Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
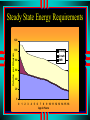
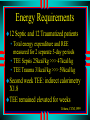
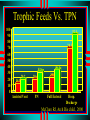
The Science of Effective Pediatric Inpatient Nutrition 2005 Kevin M. Creamer M.D., FAAP Medical Director, PICU WRAMC Chief, Pediatric Nutrition Support Team A hypothetical case Starvin Marvin is a 2 y.o. who presents with a 2-3 week Hx of fevers, weight loss, pallor, decreased energy, appetite and activity PE reveals Wt 13kg , down 1.5 kg, pallor, petechia,+ HSM Labs reveal WBC 26 K with 50% blasts, anemia and thrombocytopenia Hospital Course Day 1 - NPO, IVFs, labs, Xrays Day 2 – NPO for BM and LP, as well as Hickman Day 3- Chemo, picky PO Day 4-6 - continued poor PO, with emesis occasionally Day 7-10 – emesis resolves, PO inadequate Day 12 – pancytopenia, sepsis with GNR Teaching points Nutritionally-at-risk from the word GO • Debilitated Ortho spine patient • Recurrent bowel obstruction patient No nutrition plan, No monitoring, No intervention Hope is not a method Could sepsis event been avoided?? Inpatient Nutrition Goals Think about nutritional status on every patient Outline the dynamic between illness, nutritional state and secondary morbidity Recognize need to estimate/calculate goals calories in order to reach the goal • Individualized goals for time course, and disease process Institute effective nutrition support with the help of Pediatric nutritionist Acute Stress The 5 W’s of Inpatient Nutrition Why, Who, When, Where, What ? Acute Stress Major Surgery, Sepsis, Burns, Trauma • Result in massive outpouring of catechols, ACTH, GH, ADH, glucagon, somatomedins – Insulin inhibition, elevation of glucose and free fatty acids • ↑ Inflammatory Cytokines: TNF, IL 1, IL-6 – PMN release and degranulation Mucosal permeability hormones and mediators ↑ release of cAMP which down-regulate lymphoid immune activity Stress Acute Stress NPO state starves gut mucosa • Gut mass 50% in 7 days of fasting • Gut contains 80% of body’s immune tissue – “GALT and MALT” • Intestinal sIgA ↓ in 5 days • ↑ Th1 pro-inflammatory lymphocytes Major stress doubles protein turnover • Skeletal muscle cannibalized for fuel for enterocytes (glutamine) Stechmiller JK, Am J Crit Care, 1997 Bacterial Translocation Disruption of mucosal barrier • Ischemia-reperfusion during shock risk of ulceration and permeability Bacterial translocation • Culture(-), found bacterial DNA in blood stream Cytokine amplification in lymphatics and liver Bacterial Translocation Enteral nutrition can prevent translocation • Trophic feeds stimulate gut hormones and nourish mucosa, increase blood flow, re-energize tight junctions, improve brush border • Enteral vs. Parenteral feeds - postop septic related complications Enteral feeds stimulate Th2 lymphocytes which PMN adhesion in lung Deitch EA, Ann Surg, 1987, 1990;Border JR, AnnSurg, 1987; Carrico CJ, Arch Surg, 1986; Alverdy JC, Surgery, 1988; Moore J, JPEN, 1991,Kudsk,Am J Surg, 2002 WHY ? Is nutrition such a big deal? Malnutrition Prevalence Nutrition Status and Outcomes Gut Bacterial Translocation Malnutrition Prevalence 15 to 50 % of hospitalized pediatric inpatients are malnourished on presentation (down from 35-65%) • 15 to 20 % of critically ill patients • 33% patients with congenital heart disease • 39% awaiting elective surgery Parsons, AJCN,1980; Mize, Nutr Supt Ser, 1984; Merritt, Am J Clin Nutr, 1979, Huddleston KC, CC Clin of NA, 1993, Cameron, Arch Ped 1995, Cooper, J Ped Surg 1981 Malnutrition Snapshot Inpatient population of Boston Children’s Hospital was surveyed Sept 24,1992 • 268 children ages 0-18 years Using Waterlow criteria: • 25% were acutely malnourished, 27% were chronically malnourished Of 17 ICU patients, 4 (24%) were classified with severe PEM Hendricks, Arch Ped Adol Med, 1995 Nutrition and Outcome State of nutrition vs. LOS and Cost 18 16 