knowledge and anticipation of this factual history may
help avoid subsequent hypoglycemia from the delayed absorption of the home
administered insulin as the patient’s vascular fluid status is restored.
1. Continuous Low Dose Intravenous Insulin Infusion:
Initiate insulin infusion therapy only when intensive medical/nursing
supervision of the patient’s clinical status is available and the rapid
determination of serial glucose levels is possible.
a. Rationale:
*
maintains a steady state plasma insulin level thereby, avoiding
marked variations in acid-base balance and serum glucose levels
*
allows for easy, rapid regulation of the administered insulin dose
*
requires less total insulin to correct the ketoacidosis
*
may reduce the time necessary to clear serum ketones and correct
ketoacidosis
*
effectively inhibits ketosis and hepatic glucose production
*
the short half-life of intravenous insulin (approximately 5 minutes)
allows for better, more accurate “minute to minute” control of
therapy as well as a more rapid treatment response time to changes
in insulin dosage
b. Dose:
1. Administer initial IV bolus of 0.025-0.1 units per kilogram of body
weight of fast-acting insulin (Regular or Humalog) to saturate the
insulin receptors. The bolus dose is based on the level of initial
19
hyperglycemia and acidosis. This bolus may be omitted if the
patient’s initial blood pH is > 7.15 OR initial serum glucose is
400 mg/dl.
2. Start continuous infusion of 0.1units/kg/hour of fast-acting insulin
(Regular or Humalog). The desired concentration of insulin is
calculated and mixed in either ½ (0.45%) normal saline or 0.9%
normal saline. The infusion rate per hour is varied to administer the
needed insulin treatment regimen. The insulin infusion rate,
however, should be maintained between 0.05 and 0.1 units per
kilogram of body weight per hour unless there is evidence of
intrinsic insulin resistance (i.e. Type II diabetes mellitus, obesity,
therapeutic hypercortisolism or the presence of an underlying
bacterial infection) OR the initial hyperglycemia fails to decrease by
at least 50 mg/dl/hour.
The standard recommended insulin concentration/dilution for continuous
intravenous infusion is:
1.00 U/ml
Mix 100 units R/H in 100 mls. NS
For young children requiring lower insulin infusion dosages use:
Insulin Concentration
0.10 U/ml
0.20 U/ml
0.50 U/ml
Dilution
Mix 25 units R/H in 250 mls. NS
Mix 50 units R/H in 250 mls. NS
Mix 125 units R/H in 250 mls. NS
3. Maintain administered glucose:insulin ratio at 4-6:1 (grams of
intravenous glucose per hour: units of intravenous insulin per hour).
The hourly fall in serum glucose concentration should NOT exceed
100 mg/dl/hr. As the patient becomes adequately hydrated and less
acidotic, insulin resistance decreases (i.e. insulin sensitivity) and its
glycemic effect improves. If the blood glucose falls to
250 mg/dl or less, increase the glucose concentration, rather than
decreasing the insulin infusion, to maintain the above ratio. Avoid
decreasing the rate of the insulin infusion since this will likely delay
the clearance of serum ketones and the correction of the
ketoacidosis. Aim to maintain the serum glucose in the 200 - 250
mg/dl range until plasma ketones are cleared and the ketoacidosis
resolves.
Note: If the serum glucose is < 200 mg/dl, increase the glucose
concentration of the IV fluids. Temporarily hold the insulin infusion
and monitor the blood sugar every 30 minutes until it rises above
200 mg/dl. Once the blood sugar is 200 mg/dl, resume the insulin
infusion BUT at a higher hourly glucose to insulin ratio.
20
Note: Never give intravenous insulin by multiple intermittent
injections to treat DKA.
Note: Insulin mixed in saline is stable for approximately 24 hours.
Note: Flush the initial 25 mls. of each mixture to coat the IV tubing
and the Soluset/Buratrol.
Note: Continuous intravenous insulin can be piggy-backed into an
existing IV BUT should always be given with an IVAC or a similar
pump device to ensure its precise administration. When piggybacked, the insulin tubing should be inserted as close to the venous
access site as possible without an inline filter. Using only one
extremity for both the necessary fluid replacement and the
continuous insulin infusion allows for serial laboratory blood
samples to be drawn from the contralateral extremity via a patientfriendly heparin “lock”.
