Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
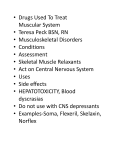
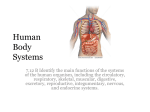
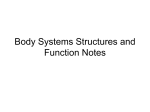
Beheshti Univ Dent J 2005; 22(Special Issue): 100-106 The association between occlusal features and craniofacial structure Downloaded from jds.sbmu.ac.ir at 10:54 +0430 on Friday May 5th 2017 Safavi S.M.R. DDS, MS1, Tahmasbi S. DDS 2, Shoai SH. DDS2 1 Assistant Prof., Dept. of Orthodontic, Dental School, Shahid Beheshti University of Medical Sciences, Tehran-Iran; 2Dentist. ABSTRACT Purpose: To investigate the relationship between craniofacial skeletal structure and occlusion. Materials & Methods: Data were obtained from lateral cephalometric radiographs and study casts of 60 patients with various malocclusions, with the mean age of 13.3±1.5 years. Thirteen angular and 14 linear skeletal measures as well as 5 occlusal measures including; overjet, overbite, molar relation, maxillary and mandibular crowding were applied. Relations were examined by use of univariate and multivariate statistical methods. Results: Simple correlation analysis between individual skeletal measures and individual occlusal characteristics showed that the strongest linear correlation exists between overbite and Pal-GoMe angle (r=-0.451, P-value≤0.01). Stepwise multiple regression was carried out for quantitative occlusal variables. The prediction formula for overjet had the highest multiple R and R2 values (multiple R=0.654, R2= 0.428), which shows that multiple skeletal features explained 43% of the variance in overjet. Conclusion: Individually and in combination, skeletal measures were poorly associated with individual features of occlusion, so that variations in skeletal structure account for at most 43% of the variations in occlusion. _______________________________________________________________________________ Keywords: Occlusion, Craniofacial structure, Association. INTRODUCTION O cclusion varies from optimal to severe malocclusion, with continuous variation between the two and reflect bone growth, dental development and neuromuscular maturation. The concept that definitive relationships exist between occlusion and craniofacial morphology is well known to orthodontists.(1-3) It has been argued that orthodontic diagnosis might be facilitated if the relationship between occlusion and craniofacial structure were better understood.(1) The orthodontist needs to know how the major functional components of the face (cranial base, jaws, teeth) are related to each other.(2) Numerous studies have examined the relationship between craniofacial morphology and a single characteristic of occlusion such as openbite,(4-7) deep bite,(8,9) mandibular and Angle anterior crowding(10-12) classification.(13-16) Others have examined the correlation between craniofacial structure and multiple features of occlusion.(16,17) The results of these studies often are contradictory because of several problems inherent in examining the association between craniofacial structure and occlusion. Not only do most samples rarely include a typical assortment of occlusal variation, but the Angle classification schemes alone do not 100 Downloaded from jds.sbmu.ac.ir at 10:54 +0430 on Friday May 5th 2017 Safavi et al. best represent that variation.(1) In addition, a malocclusion is the combination of several individual skeletal problems of which none may be remarkable in and of itself.(18,19) The purpose of this study was to examine the relationship between craniofacial skeletal structure and occlusion on a sample of occlusal variation with several angular and linear skeletal measures using univariate and multivariate statistical methods. MATERIALS & METHODS In this analytical study, the data were obtained from pretreatment lateral cephalometric radiographs and dental casts of children in early permanent dentition selected from the archive of Shahid Beheshti University Orthodontic department. There were 37 girls and 23 boys with ages ranged from 11 to 16 years. All subjects met the following criteria: 1. Presence of no primary tooth. 2. Presence of all permanent teeth except for the third molars. The second molars were in various stages of eruption. 3. No premature loss of primary teeth in the orthodontic records. 4. No tempromandibular joint abnormality, mandibular deviation or facial asymmetry. The lateral cephalograms were traced by one investigator (ST). Landmarks were identified as described by Riolo and associates.