14 12 10 8 6 4 2 0 $16,691 $14,118 $7,692 Normal Borderline Malnourished Robinson G, JPEN, 1987 Nutrition and Outcome Low Prealbumin 95% specific, in 147 consecutive admissions 8 measures of malnutrition in 134 patients 50 cardiac surgery patients assessed • Low Prealbumin predictive post-op infectious complication 20 18 16 14 12 10 8 6 4 2 0 PCM No PCM PCM* No PCM* LOS Mortality (%) Potter, Clin Invest Med, 1999; Weinsier,Am J Clin Nut, 2005 Leite, Rev Paul Med, 1995 Parameter Low Risk High Risk Hosp. Days 7 13.5 Mech. Vent. 0 8.5 NPO days 3 8.5 Days on O2 4 20 P< 0.02 Nutrition Screen predictive of outcome in 25 RSV PICU admits Mezoff, Pediatrics, 1996 Nutrition and Outcome 60 PICU patients had nutrition status evaluated, with PSI, and TISS applied Acute PEM associated (P<0.01) with physiologic instability, mortality and quantity of care Malnutrition can result in delayed wound healing, respiratory failure, increased potential for infection, death Pollack MM, JPEN, 1985 Nutrition and Outcome Ventilator Patients: Weaned Died No Specific Nutrition Plan 18 15 Focused Nutrtional Care 13 1 Bassili HR, JPEN,1980 Nutrition and Outcome PICU Outcomes in 323 patients after Nutrition support team instituted • Use of Enteral nutrition (EN) in medical patients increased 25% to 67% Mortality risk decreased 83% for those receiving EN >50% of LOS • EN independent predictor of survival in multiple regression analysis. Gurgueira, JPEN, 2005 WHO ? Needs to know? Gets assessed? ALL Physicians! ALL Patients! Nutrition Dichotomy 79 FP residents • Nutrition Interest (72.2%) vs. Perceived Knowledge – Parenteral and enteral nutrition 34.2%, Infant nutrition 27.5 %, Nutrition assessment 17.7% 3416 Primary Care physicians • < 40% practiced what they preached Lasswell AB, J of Med Ed, 1984, Levine BS, Am J Clin Nut, 1993 Nutrition Practice: Uphill battle Adult ICU group found their patients only received 52% of goal calories • Reasons included physician under ordering, frequent cessations, and slow advancement Designed a protocol but only 58% went on it Spain, JPEN, 1999 I wonder if I’m missing out on some critical piece of information Nutrition Screen Should be completed within 24 hours of admission High risk surgical patients should be screened weeks to months ahead of planned surgery In your continuity clinic • Multidisciplinary team • Supplement , reassess, or reschedule Nutritionally-at-risk Weight for age < 10th % tile Weight for Height < 10th % tile Acute weight loss > 5% over 1 month or >10% total Birth weight < 2 SD below mean for gestational age Increased metabolic requirements 2 chronic disease Impaired ability to ingest or tolerate oral feeds Weight % tile crossing 2 contour lines over time (FTT) Prealbumin Transthyretin has nothing to do with albumin • Small body pool and half life of 2 days makes prealbumin an reasonable monitor of visceral protein homeostasis Drops during the first 3-5 days of stress it should rise thereafter Daily rise of 1mg/dl indicates anabolism Plasma Protein Stress Response CRP Prealbumin Fleck, A. Br J Clin Pract, 1988 Prealbumin as a predictor Surgically stressed Infants • Prolonged ↑ CRP with ↓ Prealbumin had ↑ mortality – Strongest predictor POD#5 prealbumin depression Prealbumin ideal nutrition screen for: • 50 children with solid tumors – before and during chemo • 86 Adult post-op patients requiring TPN Chwals WJ, Surg Clin NA, 1992, Elhasid, Cancer, 1999, Erstad, Pharmaco, 1994 Prealbumin Measure twice weekly Once 65% of needs met expect levels to rise 1mg/dl a day If weekly rise is less than 4mg/dl • check N2 balance and CRP to determine if cause is nutritional inadequacy or ongoing SIRS Expert roundtable, 10th World Congress of Gastroenterolgy WHEN? Should I start? Early Enteral vs Standard timing Enteral Contraindications Intubation/extubation planned within 4° Hemodynamic instability requiring escalation in therapy