Note: Do NOT administer bicarbonate or calcium in the same
intravenous line as the insulin infusion.
4. When the blood glucose is 400 mg/dl, add dextrose to the main
intravenous, fluid replacement line.
5. If unable to maintain the serum glucose in the 200 - 250 mg/dl range
using D10 ½ (0.45 %) Normal Saline, then the insulin infusion can
be decreased. The insulin infusion, however, should NOT be
decreased below 0.05 units/kg/hour if at all possible as low rates of
insulin infusion will result in a slower resolution of the ketoacidosis.
6. The insulin drip can generally be discontinued when the patient’s
blood pH is 7.30 AND the serum bicarbonate is 20 mEq/L. The
endpoint of therapy for DKA is the correction of the acidosis and
NOT the achievement of euglycemia. Thereafter, proceed with
insulin therapy using the traditional subcutaneous method.
Note: It is imperative that subcutaneous fast-acting insulin be
administered immediately upon (Humalog), or 20-30 minutes prior
to (Regular), discontinuation of the intravenous insulin infusion.
Otherwise, because of the very short half-life of intravenous insulin,
insulin deficiency will quickly develop and could lead to the reappearance of ketoacidosis.
21
2. Intermittent Subcutaneous Insulin:
Subcutaneous insulin should be administered to a DKA patient ONLY if
vascular volume is adequate since subcutaneous insulin absorption in a
dehydrated patient is unpredictable. Do NOT give insulin SQ or IM if
patient is in shock.
a. Fast acting (Regular or Humalog) U-100 insulin
Severity of DKA
Moderate/Severe
Mild/Moderate
Mild
Insulin Dose
1.0 units/kg SQ
0.5-1.0 units/kg SQ
0.25 units/kg SQ
b. Initially can give ½ the calculated dose as an intravenous bolus if
hyperglycemia is > 750 mg/dl.
c. An additional bolus of subcutaneous insulin may be given in 1-2 hours
if the patient’s blood sugar fails to respond to the initial bolus.
Note: check patient’s vascular volume/hydration status prior to any
additional bolus to ensure adequate subcutaneous absorption of insulin.
If dehydration persists, give additional fluids (see section IV.A.2.a
above) and consider administering insulin intravenously as a continuous
infusion (see section IV.E.2 below).
d. Subsequent doses of fast acting insulin (U-100) are usually given
q 3 to 4 hours after the initial bolus(es) at doses of 0.25-1.0 units per
kilogram of body weight subcutaneously.
Note: subsequent doses of subcutaneous insulin will need to be adjusted
on the basis of follow-up lab studies and the clinical response of the
individual patient
e. Once oral intake is tolerated, subcutaneous injections of fast-acting
insulin (Regular or Humalog) are given prior to each main meal and at
bedtime at a dose of 0.1-0.2 units per kilogram of body weight. If the
patient is stable, an intermediate (NPH) or long-acting insulin (UltraLente) may be substituted for the bedtime dose of fast-acting insulin.
22
f. With continued improvement, combinations of rapid (Regular or
Humalog) and intermediate/long acting insulins in multiple doses may
be given as follows:
Total Daily Dose: 0.6-1.2 units per kilogram of body weight per day
divided as follows:
Time
Pre-breakfast
Total Daily Dose
2/3 - 3/4
Pre-dinner
1/6 - 1/8
Insulin
NPH:Regular or Humalog
(2:1 ratio)
Regular or Humalog
Pre-bedtime snack
1/6 - 1/8
NPH or Ultra-Lente
Note: If the patient is to receive only a b.i.d. insulin injection regimen at
home, the bedtime intermediate or long-acting insulin may be combined
with the pre-dinner fast-acting insulin and administered together as a
single injection.
Note: Subcutaneous Regular insulin must be administered 20 to 30
minutes before the scheduled meal for maximal effectiveness.
