Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
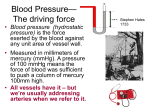
Adam Manko, M.D. PGY-3 Internal Medicine University Hospitals Case Medical Center Sepsis – Definition Initial Management Medications Mechanical Ventilation - Briefly What Your Senior Expects From You Summary 69 y/o Male presented to ER with shortness of breath. VS 38.3 88/46 114 28 86% He is placed onto 50% ventimask, but continues to have low oxygen saturation and is intubated in the ER. He is given 2L of NS and repeat BP is 92/44 The Patient arrives in the MICU…..what do you do next? Sepsis is a continuum….. SIRS Sepsis Severe Sepsis Septic Shock Refractory Septic Shock Multi-Organ Dysfunction Syndrome (MODS) SIRS Criteria ◦ ◦ ◦ ◦ Temperature >38.3 (or >38.0 for 1 hour) or <36.0 WBC >12k or <4k, or >10% bandemia RR >20, or paCO2 <32mmHg HR >90 Sepsis = SIRS + suspected infection ◦ Does not have to be culture proven infection to begin treatment for Sepsis Severe sepsis = sepsis + and signs of at least one organ dysfunction thought to be from tissue hypoperfusion ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ Hypotension Elevated lactate Urine output <0.5ml/kg Acute Lung Injury with PaO2/FiO2 ratio of <250 ARDS Acute Renal Failure Elevated bilirubin Platelet Count <100,000 Coagulopathy with INR >1.5 Altered Mental Status Abnormal EEG findings Cardiac Dysfunction “Early Goal Directed Therapy” ◦ ◦ ◦ ◦ ◦ ◦ ◦ Goal SBP >90 Goal MAP >65 Goal Hemoglobin 7-9 Goal urine output >0.5ml/kg/hr Goal normalized serum lactate Goal Mixed Venous >70% Central Venous >65% Goal SBP >90, MAP >65, Hgb 7-9 IVF bolus with NS What if you give IVF and remains hypotensive? ◦ Need to check a CVP!!! CVP ◦ = Central Venous Pressure What is the utility of a CVP ◦ Estimates the Right Atrial Pressure ◦ What is a Normal Right Atrial Pressure <6 Place a CVC = Central Venous Catheter Locations include ◦ Internal Jugular ◦ Subclavian CVP >8 If intubated, CVP >12 What if still hypotensive but at goal CVP? Norepinephrine ◦ First Line pressor (preferred agent over dopamine (NEJM 2010 Comparison of Dopamine and Norepinephrine in the Treatment of Shock) ◦ Mainly A1, some B1 ◦ Dosing in mcg/min Typically uptitrate to max of ~30 mcg/min Vasopressin ◦ Second line pressor ◦ Entirely V1 Can be titrated, however we typically turn it “on or off” at dose of 0.04 U/min Phenylephrine ◦ Weaker pressor, A1 activity ◦ Less arrhythmogenic Dopamine ◦ Dose dependent ◦ Low dose 1-3mcg/kg/min = “renal” dosing, almost all D1 ◦ Medium dose 3-10mcg/kg/min = B1 and D1 ◦ High Dose >10mcg/kg/min = “pressor” dosing Epinephrine ◦ “king of pressors” ◦ Used as last line pressor at our institution ◦ Side effect includes increased risk of intestinal ischemia Pressor photo Mixed Venous >70 ◦ Mixed venous taken from a swan-ganz catheter Central Venous >65% ◦ Taken from Central Line in the SVC High Venous saturation with unclear utility Low Venous saturation means increased extraction peripherally How to increase mixed venous saturation, you have 2 option ◦ Increase hematocrit ◦ Increase cardiac output Dobutamine Consider when refractory hypotension ◦ when you are adding 2nd pressor, think of adding steroids!! No longer recommended to do ACTH stim or random cortisol Empirically add hydrocortisone, dose 50mg q6h Antibiotics within 1 hour Typically vancomycin and zosyn are first line agents if unclear of source Start broad and narrow when source identified ABX photo from UH guide Maintain tight blood glucose control with goal 140-180 If unable to manage easily (you get 2 tries with SQ insulin) then start on insulin gtt Protocol driven by nursing ◦ FYI this is different than the DKA protocol ◦ (2010 NEJM – Glycemic Control in the ICU) DVT ◦ If no contra-indications…. Heparin SQ preferred agent ◦ If contraindications SCDs and TED hose Stress Ulcer ◦ PPI or H2 blocker Protective Lung Ventilation Strategy ARDSnet protocol ◦ Low tidal volumes 6ml/kg of IBW ◦ PEEP ◦ Goal plateau pressure <30 (2007 NEJM - Low Tidal Volume Ventilation in the Acute Respiratory Distress Syndrome) (2000 NEJM – Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome) ARDS NET photo RRT = Renal Replacement Therapy ◦ HD = Hemodialysis ◦ UF = Ultrafiltration CRRT = Continuous Renal Replacement Therapy ◦ CVVH = Continuous veno-venous hemofiltration ◦ CVVHD = Continuous veno-venous hemodialysis A ◦ Acidosis E ◦ Electrolyte imbalance I ◦ Intoxication O ◦ Fluid Overload U ◦ Uremia Sedation ◦ ◦ ◦ ◦ ◦ Versed for anxiety Fentanyl for pain Haldol for agitation Propofyl Precedex Assess the patient!! (Go into room, not look in EMR first) Labs ◦ CBC ◦ RFP ◦ LFTs ◦ Coag ◦ Type and Screen ◦ Lactate!!! ◦ In the right setting Troponin, amylase, lipase, etc Microbiology ◦ Blood cultures x2 ◦ UA and culture ◦ +/- sputum culture Imaging ◦ CXR, +/- KUB ◦ CT in right setting Check for Access ◦ Prep for CVC If hypotensive, need invasive hemodynamic monitoring ◦ Central Line (CVC) ◦ Arterial Line Other ◦ HD Catheter? ◦ Introducer (Cordis)? Get us if you are uncomfortable in a situation, aka the patient is very sick and crashing!! STAY CALM!!! Nurses are your friend or worst enemy, the choice is yours!! ◦ They have taken care of more patients than you, they often know what the next step is, use them as a resource!! In Summary, the Goals of Sepsis are…… 69 y/o Male presented to ER with shortness of breath. VS 38.3 88/46 114 28 86% He is placed onto 50% ventimask, but continues to have low oxygen saturation and is intubated in the ER. He is given 2L of NS and repeat BP is 92/44 The Patient arrives in the MICU…..what do you do next? Identify Severe Sepsis and Septic Shock Early IVF Early invasive hemodynamic monitoring Goal endpoints ◦ Urine output, SBP, MAP, lactate, central venous sat, CVP <8 or 12 ◦ Pressors and Steroids Cultures and ABX Thank you!!!