Intestinal obstruction Massive UGI bleed Gut ischemia I’m nervous about this kid Early feeds vs. Standard Adults with gut malignancies and neurotrauma has shorter LOS and fewer infections when fed early 19 controlled studies (24° vs 3-5 days) • 16/19 studies showed improved outcome • Improved healing, complications and LOS • Recommended for critically ill surgical pts Braga, CCM, 2001 Grahm T, Neurosurgery, 1989 Taylor, CCM 1999 Heyland DK, CC Clin of NA, 1998 Zaloga. CCM 1999 Early feeds: Pediatrics Tolerated pediatric burn patients 42 ventilated children (76% on vasoactive meds) • Transpyloric feeding tubes placed at bedside • 74% of patients reached full feeds within 24 hrs, rest within 48 hrs – No complications Chellis MJ, JPEN, 1996, Trocki, Burns, 1995 All is Not Rosy All Mechanical Ventilated patients Lots of exclusions Group Early (75) Late (75) p VAP 49.3% 30.7% .02 C diff 13.3% 4.0% .042 ICU stay 13.6± 14.2 9.8 ± 7.4 .043 Mortality 20% 26.7% .334 Ibraham, JPEN, 2002 WHERE? In the gut do I put the food? Oral vs.Tube feeding Gastric vs. Transpyloric feeds Tube Feeding Considerations Nutritionally-at-risk with inadequate oral intake for the past 3-5 days. Meeting <50% estimated needs orally for previous 7-10 days. • Shorten to 3-5 days if traumatized or severely catabolic Disease state preventing adequate P.O. intake for >5 days Gastric vs. Transpyloric No aspiration difference in 54 patients receiving gastric vs transpyloric radiolabeled feeds 33 mechanicaly ventilated Micro-aspiration 7.5 >> 3.9% in NJ fed patients 80 adult trauma victims • Duodenally fed patients reached goal calories 34 vs. 44 hours with had less pneumonia 27% vs 42%* 80 ventilated adults randomized • gastric feeds + E-mycin 200 mg q8 (55% / 74%) • Transpyloric feeds (44% / 67%) Esparza, Intens C Med, 2001,Kortbeek, J Trauma, 1999, Heyland, CCM, 2001, Boivin, CCM, 2001 Transpyloric 59 ventilated children randomized to receive continuous or interrupted transpyloric feeds during the day before and of extubation • Continuous group got >90% goal calories both day vs 73% and 46% • No aspiration events or difference in adverse events Lyons, JPEN, 2002 Neuromuscular blockade and ECMO? May decreased REE by 10-15 % Primary Neurotransmitter in Gut is VIP not acetylcholine • Neuromuscular blockade work via AcH receptors By what mechanism do neuromuscularly blocked patients become intolerant of enteral feeds? • Gastric atony 2° Benzodiazepines and narcotics Enteral feeds for Pediatric ECMO patients is safe with trends toward improved survival Pettignano, CCM, 1998 Enteral Pitfalls 2 adult studies with 95 ICU pts, had 66%-78% of goal feeds prescribed, 52%- 71% delivered • Gastric Intolerance (Residuals #1) – BZD and Narcs effect stomach > intestine • Airway management – 22/26 PICU pts had feeds held for extubation that only 5 got • Diagnostic procedures – Some ventilated patients fed right up to OR McClave SA, CCM, 1999,DeJonghe, CCM, 2001, Fry-Brower +McCunn, CCM(a), 2002, WHAT? Amount of calories do I Feed Them? How much to feed Trophic feeds Enteral vs. Parenteral Lipid phobia Caloric Goals? Brazilian PICU reviewed 37 charts Only 3 had an assessment done in 425 days No Patient had caloric goals set • Only 29.7% met goals • 80.5 % fed Parenterally Leite, Rev Assoc Med Bras, 1996 Steady State Energy Requirements 120 Calories per Kilogram 100 Activity Growth BMR 80 60 40 20 0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Age in Years Energy Requirements Calorie needs change during the course of the hospitalization. • Hemodynamically unstable? • Ventilated vs Extubated Ebb phase (Hypometabolic): obligate (–) nitrogen balance during acute critical illness • No need for growth calories (BMR may suffice?) • Watch out for overfeeding – Steatosis, Hyperglycemia, Hypertriglyceridemia Therapeutic window 187 critically ill adults >96º in ICU • Tertiles of % ACCP recommended