Alternatively, Humalog need only be given 5 to 10 minutes before the
scheduled meal.
The bedtime intermediate or long-acting insulin may be given
immediately prior to the bedtime snack without affecting its efficacy.
However, if the bedtime snack exceeds 35 grams of carbohydrates, a
small dose of short-acting insulin (Regular or Humalog) may be
necessary to avoid significant post-prandial hyperglycemia.
Note: Regular insulin may be combined with NPH but NOT with UltraLente as the latter combination may significantly delay the Regular
insulin’s absorption characteristics and result in post-prandial
hyperglycemia and a delayed hypoglycemia. In contrast, the rate of
subcutaneous absorption of Humalog has been shown to remain
unaffected when combined with Ultra-Lente and may thus, be
administered in combination without causing adverse effects on the
patient’s diabetes control. As of this writing, January 1999, data is
limited as to the effects of combining Humalog and NPH on the
former’s absorption characteristics. The consensus, however, is that the
combination of Humalog and NPH may adversely delay the glucose
lowering effects of Humalog and should, therefore, be given in the same
syringe with NPH only with caution and close monitoring of its
glycemic effect.
23
3. Intramuscular Insulin
a. Dosages are generally similar to those used with an intermittent
subcutaneous insulin regimen.
b. Because of the shorter half-life of intramuscularly administered insulin,
it is given on an hourly schedule.
24
V.
FOLLOW-UP:
A.
Sugar-free oral fluids
*
B.
can usually be given 6 to 12 hours after the start of therapy depending on
the patient’s level of consciousness, lack of nausea and success of treatment
(i.e. correction of acidosis and dehydration).
Diet
Initially, patient should be placed n.p.o. especially if nausea or vomiting is
present or if mental status/sensorium is depressed.
*
as the patient continues to improve, advance diet from clear liquids to a
Constant Carbohydrate Diet regimen with three main meals plus snacks.
*
snacks should be included as follows:
preschool age
school age
3 snacks per day (a.m., p.m. and h.s.)
2 snacks per day (p.m. and h.s.)
Note: Although not offered right away, the patient’s special diet may need
to be offered 12 or more hours in advance to allow its preparation by the
hospital’s kitchen staff.
C.
Calories
*
caloric requirement may be estimated as follows:
1000 kcal/day + [(100 x Age in years)] = Total daily calories
*
distribution of calories should be as follows:
CHO
Protein
Fat
D.
55 %
15 %
30 %
Insulin
1. If patient is an established, previously diagnosed diabetic child or
adolescent, simply resume his/her outpatient insulin regimen and monitor
its glycemic effect via frequent capillary blood sugars prior to discharge.
Supplemental Regular or Humalog insulin may be given for significant
pre-prandial hyperglycemia.
25
2. If patient is newly diagnosed, start him/her on a b.i.d. or t.i.d. subcutaneous
insulin injection regimen as follows:
*
Total daily dose 0.6 – 1.2 units per kilogram of body weight per day
given as
a.m. pre-breakfast
2/3 – 3/4 of total, calculated daily dose with
1/4 – 1/3 as fast-acting Humalog and
2/3 – 3/4 as intermediate acting NPH
p.m. pre-dinner
1/8 – 1/6 of total, calculated daily dose as
fast-acting Humalog
h.s. pre-bedtime snack 1/8 – 1/6 of total, calculated daily dose as
intermediate acting NPH or long-acting UltraLente
Note: If the patient is to receive only a b.i.d. insulin injection regimen
after discharge, the bedtime intermediate NPH may be
combined with the pre-dinner fast-acting Humalog and
administered together as a single pre-dinner injection.
Note: The above dosage recommendations are only rough guidelines
and should individualized for each patient’s unique
requirements.
Note: Most newly diagnosed patients with diabetes are relatively
insulin resistant, even after the diabetic ketoacidosis has
resolved. As a result, the insulin dose they are discharged on is
often higher that the daily insulin dose they require after a few
weeks.
26
VI.
COMPLICATIONS OF DKA THERAPY
A.
