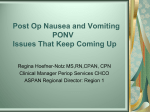
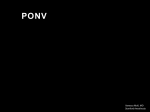
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
KETOBEMIDONE OR MORPHINE? Are they equivalent in terms of postoperative nausea and vomiting, mean amount of drug used and patient satisfaction with pain relief postoperatively? FÖRFATTARE Ulrika Parker KURS Omvårdnad – Självständigt arbete II VEA010 OMFATTNING 10 p HANDLEDARE Marianne Gustafsson EXAMINATOR Helle Wijk Sahlgrenska akademin VID GÖTEBORGS UNIVERSITET Institutionen för vårdvetenskap och hälsa Titel (svensk): Ketobemidon eller morfin? Är de likvärdiga för postoperativt illamående, medelmängd använd dos och patientens nöjdhet med smärtlindringen postoperativt? Titel (engelsk): Ketobemidone or morphine? Are they equivalent in terms of postoperative nausea and vomiting, mean amount of drug used and patient satisfaction with pain relief postoperatively? Arbetets art: Självständigt arbete I – fördjupningsnivå II Fristående kurs/kurskod: Omvårdnad – Självständigt arbete II VEA010 Arbetets omfattning: 10 poäng Sidantal: 8 sidor Författare: Ulrika Parker leg. sjuksköterska och arbetar på Kärnsjukhuset i Skövde e-post: [email protected] Handledare: Marianne Gustafsson Examinator: Helle Wijk ABSTRAKT Bakgrund Patient kontrollerad smärtlindring (PCA) är vanligt förekommande som smärtlindringsmetod efter en operation. Även om patienter som genomgår kirurgi rapporterats föredra smärta hellre än illamående, har mer tyngd lagts vid att minska patientens smärtupplevelse än deras PONV. Vi har jämfört två i Skandinavien vanliga läkemedel, morfin och ketobemidone, när det gäller postoperativt illamående (PONV), medelmängd använd dos, patientens nöjdhet med smärtlindringen och om det var några skillnader mellan kön och PONV. Metod En databas startades år 2000 där man registrerade PCA och bl.a. förekomsten av PONV, nöjdhet med smärtlindringsmetoden, kön och mängd använt läkemedel. Mellan April 2000 och November 2004 registrerades 2975 poster. Av dessa gick det att använda 1583. Vilket läkemedel som användes valdes slumpmässigt av ansvarig narkosläkare. Bortfallet analyserades stickprovsmässigt och beslöts också vara slumpmässigt. Resultat Det visade sig att morfin gav mindre illamående än ketobemidone. Patienterna var lika nöjda med smärtlindringen i båda grupperna och det var ingen skillnad i medelmängd använd dos. Andel kvinnor med PONV var 36,2% och 21,2% för män. Diskussion PONV är ett relativt stort postoperativt problem och resultatet från studien pekar mot att vi kan rekommendera att använda morfin i stället för ketobemidone i PCA för att minska patientens upplevelse av PONV. Key words: PCA, PONV, ketobemidone, morfin, välmående, biverkan ABSTRACT Background: Patient Controlled Analgesia (PCA) is widely used for pain management after surgery. We have compared two commonly used opioids in Scandinavia, morphine and ketobemidone, in terms of postoperative nausea and vomiting (PONV), mean amount of drug used, patient satisfaction with pain relief and if there was any differences for gender and PONV. Although surgical patients report preferring pain to nausea, more emphasis has been on decreasing patient’s pain experience than their PONV. Method: A database was set up to register post operative nausea and vomiting (PONV), satisfaction with the method, gender and amount of drug used. There were 2975 patients registered between April 2000 and November 2004. Out of these there were 1583 possible posts to use. The drugs were chosen at random by the anesthesiologist on duty. The missing data was analyzed and also found to be by chance. Results: The results showed that morphine gave less nausea than ketobemidone although patient satisfaction with pain relief was equal in both groups and there was no difference in the mean amount of drug used. The PONV rate for women was 36,2% and for men 21,2%. Conclusion: PONV is a relatively major problem postoperatively and the result from the present study indicates that we can recommend using morphine over ketobemidone in PCA for the PONV rate to be lower. Keywords: PCA, PONV, ketobemidone, morphine, well-being, side effects Content Background............................................................................................................... 1 Symptoms related to well-being ............................................................................................. 1 Postoperative Nausea and Vomiting ( PONV ) ...................................................................... 1 Pain ......................................................................................................................................... 1 Analgesia................................................................................................................................. 