(20) 13 angular and 14 linear measures were selected to assess: cranial base flexure and length, maxillary horizontal and vertical positions and length, mandibular horizontal and vertical positions and length, anteroposterior and vertical maxillarymandibular discrepancies. All occlusal measurements were taken directly from the dental casts. Overbite, overjet and molar relationship were identified and measured as reported by Solow.(21) Maxillary and mandibular crowdings were measured from one first molar to the other directly on dental casts. The following statistical analysis were performed: 1. Pearson’s product-moment coefficient of correlation to assess the association, among skeletal measures, and between individual occlusal characteristics and skeletal measures. 2. Stepwise multiple regression to determine whether combinations of skeletal measures explained more variance in any single occlusal characteristic than did single measures. In this procedure a skeletal variable was entered and retained in the regression model at each step if it explained a significant amount of variance in occlusal variable at the P=0.05 significance level. Addition of skeletal variables to the model was stopped when no other variable met the 0.05 significance level criterion and R reached to the maximum level. RESULTS The study sample consisted of 37 girls and 23 boys with the mean age of 13.3±1.5 years. The distribution of malocclusion in the sample was approximately similar to that in the Iranian population. Table 1 shows the mean, range and standard deviation of overjet, overbite, maxillary crowding and mandibular crowding and indicates that wide range of occlusal characteristics have been selected in order to strengthen external validity. Figure 1 shows the distribution of cases according to Angle classification. Table 1. Mean, range and standard deviation of occlusal variables(mm). Overjet Overbite Max. Crowding Mand. Crowding Mean SD Maximum Minimum 3.41 2.13 4.03 2.5 2.42 4.17 10 +8 +13 0 -4 -6 3.11 3.48 +13 -4 The correlation among skeletal variables revealed several strong (r≥0.75, P≤0.05) associations, most of them reflecting redundancy or topographic relationship. The significant linear correlation between 101 Beheshti Univ Dent J 2005; 22(Special Issue): 100-106 Downloaded from jds.sbmu.ac.ir at 10:54 +0430 on Friday May 5th 2017 individual occlusal features and individual skeletal measures ranged from 0.275to -0.451 (Table2). Fig 1. Histogram showing distribution of malocclusion in the sample. Overjet showed significant correlation with several skeletal measures while the highest of these correlation were between overjet and A-N-B (r=0.377, P≤0.05) (Fig.2). The strongest correlation between overbite and skeletal structure was found between overbite and Pal-GoMe (r=-0.451, P≤ 0.05) (Fig.3). with other skeletal measures were not statistically significant. Fig 3. Linear correlation between overbite and Pa-GoMe angle (r=-0.451). The only significant correlation of mandibular crowding was found with ANS– Me/N-Me (r=-0.292, P≤0.05). Multiple R and R2 values were calculated with stepwise multiple regression to assess whether linear combinations of skeletal measures explained more variance in any single quantitative occlusal variable than did single measures. Unstandardized and standardized regression coefficients were also determined. Fig 2. Linear correlation between overjet and A-N-B angle (r=0.377). Maxillary crowding showed significant correlation with N-Se (r=-0.302, P≤0.05) (Fig.4) and ramus length, but it’s correlation Fig 4. Linear correlation between maxillary crowding and N-Se (r=0.302). 102 Safavi et al. Table 2. Linear correlation between individual occlusal characteristics and individual skeletal measures. Downloaded from jds.sbmu.ac.ir at 10:54 +0430 on Friday May 5th 2017 Occlusal Skeletal S-N-B S-N-Pog A-N-Per B-N-Per Pog-N.Per N-Se Mandible Man. Dis. Maxila Max. Dis Ramus A.L.F.H ANS-Me/N-Me N-S-Ar S-Ar-Go Ar-Go-Me Sum- Post Pn-Pal Pal-GoMe SN-MeGo N-S-Gn P.F.H A.F.H Jarabak I. S-N-A S-N-B Mand. Crowding NS NS NS NS NS NS NS NS NS NS NS NS 0.292 NS NS NS NS NS NS NS NS NS NS NS NS NS From occlusal variables, the highest multiple R and R2 were related to overjet regression model (multiple R=0.654, 2 P≤0.05), which shows R =0.428, combination of 5 skeletal measures explained 43 percent of the variance in overjet. Overbite prediction formula showed that only 29 percent of the variance in overbite were explained by multiple skeletal measures. The multiple R values of maxillary crowding and mandibular crowding were less than 0.5. DISCUSSION This study investigated the relationship