Cerebral Edema
Most patients with diabetic ketoacidosis recover without complications when
properly treated. Poor prognostic signs at the time of admission include
hypotension, azotemia, seizures, coma and the presence of an associated
illness. In children, cerebral edema during DKA and its therapy is STILL
a too common cause of death.
A decrease in the level of consciousness may occur normally during the course
of appropriate therapy for DKA but it is always a potential cause for concern.
Computed tomography and magnetic resonance studies of patients with DKA
have demonstrated the existence of mild cerebral edema in almost all patients
often before intravenous fluid replacement has been started. If clinically
significant cerebral edema occurs, it is often after a period of clinical
improvement and often in the first 6 to 12 hours after institution of therapy.
The cause of the deranged CNS function is multifactorial and has been related
to (1) the degree of cerebral edema, (2) the degree or severity of the acidosis,
(3) the degree of dehydration and (4) to various other factors including the
degree of hypoxemia. Although the etiology of this devastating complication
of DKA remains unknown, theories include:
a. osmotic disequilibrium between the brain and plasma as the blood glucose
is rapidly lowered (i.e. glucose lowered at > 100 mg/dl/hr). Rapid falls in
plasma glucose or osmolality during fluid replacement therapy have both been
associated with the occurrence of cerebral edema. In one study, the
development of coma was correlated with serum osmolalities 320 but NOT
with the degree of acidosis.
b. decreased plasma osmotic pressure due to infusion of large amounts of
free water (i.e. fluid intake > 4000 ml/m²/day). The failure of the corrected
sodium to rise during rehydration indicates the excessive administration of
free water.
c. insulin-induced ion flux across the blood-brain barrier. Administration of
bolus bicarbonate therapy has been related to the occurrence of a worsening
mental status/sensorium.
27
The diagnoses of cerebral edema is suspected clinically when any of the following
symptoms or signs are present:
EARLY SIGNS:
Coma scale 10
Headache, recurrent and severe
Decreasing mental status (disorientation, decreased cooperation, decreased level
of consciousness)
Increased blood pressure with decreased pulse rate and respiratory insufficiency
(Cushing’s Triad)
LATE PHENOMENA:
Papilledema
Unilateral pupil dilation and other focal neurologic signs
Vomiting, recurrent and persistent
Treatment:
To be of benefit, treatment must be initiated STAT as soon as the patient’s
clinical course suggests the presence of increased intracranial pressure and
cerebral edema (i.e. altered mental state and coma scale 10).
Treatment consists of:
1. Bolus infusion of 1cc of D50W per kilogram of body weight
(maximum 50cc/dose).
2. Bolus infusion of 20 % mannitol at 0.5 - 1.0 gram per kilogram of
body weight given over 30 to 60 seconds. Bolus may be repeated
every 2 to 4 hours as clinically indicated.
3. Decrease total IV fluid administration to 100 - 150 % of
maintenance.
4. Elevate head of bed to 30 degrees. Perform frequent neuro checks
(i.e. every 30 minutes).
5. Intravenous Dexamethasone at 0.5 – 1.5 mg per kilogram of body
weight IV push over 30 to 60 seconds.
6. Control airway and intubation with hyperventilation to an arterial
pCO2 of 28 to 30 mm. Lower values of pCO 2 should be avoided
since such values can result in cerebral ischemia.
7. Re-evaluate insulin requirements.
28
B.
Other complications of diabetic ketoacidosis include:
a. vascular thrombosis from volume depletion, hyperosmolality, increased
blood viscosity and changes in clotting factors favoring thrombosis
b. adult respiratory distress syndrome (ARDS). Although its cause is
unknown ARDS in DKA is most likely related to the metabolic acidosis
Diabetes is a complex disorder that requires a multidisciplinary team to interact with the
patient in order to achieve maximum benefit. It is crucial that the child and family receive
appropriate education from a Pediatric Diabetes Team after the initial metabolic problem has
resolved and the patient’s status is stable.
29
NUTS and BOLTS of DKA MANAGEMENT
I.