1 Satisfaction with pain relief .................................................................................................... 2 Patient wellbeing after ketobemidone versus morphine ......................................................... 2 Theoretical reference .............................................................................................................. 3 Ethical viewpoint .................................................................................................................... 3 Aim............................................................................................................................. 3 Method....................................................................................................................... 3 Setting ..................................................................................................................................... 3 Subjects ................................................................................................................................... 3 The PCA process..................................................................................................................... 3 Follow up ................................................................................................................................ 4 Drug selection criteria............................................................................................................. 4 Instruments.............................................................................................................................. 4 Analysis................................................................................................................................... 4 Missing data ............................................................................................................................ 4 Results....................................................................................................................... 5 The PONV rates for the two drugs ......................................................................................... 5 Discussion ................................................................................................................ 6 Method discussion .................................................................................................................. 6 Result discussion..................................................................................................................... 7 Acknowledgments................................................................................................................... 8 References ................................................................................................................ 9 Appendix ..................................................................Fel! Bokmärket är inte definierat. Author Guidelines........................................................... Fel! Bokmärket är inte definierat. Background Symptoms related to well-being A major part of the work for the nurse in the post-surgical ward is helping patients to be relieved of symptoms like pain, nausea or other discomforts. Nausea can be caused by a multitude of factors such as gender, smoking habits, kind of surgery or choice of drugs used during surgery. Nausea is very much part of feeling comfortable or not. Nausea, sedation, apnea, constipation and urinary retention are also well known side effects of opioids (1). In order to relieve pain or nausea effectively the nurse needs to be following guidelines set up and keep up with new knowledge and research. Comfort is essential in giving good nursing care (2). Listening to the patient is considered as humanistic nursing involving interaction between the nurse and the patient (2). In order to give good nursing care the nurse needs to do all in her power to relieve the patient from different kinds of uncomfortable symptoms like nausea as well as pain. Postoperative Nausea and Vomiting ( PONV ) Due to a number of reasons such as site and length of surgery, choice of anesthesia, smoking habits, gender and motion sickness PONV van occur (3). Most surgical patients can accept postoperative pain to nausea and it may not always be perceived as a true medical problem. PONV is also likely to have economic impact on health care resources and also strongly affect patient satisfaction (4). Surgical patients have reported that the fear of suffering from PONV is worse than the fear of postoperative pain (5). It is therefore interesting to compare two different opioids commonly used postoperatively in terms of side effects like PONV. Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage (6). It is always subjective and what the experiencing person says it is (7). Pain is more than just suffering. It is linked to specific physiological responses that cascade to increase pain intensity and extent. Pain triggers stress related hormones that promote tissue breakdown, energy mobilization and fluid retention. This can lead to cardiovascular effects like tachycardia, hypertension, ischemia and ventricular arrhythmias. It can also lead to slowing down of peristalsis and immune impairment. Aggressive pain control is therefore physiologically valuable as well as improving patient satisfaction (8). Pain in itself can also cause nausea (9). Analgesia Analgesia can subdue unwanted responses and potentially improve overall patient outcome and shorten hospital stay (8). Strong opioids have been used for a long time in postoperative pain management. Opioids change the pain experience and increase the pain threshold (1). The analgesic effect is believed to be on different levels in the central nervous system; brain stem and spinal. Although new drugs have been developed, opioids are still superior and widely used for severe pain. About 30% of patients who have postoperative pain treatment with opiods will have nausea or will vomit. However, opioid-induced nausea and vomiting is, strictly speaking, not PONV (4). A certain technique for administering opioids postoperatively has been developed called patient controlled analgesia, (PCA). This means that the patient experiencing pain can press a button on a pump and through an intravenous line get a dose of selected opioid. Patient satisfaction is high since there is no waiting time 1 involved. The preset dose is administered immediately avoiding a call for the nurse to first come to the patient’s bed and then go away to administer the drug and come back. The nurse is free to concentrate on other tasks. Patients report that it is very satisfactory being able to control something in a situation where you do not have much control. The method is safe when following guidelines set up by anesthesiologists. Any opioid can be used in PCA (1). Drawbacks can be that the patient is left to a mechanical pump instead of a human hand giving the drug and can feel abandoned. One can also ask if the patient always push the button for the right reasons or for anxiety or other reasons? Satisfaction with pain relief It is always difficult to create numerical truths from a subjective phenomena like pain. Patient satisfaction with pain relief is highly subjective. The patient may also be unsatisfied for other reasons than poor pain relief and the instrument for pain evaluation may be misunderstood. The actual pain experience was mainly found to be in accordance with the pre-operative expectations and the validity of patient satisfaction as an optimal outcome variable in quality assurance processes of postoperative pain management may be questioned (10). Despite moderate to severe pain, patients were generally satisfied with their pain relief (11). There was no correlation between patient satisfaction with pain management and VAS pain scores in the emergency room (12). Other factors seemed to be important to satisfaction such as empathy and explanation. High levels of satisfaction with pain management was found despite pain still being experienced by patients (13). Three different ways of informing the patient was studied before receiving the PCA method of relieving pain. Seventyfive patients received a leaflet, 75 got an interview with a trained nurse from the pain team and 75 patients got the usual information. There were no benefits to any method as to pain relief experienced, worries about addiction and safety or knowledge about side effects (14). Patient wellbeing after ketobemidone versus morphine Earlier studies have shown differences between ketobemidone and morphine in relation to pain relief and side effects. Pre medication given to 227 women undergoing day surgery for abortion or DNC (dilation and curettage) was compared double blindly. The results showed 10 mg morphine plus 0,4 mg scopolamine was more sedating than 5 mg ketobemidone plus 25mg A29 (spasmolyticum) as well as giving more nausea and dryness of mouth. Ketobemidone had the same calming effect as morphine but patients woke up earlier and experienced more pain. More patients in the ketobemidone group needed anti emetics (15). Another double blind study compared ketobemidone with morphine in 309 patients with chest pain. They found that 5 mg ketobemidone was equipotent with 10 mg morphine. The ketobemidone group had a significant increase of patients who were completely pain free 15 and 30 minutes after the medicine was given compared to morphine. Approximately 15 % in both groups experienced nausea and 7 % had vomiting. No other differences were found (16). Another double blind study with 81 patients going through open heart surgery found no differences between