caloric intake Patients receiving 33-65% goal Vs. <33% (18kcal/kg) • OR survival 1.22, discharge without sepsis 1.2, without vent 1.8 • Patients > 65% goal OR 0.82, 0.75, 0.69 Sickest patients (SAPS>50) • Did worse when they received >33% goal Krishnan, Chest, 2003 Energy Requirements Flow phase (Hypermetabolic) • As the child improves and becomes anabolic, calorie needs for growth and activity must be included Underestimating needs can increase risk for infection, poor wound healing, poor growth, and overall poor outcome Energy Requirements 12 Septic and 12 Traumatized patients • Total energy expenditure and REE measured for 2 separate 5-day periods • TEE Sepsis 25kcal/kg >>> 47kcal/kg • TEE Trauma 31kcal/kg >>> 59kcal/kg Second week TEE: indirect calorimetry X1.8 TEE remained elevated for weeks Uehara, CCM,1999 1º Fever ↑12% Trophic Feeds fed 15% calories enterally had permeability and bacterial translocation 10 post-op infants fed trophically (21cal/kg/d) had improved Staph killing vs TPN alone Rats • 37% vs. 52% vs. 65% (Controls) – Related to production of TNFα > 6kcal/kg (>25% ACCP cal goals) in 138 adult MICU patients reduced BSI (relative hazard 0.24) Omura, Ann Surg, 2000, Okada, J Ped Surg, Robinson,CCM, 2004 Trophic feeds Feed type # Patients Mortality SMR Enteral 167 25% .71 Parenteral 26 54% 1.4 Parenteral + Trickle 24 38% .9 Trophic feeds are stress ulcer and antibiotic prophylaxis rolled into one Marik, CCM(a), 2002 Trophic Feeds Vs. TPN 100 90 80 70 60 50 40 30 20 10 0 92.4 70.3 36.1 32.6 14.1 20.2 Assisted Vent 20.6 PN 24.8 Full Enteral Hosp. Discharge McClure RJ, Arch Dis child , 2000 Enteral Feeds vs. TPN Enteral feeds in Critically ill population • improve wound healing, mucosal permeability > 10 studies show enteral feeds are safe, feasible and cheaper than TPN Meta analysis adult ICU patients Enteral feeds vs. TPN RR infection 0.66 Schroeder D, JPEN, 1991, Hadfield R, Am J Resp Crit Care Med, 1995 Robert Dimand, UC Davis, Peds CC Update 2002, Gramlich, Nutrition, 2004 TPN vs. Hope Meta Analysis 26 studies (210 reviewed) • 2211 patients • Trend toward reduced complications in TPN patients (risk ratio 0.84) 4 studies used TPN > 3 weeks • Mortality in TPN pts was 6.8% vs. 12.4% Meta Analysis 11 studies • Parenteral nutrition vs. delayed enteral improved mortality • Increased infectious risk (OR 1.65 CI1.1-2,5) in PN vs. all enteral Heyland DK, JAMA, 1999, Simpson, Int Care Med, 2005, Doig, CCM(A) 2005 Parenteral Considerations Nutritionally-at-risk patient with non- functional gut. Adequate nutritional status on admission but non-functioning gut 3-5 days after admission “The major advance in TPN since the 1980’s is that it is not used as much” Lipid Phobia? When infants given TPN without lipids • CHO only TPN resulted in amino acid oxidation, proteolysis, CO2 production and lipogenesis Lipid requirements • Essential fatty acid (0.5gm/kg/d), Promote Nitrogen sparing, Increased lipid clearance during stress Balanced approach to fulfilling energy requirements Bresson, Am J Clin Nut 1991,Tilden, AJDC, 1989, Schears, Crit Care Clin, 1997 Lipids Original 10% lipid compounds – Intravenous fat emulsions contain 50-60% linoleic acid a precursor to arachidonic acid – May disturb balance between thromboxane and prostacyclin production Modern 20% emulsion cause less Trig • Neonates clear better, less phospholipids • No problems with oxygenation when given as 1824° infusion • No immune problems when Triglycerides <700 Monitor Outcomes Residuals Age appropriate weight gain Diarrhea / Constipation Medication Compatibility? Emesis / Aspiration Proper wound healing Fluid and electrolyte balance Euglycemia Improved N2 balance and Prealbumin HOPE IS NOT A METHOD! Who? Is you, screening all your patients Why? They’ll do worse if you don’t When? The sooner the better What? Enteral better, even trophic better than TPN alone Where? PO>NG>NJ > IV