Initial Evaluation
History:
Presence of concurrent illness; missed/omitted insulin dosages
Physical:
ABCs; mental status/coma scale
vital signs; weight
hydration status; fruity breath/Kussmaul’s respirations
concurrent infection
Laboratory:
glucose, at bedside and by laboratory
pH and pCO2
urine/serum ketones (-hydroxybutyrate)
calculated serum osmolality and anion gap
Na/K/Cl/CO2
BUN/Creat/Ca/Phos/Mg
CBC with differential
new IDDM (islet cell antibodies, anti-GAD antibodies, insulin, C-peptide,
Hemoglobin A1C)
II.
Fluids
a. Estimate fluid deficit (5,10,15%) and 48 hours maintenance requirements.
b. Give initial bolus: isotonic (0.9%) NaCl 10-20 ml/kg. May repeat as indicated by
patient’s clinical status. Continue replacement with isotonic (0.9%) NaCl until IV
dextrose added, then change to ½ (0.45%) normal saline unless patient remains
hyponatremic.
c. Rehydrate over 48 hours. Give ½ calculated fluid deficit over first 24 hours.
Give the remainder over next 24 hours.
d. Maintain total fluids at < 4000 ml/day or < 250 % of maintenance unless clinical
findings dictates otherwise.
e. Continuously assess ongoing fluid losses and replace as needed.
f. Potassium supplementation added after renal function status established and if
initial serum K 5.0 mEq/L. Give 20-40 mEq/L as ½ KCl and ½ KPO4. Increase
concentration to 60 mEq/L if patient hypokalemic.
g. Start IV dextrose when blood glucose 400 mg/dl OR if blood glucose falling at
greater than 100 mg/dl/hour. Give IV dextrose to maintain serum glucose
between 200-250 mg/dl and the glucose (grams per hour) to insulin (units per
hour) ratio at 4-6 to 1 by raising amount of dextrose administered.
h. Caution with chloride overloading which may promote a non-anion gap metabolic
acidosis.
30
i. Use of bicarbonate reserved for when initial pH < 7.10 and repeat pH fails to
improve after initial fluid bolus(es) resuscitation (i.e. repeat pH < 7.10 one hour
after initial results). Give bicarbonate at 0.5 mEq/kg over 1-2 hours AND
NEVER as a bolus unless patient in full cardiorespiratory arrest.
III.
Insulin
a. Standard therapy:
1. give initial loading dose of 0.25-1.0 units/kg SQ or IM. May repeat in 1-2
hours if blood glucose remains > 500 mg/dl.
2. maintenance: 0.25-1.0 units/kg SQ every 3-4 hours until ketones clear.
3. do NOT give insulin SQ if vascular perfusion is compromised.
b. Low-dose insulin infusion therapy:
1. initial bolus: 0.025-0.1 units/kg IVP unless initial pH > 7.15 or blood glucose
level < 400 mg/dl.
2. maintenance: mix fast-acting (Regular or Humalog) insulin in isotonic (0.9%)
normal saline at desired concentration. Change solution every 24 hours.
Piggyback insulin infusion unto IV fluids given for hydration. Do NOT,
however, administer insulin in the same IV tubing as calcium. Do NOT mix
the bicarbonate directly into the insulin infusion IV bag.
Give continuous insulin infusion at 0.1 units/kg/hour.
If serum glucose decreases to 200 mg/dl, raise IV dextrose infusion rate or
concentration AND hold insulin infusion until hypoglycemia resolves. Once
serum glucose rises > 200 mg/dl, restart insulin infusion but at a greater
hourly glucose to insulin ratio.
It is important that when insulin infusion is terminated that patient receive SQ
fast-acting insulin 20-30 minutes prior to (Regular), or immediately
(Humalog) upon discontinuation of the insulin infusion.
IV.
Monitoring
a. Clinical:
1. perform vital signs including blood pressure and Neuro checks every 1-4
hours until ketoacidosis resolves and patient is stable.
2. maintain strict Intake and Output while patient on IV fluids.
3. check weight.
b. Laboratory:
1. hourly bedside capillary glucoses with intermittent corroborating serum
glucose sampling by hospital laboratory.
2. pH and pCO2 every 2 hours until pH > 7.25.