between features of occlusion and craniofacial structure. The simple correlation analysis of overbite with skeletal measures showed that increase of overbite is accompanied with decrease of A.F.H (NMe), A.L.F.H (ANS-Me), sum of posterior angles, SN-MeGo and Jarabak Index Max. Crowding NS NS NS NS NS -0.302 NS NS NS NS -0.284 NS NS NS NS NS NS NS NS NS NS NS NS NS NS NS Overbite Overjet NS NS NS NS NS NS NS NS NS NS NS -0.365 -0.303 NS NS NS -0.300 NS -0.451 -0.354 NS NS -0.327 0.354 NS NS 0.377 -0.282 NS -0.321 -0.339 0.275 NS -0.348 NS NS NS NS NS 0.377 -0.282 NS -0.321 NS NS NS NS NS NS NS NS -0.303 (P.F.H/A.F.H×100). Similar findings have been reported by Bjork(1947),(22) Schud (1964),(23) Solow(1966),(21) Parlow(1972),(24) Keeling(1989),(17) Tsang(1997),(7) and (25) Meyers(1992). However our results showed that individual features of occlusion were poorly related to individual skeletal measures; the highest correlation (r=-0.451) explained only 20 percent (R2=0.20) of the variance between overbite and Pal-GoMe (basal angle). These values were lower than comparable values reported by Beckmann et al(1998)(9) (R2=0.31) but were nearly similar to the findings of Solow(1966),(21) Keeling(1989),(17) and Meyers(1992).(25) In multiple regression, when A-N-B entered the overbite prediction formula, raised r from 0.451 to multiple R=0.537; adding 9 per cent to explained variance. It was interesting that A-N-B, which is an anteroposterior skeletal measure, showed a considerable correlation with overbite, which is a vertical occlusal feature. In anteroposterior relations, simple 103 Downloaded from jds.sbmu.ac.ir at 10:54 +0430 on Friday May 5th 2017 Beheshti Univ Dent J 2005; 22(Special Issue): 100-106 correlation analysis showed that increase of overjet is associated with decrease of S-N-B, S-N-Pog and mandibular length and increase of N-Se. The strongest correlation was found between overjet and A-N-B angle (r=0.377) which indicated that only 14 per cent of the variance in overjet could be explained by AN-B angle. These values are higher than comparable values reported by Solow,(21) Bjork(1947)(22) and Keeling et al(1989)(17) (R2=0.09) but are considerably lower than values reported by Meyers (R2=0.42).(25) The higher values of shared variance reported by Meyers, may indicate that Dipaolo’s quadrilateral measures, which are consistent with Enlow’s counterpart principle and are used in Meyers’ study, better express the relations between variations in anteroposterior skeletal structure and variations in sagittal occlusion than other measures. Another reason for this difference, may be the variation in study sample. The multiple regression between overjet and five skeletal measures, increased multiple R as high as 0.654. This indicated that up to 43 percent of the variance in overjet could be accounted for by the variance in skeletal measures. The interesting point was the relation of vertical skeletal measures such as Pn-Pal, SN-MeGo and Jarabak index, with overjet, a sagittal occlusal characteristic. Although, the skeletal measures used in our study are different from Dipaolo’s quadrilateral measures used in Meyers’ study, the results of multiple regression analysis were similar (multiple R2=0.43). Mandibular crowding showed a significant correlation with ANS-Me/N-Me but it’s correlations with other skeletal measures such as Jarabak index and SNMeGo were not significant. Similar findings have been reported by Meyers(1992)(25) and Eslamian(2003),(26) but Sakuda(1976) reported a significant correlation between mandibular crowding and Sn-MeGo (mandibular plane angle) and mandibular body length.(11) Finally, it seems that, the reason of this low correlation between occlusion and skeletal structure, is the influence of other factors. With the explosion of discoveries in developmental biology and genomics in the past decade, the direct relevance has affected the understanding of development, growth and adaptation of craniofacial skeletal tissue. It is essential to identify and understanding the role of key intrinsic and extrinsic factors that influence gene expression and cell growth during the development of the craniofacial complex.(27,28,29) CONCLUSION 1. Individually, occlusal characteristics were poorly associated with individual measures of craniofacial morphology (14 per cent of the variance in overjet and 20 per cent of the variance in overbite could be explained by a single skeletal measure). 