ketobemidone, meperidine and morphine comparing the effect of pain relief, shivering or PONV (17). A study with 54 children concluded that ketobemidone had the same analgesic potency and similar adverse effects as morphine (18). These earlier studies have been prospective and not unanimous. It was therefore interesting to investigate if any differences could be found in a large material and to compare two different opioids commonly used postoperatively in terms of side effects like PONV. 2 Theoretical reference The theoretical model used in this study is based on Watson´s theory of nursing care (19). According to her, specific methods, use of technical gear or outcome measures of treatment is not similar to the core of nursing care characterized by the relationship between the nurse and the patient. Important factors in the core of caring are what bring positive health results independent of the situation. Caring sciences and medical sciences compliment each other and the nurse needs to integrate knowledge about physiology with knowledge about human behavior in order to develop and promote health as well as to help sick people. Ethical viewpoint The study followed guidelines according to the Helsinki declaration and Swedish law for the use of databases (20). Aim The aim of the present study was to compare ketobemidone and morphine in PCA in terms of postoperative nausea and vomiting (PONV), mean amount of drug used, patient satisfaction with pain relief and if there was a difference for gender and PONV. Method This study was a descriptive, comparing and retrospective study. Setting This study was done in a 550 bed general hospital in Sweden with approximately 12.000 operations done yearly. A database was started in the year 2000 to register patients receiving PCA as a part of their postoperative pain management. The register was set up to follow Swedish laws and regulations for computerized personal data files. Clinics included were general surgery, gynecology, orthopedic and pediatric. Subjects During 4½ years 2975 patients were registered to be included in the present study (April 2000 - Nov.2004). Of these, 1583 (53 %) of all registered patients receiving PCA had all information needed to be included in the study such as satisfaction rate, stopping date, amount of drug used and PONV. The patient did not have to be fluent in Swedish to be offered a PCA but they had to be able to understand the method when explained. The sample consisted of 579 orthopedic patients, 159 general and urology patients, 450 gynecology patients and 395 unspecified. Diagnoses involved were hysterectomy, laparatomy, hip or knee replacement, spinal surgery, trauma, prostathectomy, nephrectomy among others. Patient age ranged from 8-96 years. Out of 1583 patients there were 1045 women and 538 men. 35 children (< 18 years old) participated. They were informed about the PCA method together with their parent or guardian. The PCA process Patients were offered this method when major surgery was planned and an epidural pain relief was not in use. For minor surgery it was not offered. The data base registered patients name, birth date, drug, concentration of drug, diagnosis, clinic, starting date, stopping date, patient 3 satisfactory rate, amount of drug used, side effects such as nausea, vomiting and urinary retention. The anesthesiologist in charge registered data directly in the computer and printed a paper copy. That paper copy was signed by the anesthesiologist and considered a legal document to follow the patient chart. The selection of drug was equally divided between the genders. Women had 64,6 % ketobemidone and 63,4 % morphine in their PCA. Men had 35,4 % ketobemidone and 36,6 % morphine. Amount of drug used ranged from 2-924 mg. Time span for the PCA being used ranged from 1-21 days with the most common it being used 2-3 days. Follow up When the PCA was discontinued the nurse in charge asked the patient to rate satisfaction with pain relief, nausea, vomiting and urinary retention. Amount of drug used and date of discontinuation was to be filled in by the nurse. If the patient was unable to do the recording the nurse could do it by asking the patient and filling in the information for him or her. A copy was then made and given to the postoperative pain nurse who registered the data collected into the database. The drugs used for PCA were ketobemidone and morphine. The concentration of both drugs was 1 mg/ml and the pre-set dose 1 mg. The concentration and dose was possible to adjust according to the patient weight. Which of the two drugs to be chosen was up to the doctor in charge. Drug selection criteria A questionnaire was sent to the doctors on staff asking them how they chose between morphine and ketobemidone. Of the 17 questionnaires sent out, 16 were returned. Four