3. lytes/CO2/calculated osmolality and anion gap every 2-4 hours.
4. urine ketones q8-12 hours. Serum -hydroxybutyrate every 8-12 hours if
rapidly available.
5. BUN/Creat/Ca/Phos/Mg q8-12 hours.
31
V.
Complications
a. Cerebral edema:
1. to be beneficial, treatment must be initiated AS SOON AS the patient’s
clinical course suggests the presence of an increased intracranial pressure and
cerebral edema (i.e. altered mental status, coma scale < 12, Cushing’s triad
[increased blood pressure, decreased heart rate and respiratory insufficiency],
papilledema or focal neurological signs such as unilateral pupil dilation).
2. treatment consists of:
bolus infusion of 1cc/kg D50W (maximum 50cc/dose)
bolus infusion of 20 % mannitol at 0.5-1.0 gr/kg over 30 seconds
lowering IV fluid rate to 100-150 % of maintenance
elevating head of bed to 30 degrees
controlling airway and intubation with hyperventilation
b. Thrombosis from volume depletion, hyperosmolality and increased blood
viscosity.
c. Adult respiratory distress syndrome (ARDS).
VI.
Evaluate and treat for an underlying inciting condition that may have precipitated the
DKA (i.e. infection; psychosocial instability; non-compliance)
VII.
Please see DKA protocol for complete details.
32
NUTS and BOLTS of DKA MANAGEMENT
I.
Definition
blood pH < 7.30
serum bicarbonate < 15 mEq/L
II.
Goals of Treatment
correct volume depletion
correct acidosis/abolish ketosis
replace electrolyte losses
avoid complications
III.
Initial Evaluation
History
presence of concurrent illness
missed/omitted insulin doses
IV.
Fluids
estimate deficit and
maintenance requirements
initial bolus: 10-20 ml/kg NS
may repeat as indicated
rehydrate over 48 hrs: give
½ over first 24 hrs, remainder
over next 24 hrs.
assess ongoing losses
maintain total fluids < 4L/day
unless higher volumes indicated
give initial fluids as NS;
change to ½ NS when adding
dextrose to IV
add IV dextrose when blood
glucose < 400 mg/dl OR
dropping by 100 mg/dl/hr
add K at 20-40 mEq/L to IV
(½ KCl and ½ KPO4) once
know serum K conc. and
renal function status
V.
Insulin Infusion
initial bolus 0.025-0.1 u/kg
unless pH > 7.15 or
blood glucose < 400 mg/dl
insulin drip 0.05-0.1 u/kg/hr
maintain glucose:insulin ratio
at 4 to 6 grams/hr per unit/hr
Physical
ABCs
mental status/coma scale
vital signs
weight
fruity breath/Kussmaul’s
hydration status
concurrent infection
Laboratory
glucose, bedside and laboratory
pH and pCO2
urine/serum ketones (-OHbutyrate)
calculated serum Osmo/anion gap
Na/K/Cl/CO2
VI.
BUN, Creat, Ca, PO4 , Mg
CBC with diff.
new IDDM (ICA, anti-GAD, Hgb A1C,
insulin, C-peptide)
Monitor
bedside glucose hourly
pH/pCO2 q2hrs till pH > 7.25
lytes/CO2 q2-4hrs
calc. osmo/anion gap q2-4hrs
urine ketones q8-12hrs
serum -OHbutyrate (if avail)
BUN/Creat q8-12hrs
Ca/Phos/Mg q8-12 hrs
I/Os while on IV fluids
Neuro checks q1-4hrs till DKA
resolves
33
BIBLIOGRAPHY
Levin, DL and Morriss, FC, Essentials of Pediatric Intensive Care, Vol. 1, 2d Ed. Chapter
58: 565-570, 1997.
Menon, RK and Sperling, MA, Diabetic Ketoacidosis. Pediatric Critical Care Chapter 70:
797-804, 1992.
Weigle, C, Metabolic and Endocrine Diseases in Pediatric Intensive Care. Textbook of
Pediatric Intensive Care, Rogers Chapter 31: 1058-1070, 1987.
34