Survey
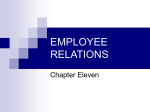
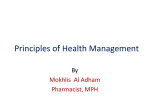
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Pain management Dr Malith Kumarasinghe MBBS (Colombo) Pain management Definition pain is an, unpleasant sensory and emotional experience associated with actual or potential tissue damage According to Katz and Melzack, pain is a personal and subjective experience that can only be felt by the sufferer. According to McCaffery pain is whatever the experiencing person says it is and exists whenever they say it does. PAIN PHYSIOLOGY Process of pain physiology nociceptor TRANSDUCTION TRANSMISSION PERCEPTION MODULATION Pain physiology contd.. Pain stimuli is converted to electrical energy. This electrical energy is known as Transduction. This stimulus sends an impulse across a peripheral nerve fiber (nociceptor). Pain physiology contd.. Transmission: A delta fibers (myelinated) send sharp, localized and distinct sensations. C fibers (unmyelinated) relay impulses that are poorly localized, burning and persistent pain. Pain stimuli travel- spinothalamic tracts. Pain physiology contd.. Perception: Person is aware of pain – somatosensory cortex identifies the location and intensity of pain Person unfolds a complex reactionphysiological and behavioral responses is perceived. Physiology contd.. Modulation: Inhibitory neurotransmitters like endogenous opioids work to hinder the pain transmission. This inhibition of the pain impulse is known as modulation Neurophysiology of pain (excitatory) Bradykinin- most potent pain producing chemical Prostaglandins- increase sensitivity to pain experience . Is a potent vasodilator and increase the production of bradykinin resulting edema Neurophysiology contd.. Substance P- transmits pain impulses to brain centers and causes vasodilatation and edema Serotonin- causes pain by altering sodium flow—neuron to fire Histamine,Leukotrienes and nerve growth factor are released Neuromodulators (inhibitory) Endorphins& dynorphins- morphine like substances. Located in the brain, spinalcord&GIT Produce analgesia when attached with opiate receptors in the brain Effects of pain Sympathetic responses Pallor Increased blood pressure Increased pulse Increased respiration Skeletal muscle tension Diaphoresis Effects of pain Parasympathetic responses Decreased blood pressure Decreased pulse Nausea & vomiting Weakness Pallor Loss of consciousness Behavioral characteristics Facial expressions- grimace, clenched teeth, wrinkled forehead, crying Body movements -restlessness, immobilization, muscle tension, protective movement of body parts Social interaction- avoidance of conversation & contacts TYPES OF PAIN ACUTE PAIN CHRONIC PAIN CUTANEOUS PAIN DEEP SOMATIC PAIN VISCERAL PAIN REFERRED PAIN NEUROPATHIC PAIN PHANTOM PAIN FACTORS INFLUENCING PAIN PHYSIOLOGICAL SOCIAL SPIRITUAL PSYCHOLOGICAL CULTURAL PAIN ASSESSMENT PAIN RATING SCALES- NRS, VAS,VAT,FACES RATING SCALE, PAIN-0-METER McGill PAIN QUESTIONNAIRE BODY MAP ABCDE for pain assessment &management Ask about pain regularly Believe the patient and family in their reports &what relieves it Choose pain control options appropriate for the patient Deliver interventions timely, logical &coordinated fashion Empower patient and their families JCAHO Standards for postoperative pain management are: Recognize patients’ rights to appropriate assessment and management of pain Screen for pain and assess the nature and intensity of pain in all patients Record assessment results in a way that allows regular reassessment and follow-up Determine and ensure that staff are competent in assessing and managing pain. Address pain assessment and management when orienting new clinical staff Standards Contd.. Establish policies and procedures that support appropriate prescribing of pain medications Ensure that pain doesn’t interfere with a patient’s participation in rehabilitation Educate patients and their families about effective pain management PRICIPLES OF PHARMACEUTICAL PAIN MANAGEMENT Provide medication in adequate doses. Utilize a preventive approach to pain relief. Use round the clock dosing with rescue medication available. Closely assess clients with particular diligence with first doses or when medication dose or the type is changed Combinations of analgesics may be more effective than those given singularly. PRINCIPLES CONTD. Understand and be prepared to treat side effects of medications avoidance of non-life threatening side effects (such as constipation, nausea, pruritis) more important that providing pain relief. These concomitant conditions are easily treated. Additions of adjuvant medications enhance pain relief. Principles contd. Believe the patient’s report of pain. Maintain a therapeutic relationship that facilitates mutual trust. Do not use placebos for pain. incorporate the goal of total pain relief into the pain management regimen operate as a team to provide the most effective pain relief outcomes PRINCIPLES CONTD. Asking for pain medication reflects the need for pain relief in 99.9% of people with pain and doses does not reflect an addictive personality. Recognize that respiratory depression is a rare occurrence, occurring most commonly among clients who are over sedated. Respiratory depression rarely occurs after the first few doses of an opioid. Principles contd. Only the patient and no one else can determine the amount of pain experienced There are no objective indicators that can be observed by another Pain management Medications to control pain (Pharmacological) Anesthetic agents Analgesic agents NSAIDs Anesthetic agents Local Anesthetics Lidocaine Bupivacaine Ketamine Analgesics Opioid Analgesics Fentanyl Morphine Codeine Demerol (Meperidine) Benzodiazepines Commonly used drugs Inj.Morphine(50mg) & Inj.Lorazepam(16mg) in 37 ml of 5% dextrose@ 4-8ml/hr Inj.Medazolam2mg/hr If agitated -Halopperidol Patient receiving Epidural Analgesia Epidural Analgesia syringe Patient Controlled Analgesia (PCA) Analgesics contd.. Non-Opioid Analgesics Paracetamol Aspirin NSAIDs- ketorolac Celecoxib Brufen WHO Analgesic Ladder NSAIDs NSAID Management contd.. Non-pharmacological interventions Massage Diversion therapy Relaxation therapy TENS Heat & cold applications Yoga Management contd… Meditation Humor Touch Magnets Magnets Yoga Meditation Humor Conclusion Patient’s pain report should be considered Assessment of pain should be regularly carried out and managed promptly Intervention of pain relief should be individualized Not to postpone pain relief but to consider Inter-disciplinary team approach