said they chose at random, six said they chose ketobemidone unless there was a reason to avoid it such as; gynecological surgery, C-section, nausea from ketobemidone or objections to it. Four said morphine was their first choice and one said he checks with the nurse what she prefers. One said whatever the staff is most confident with will be the choice. It was therefore concluded that the drugs were chosen by chance. Instruments Patient satisfaction with pain relief was measured with a visual analog scale (21). This method was chosen as a simple and easily understood method of assesing to which degree a person agrees with something. The 100-millimeter line had anchors at both ends. One anchor was the word “worst” and the other anchor was the word “best”. The patient was instructed to define his or her satisfaction with the pain relief by making a mark somewhere along the line. PONV was measured with a yes or no question. Analysis Chi2 test was used for PONV. Proportions from two independent samples with normal distribution samples were tested. T test was used for comparing mean amount of drug used and patient satisfaction with pain relief. The two groups were a normal distribution sample. Missing data The amount of missing data had many reasons. Not all ordered treatments were started and the record never made it back to the pain team to be registered in the database. Sometimes patients got registered for a PCA as a security back-up in case the epidural was not enough but the PCA was neither used nor discontinued in the data base. Some nurses’ stations did not have easy access to a photocopier and therefore the record never made it back to be registered. Three groups of the missing data was analyzed to verify that it was also by chance it was 4 missing, see table 1. The data was missing because not all information was filled in like satisfaction with pain relief or PONV. The missing data was not further analyzed though it was considered all being by chance. Table 1. Missing data for gallbladder, unspecified gynecology and hip surgery. Total: Amount drug filled in: Gallbladder, n=23 ketobemidone morphine 23 0 10 Gynecology n=114 ketobemidone morphine 65 49 37 27 Hip, n=368 ketobemidone morphine 153 215 Stop date filled in: Missing: 56% 36 27 45% 45% 100 124 35% 42% Results The PONV rates for the two drugs Ketobemidone was given to 1015 patients. Of these 333 filled in experienced PONV. Morphine was given to 568 patients and 159 filled in experienced PONV. In the total group (n:1583) 492 patients experienced PONV ( figure 1). 1200 1091 PONV 1000 Number No PONV 800 682 600 400 409 333 492 159 200 0 Ketobemidone Morphine Total Figure 1 shows the number of patients experiencing PONV for ketobemidone, morphine and the total group of patients. The PONV rate was about 33 % for the patients who got ketobemidone, 28 % for the patients who received morphine and 31 % for the total group of patients. P-value was 0,04 and it was statistically correct to state that morphine gave less nausea and vomiting compared to ketobemidone (figure 2). 5 100,0% 90,0% % PONV % No PONV 80,0% Percent 72,0% 67,2% 70,0% 68,9% 60,0% 50,0% 40,0% 32,8% 30,0% 28,0% 31,1% 20,0% 10,0% 0,0% Ketobemidone Morphine Total Figure 2 shows the PONV rate for the patients who got ketobemidone, morphine and for the total group of patients. The mean amount of drug used The mean amount of drug used was similar in both groups. Ketobemidone had a mean amount of drug used of 51,6 mg with a span of 2-924 mg (SD 65,7). Morphine had a mean amount of 54,0 mg with a span of 2-681mg (SD 67,3). The difference in experienced PONV could therefore not be explained with a major difference of amount of drug used, (p = 0,77). Patient satisfaction with pain relief for the two drugs Patient satisfaction was rated 72,3 mm (SD 22,8) as a mean for ketobemidone and 73,3 mm (SD 21,4) for morphine. There was no statistical difference (p = 0,37) between the two drugs which means that the patients were equally satisfied with the two drugs used. The difference in gender and PONV The PONV rate for women was 36,2 % and for men 21,2 %. Discussion Method discussion One of the strengths of this study was the large number of participants. What was known before on this subject was done on smaller materials and not consistent. The two groups compared in this study were different sized due to a treatment tradition in the hospital studied. The drug of choice had been ketobemidone for other postoperative pain management than PCA and that trend followed when PCA was started. Ketobemidone was believed to give less nausea and be more potent than morphine and therefore more used. Some documents never got back and couldn´t be registered in the database. Lack of time or copiers was blamed in the beginning. Nurses’ negligence sometimes played