2. A linear combination of skeletal measures explained more variance in an occlusal variable (43 percent of the variance in overjet and 24 percent of the variance in overbite). Acknowlegdement We are grateful to Hamid Farhadi for his assistance to complete the manuscript and his documentation. REFERENCES 1. Moyers RE, Wainrigth RL: Skeletal Contributions to Occlusal development. In: McNamara JA: The biology of occlusal development. Ann Arbor, University of Michigan, Center for Human Growth and Development, 1977: 89-111. 2. Proffit WR, Fields HW: Contemporary Orthodontics. 3rd Ed. St Louis: The C.V. Mosby Co. 2000: 171. 3. Angle EH: Malocclusion of the teeth. 7th Ed. Philadelphia: White Mfg Co. 1907; 4. Hellman M: Open bite. Int J Orthod 1931; 17: 421-44. 5. Hepak FN: Cephalometric Appraisal of the open bite case. Angle Orthod 1984; 104 Downloaded from jds.sbmu.ac.ir at 10:54 +0430 on Friday May 5th 2017 Safavi et al. 34: 65-72. 6. Nahoum HI: Anterior open bite. A cephalometric analysis and suggested treatment procedures. Am J Orthod 1975; 65: 517-21. 7. Tsang WM, Cheung LK, Samman N: Cephalometric parameters affecting severity of anterior open bite. Int J Oral Maxillofac Surg 1997; 26: 321-326. 8. Karlsen AT: Craniofacial morphology in children with angle class II-1 malocclusion with and without deep bite. Angle Orthod 1994; 64: 437-446. 9. Beckmann SH, Kuitert RB, PrahlAndersen B, Segner D, The RP, Tuinzing DB: Alveolar and skeletal dimensions associated with overbite. Am J Orthod Dentofacial Orthop 1998; 113: 443-52. 10.Norderval K, Wisth PJ, Boe GE: Mandibular anterior crowding in relation to tooth size and craniofacial morphology. Scand J Dent Res 1975; 83: 267-74. 11.Sakuda M, Kuroda Y, Wada K, Matsumoto M: Changes in crowding of teeth during adolescence and their relation to growth of facial skeleton. Trans Eur Orthod Soc 1976; 93-104. 12.Leighton BC, Hunter WS: Relationship between lower arch spacing / crowding and facial height and depth. Am J Orthod 1982; 82: 418-25. 13.Craig CE: The skeletal patterns characteristic of Class I and Class II, Division I malocclusions in norma lateralis. Angle Orthod 1951; 21: 44-56. 14.Milacic M, Markovic M: A comparative occlusal and cephalometric study of dental and skeletal A-P relationships. Am J Orthod 1983; 10: 53-4. 15.McNamara JA Jr: Components of Class II malocclusion in children 8-10 years of age. Angle Orthod 1981; 50: 177-202. 16.Pancherz H, Zieber K, Hoyer B: Cephalometric characteristics of Class II division 1 and ClassII division 2 malocclusions: A comparative study in children. Angle Orthod 1997; 67: 111-120. 17.Keeling SD, Riolo ML, Martin RE: A multivariate approach to analyzing the relation between occlusion and craniofacial morphology. Am J Orthod Dentofac Orthop 1989; 95: 297-305. 18.Johnston LE: A comparative analysis of Class II treatment. In: Vig PS, Ribbens KA: Science and clinical judgment in orthodontics. Craniofacial Growth series Ann Arbor, University of Michigan, Center for Human Growth and Development, 1986. (Monograph 19). 19.Wylie WL: The assessment of anteroposterior dysplasia. Angle Orthod 1974; 17: 97-109. 20.Riolo ML, Moyers RE, NcNamara JA, Hunter WS: An atlas of craniofacial growth, Craniofacil growth series. Ann Arbor: University of Michigan, Center for Human Growth and Development, 1979. 2nd Print, (Monograph 2). 21.Solow B: The pattern of craniofacial association. Acta Odontol Scand 1966; 24: 1-174. 22.Bjork A: The face in profile. Lund, Sweden: Berlingska Bok Trycheriet, 1947. 23.Schudy F: Vertical growth versus anteroposterior growth as related to function and treatment. Angle Orthod 1964; 34: 75-93. 24.Parlow RJ: A radiographic cephalometric appraisal of the proportional relationship of the molar and incisor heights in hypodivergent, hyperdivergent and normal patients. Am J Orthod 1972; 61: 309-10. 25.Meyers DM: A multivariate analysis of the relations between craniofacial structure and occlusion with Di Paolo’s quadrilateral measures. Am J Orthod Dentofac Orthop 1992; 102: 52-61. 26.Eslamian L, Arabzadeh Kashani M: The association between lower incisor crowding and Jarabak Index. Beheshti Univ Dent J 2003; 20: 14-19. 27.Thesleff I: Homeobox genes and growth factors in regulation of craniofacial and tooth morphogenesis. Acta Odont Sc 1995; 53: 129-34. 28.Richman J, Mitchell PJ: Craniofacial development: knockout mice take one on the chin. Curr Biol 1996; 6: 364-7. 105 Beheshti Univ Dent J 2005; 22(Special Issue): 100-106 identity of avian facial prominence. Nature 2002; 41: 909-12. Downloaded from jds.sbmu.ac.ir at 10:54 +0430 on Friday May 5th 2017 29.Lee SH, Fu KK, Hui JN, Richman JM: Noggin and retinoic acid transform the 106