a role as well as patients refusal to cooperate. Sometimes only some of the information asked for was 6 recorded. All nurses’ stations have since been equipped with copiers and nurses given repeated information on the importance of sending the data back for registration and the compliance rate has become better. Spasmolyticum is no longer used in pre medication in the hospital studied. That sort of drug could have been guilty of some of the side effects in earlier studies. They are still used in the form of atropine during surgery to reduce secretion and raise pulse rate. To have different concentrations of two drugs to be compared can be questionable. Another result could have emerged had one used the same concentration in Wolff´s (1988) and Raeder´s (1986) studies. A nursing action like approaching a patient’s bed and giving a drug intravenously affects the outcome of the treatment. The placebo effect is well known and amounts for as much as 25-60 % (22). To be totally fair to the two drugs compared you therefore need to use the same concentration. Result discussion In line with Watson´s nursing model the results of this study can be implemented in our daily work of alleviating postoperative patients of their pain and PONV. As a nurse in the postoperative care unit you constantly evaluate patients symptoms and their origin. The patient is often still sedated and usually experiences difficulty defining their symptoms. In this setting it is essential to integrate knowledge about physiology with knowledge about human behavior. Although PONV is less in the morphine group the satisfaction with pain relief is equal in both groups. This result is contradictory but has been shown before (10). It has been found that more than 75 % of patients were satisfied or very satisfied with their overall pain management, despite almost half of all patients reported recent moderate to severe pain. Predictors of patients´ satisfaction with how their primary doctor managed their pain were whether or not the patient was told that treating pain was an important goal (23). According to nursing this is very important knowledge since the nurse is the one closest to the patient. The nurse is responsible for pain assessment as well as of outcomes of pain treatment in the patients. One nursing intervention can therefore be to inform the patient about the importance of pain relief for their experience of well being. Patients are generally very satisfied with the PCA method and this study confirmed that. The PCA method gives the patient control of something in a situation they have little control over. Even though the patient was deciding when to use the PCA, the nurse is still assessing the patients’ pain experience and continuously evaluating the treatment. The nurse needs to be aware of that the postoperative pain itself can be a major cause of PONV (9). Although patients report fearing PONV more than pain, PONV has long been seen as a minor problem compared to the more major problem of pain. It is a known fact that opioids cause approximately 30% of a population to experience nausea. In the present study we have shown that if you treated 20 patients with PCA one less person would be nauseous if you chose morphine over ketobemidone. We need to approach the problem of PONV more seriously and take steps to address it. If our concern is pain relief, one of our major aims should be preventing and treating PONV. 7 One way of approaching the problem with nausea is using those drugs pre-, peri- and postoperatively that we know gives less nausea than others. Since we now have a good knowledge about who is at risk of developing nausea it is a professional duty to identify them and be proactive in their treatments. If we can influence a patient´s wellbeing by which kind of drug we choose there is reason to use that knowledge to the benefit for the patient. General information about the postoperative pain intensity and psychological training to reduce anxiety and depression has been suggested to improve satisfaction with the PCA method (24). To make sure that the patient uses the PCA for the right reasons is essential and adequate information about the method of utmost importance. If the patient uses the PCA for the wrong reason, like nausea, we can probably help some to alleviate their nausea by informing them about the right way to use it. One of the major tasks an acute pain services nurse has is to educate staff about pain relief and the right way to use the PCA method. Even though we were not able to show of any statistical difference in satisfaction between the two drugs there are reason to believe that the patient will be more satisfied the lesser PONV that is experienced. The difference in experienced PONV for the genders has been shown before (3). It is well known women experience more PONV compared to men and this study confirmed that. The team around the patient needs to be pro-active to avoid symptoms like pain and PONV through different medical and nursing actions. More research can be made in this area. Are there other differences between the drugs? Are there other newer drugs that can make the postoperative time more comfortable for the patient? Not much has changed since opioids started being used for severe pain but research and development are ongoing in this field and we need to keep trying to find better drugs with lesser side effects. Acknowledgments I would like to thank Marianne Gustafsson, Per Lorentzen, Helle Wijk, Anna-Lena Loft, Magnus Berndtson, Camilla Ylikangas, Susan Lindberg, Berith Wennström, Anita Jonsson, Tommy Jonsson and Heléne Lindqvist for all their help finishing this study. I would also like to thank Mary-Ann Liivrand and Eva Öfverman for support and resources and Skaraborgsinstitutet for financial support. 8 References 1. Rawal, N. (1999). Postoperativ smärta. Lund: Studentlitteratur. Postoperative pain 2. Paterson, J. G., & Zderad, L. T. (1988). Humanistic Nursing. New York. National League for Nursing. 3. Watcha, M.F. (2002). Postoperative nausea and emesis. Anesthesiology Clinics of North America, 20(2002), 709-722. 4. Tramèr, M. (2004). Strategies for postoperative nausea and vomiting. Best Practice & Research Clinical Anaesthesiology, 18(4), 693-701. 5. Van Wijk, M.G.F., & Smalhout, B.A. (1990). Postoperative analysis of the patient´s view of anasthesia. Anaesthesia, 45, 679-682. 6. IASP (International Association for the Study of Pain). (1979) List of definitions and notes on usage. Pain, 6, 249-252. 7. McCaffery, M., & Bebee, A. (1989). Pain: Clinical Manual for Nursing Practice. St.Louis: Mosby. 8. Carr, D. (1993). Clinical Updates, Pain Control: The New “Whys” and “Hows”. Pain, May 1(1). 9. Andersen, R., Krogh, K., (1976). Pain is a major cause of postoperative nausea. Can.Anaesthetists Society Journal, 23, 366-369. 10. Svensson, I., Sjostrom, B., Haljamae, H. (2001). Influence of expectations and actual pain experiences on satisfaction with postoperative pain management. Eur J Pain, 5(2), 125-33. 11. Carroll, K.C., Atkins, P.J., Herald, G.R., Mlcek, C.A., Shively, M., Clopton, P., & Glaser, D.N. ( 1999). Pain assesment and management in critically ill postoperative and trauma patients: a multi site study. Am.J.Crit.Care, Mar; 8(2):105-17. 12. Kelly, A-M. (2000). Patient satisfaction with pain management does not correlate with initial or discharge VAS pain score, verbal pain rating at discharge, or change in VAS score in the emergency department. The journal of Emergency Medicine, 19(2), 113-16. 13. Ward, S., Gordon, D. (1994). Application of the American Pain Society quality assurance standard. Pain, 56:299-306. 14. Chumbley, G.M., Ward, L., Hall, G.M., & Salmon, P. (2004). Pre-operative information and patient-controlled analgesia: much ado about nothing. Anaesthesia, Apr; 59(4): 354-8. 15. Raeder, J.C., van der Linden, J., & Breivik, H. (1986). Premedication for day case surgery: a double blind comparison of ketobemidone+ dimethylaminodiphenylbuten (A29) and morphine+ scopolamine. Acta Anaesthesiologica Scandinavica, Oct 30(7), 502-6. 9 16. Wolff,T., Leward, S., Hagman, A., Andersson, M., Larsson, L., & Elgen, K. (1988). Analgesic treatment in acute myocardial infarction. A double blind comparison of ketobemidone+ the spasmolyticum A29 (Ketogan) and morphine. Acta Medica Scandinavica, 223(5), 423-30. 17. Ohqvist, G., Hallin, R., Gelinder, S., Lang, H.,& Samuelson, S. (1991). A comparison between morphine, meperidine and ketobemidone in continous intravenous infusion for postoperative relief. Acta Anaesthesiologica Scandinavica, Jan 35(1), 44-8. 18. Jylli, L., Lundeberg, S., Langius-Eklöf, A.,& Olsson, G.L. (2004). Comparison of the analgesic efficacy of ketobemidone and morphine for management of postoperative pain in children: a randomized, controlled study. Acta Anaestesiologica Scandinavica, July, 48, 12569. 19. Watson, J. (1979). Nursing: The Philosophy and Science of Caring. Boston: Little & Brown. 20. www.codex.vr.se 21. Huskisson, E.C. (1983). Pain Measurement and Assessment. Edited by Melzack, R. New York: Raven Press. 22. Quitkin, F. M. (1999). Placebos, Drug effects, and Study design: A Clinician´s Guide. Am J of Psychiatry, 156(6), 829-836. 23. Dawson, R., Spross, J.A., Jablonski, E.S., Hoyer, D.R., Sellers, D.E., & Solomon, M.Z. (2002). Probing the paradox of patients´ satisfaction with inadequate pain management. Journal of Pain and Symptom management, March, 23(3), 211-220. 24. Breme, K., Altmeppen, J., & Taeger, K,. (2000). Patient controlled analgesia: Psychological predictors of pain experience, analgesic consumption and satisfaction, Schmerz, 14(3), 137-45. 10