Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
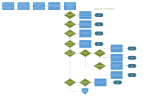
Pediatric Disaster Life Support ©) (PDLS : Scene Assessment, Triage, Resuscitation and Stabilization at the Scene of a Disaster James Courtney, DO Triage Assessment, Stabilization, Resuscitation Learning Objective At the end of this lecture, the students should be able to: - describe differences in triage decision making for - children describe triage categories describe field triage assessment describe principles of field triage, stabilization and resuscitation describe initial field stabilization methods for children describe organization of field triage, treatment, staging, and clearing/transportation for children General Principles of Disaster Care Scene Assessment Triage Assessment Initial Stabilization Resuscitation Scene Assessment Ensure scene safety Establish that disaster exists Estimate number of victims: adults/children Scene Assessment Notification to medical control: regional communications, local emergency management / disaster authority - type of event - initial casualty estimate Make initial request for additional resources Then begin triage assessment of individual patients Triage Assessment Derived from the French “trier” meaning to sort, it describes a medical decision making process Guides decisions about allocating scarce resources and limited time “greatest good for greatest number” Protocol helps makes decisions Appropriate performance crucial Triage ICS separates triage from treatment immediately - see everybody once briefly for overview Dynamic process, re-triage / re-evaluate at several stages Triage in disaster setting may be very difficult Pediatric population unique challenge Initial Brief Assessment Open airway Control major hemorrhage Categorize Triage Classifications Simple Triage And Rapid Treatment S.T.A.R.T. JumpSTART Tool for Rapid Pediatric Multicasualty Field Triage (children from 1 - 8 years of age) Triage Categories Red / Immediate / Emergent Yellow / Urgent Green / Non-Urgent / Walking Wounded Black / Deceased or soon to be Triage Classifications and Examples Red - tension pneumothorax, rib fractures, upper airway obstruction, hemorrhage, femur fracture, asthmatic Yellow - humerus fracture, scalp lacerations, shoulder dislocation Green - ankle sprain, simple laceration, orphaned child, subluxed radial head Black/Blue - cardiopulmonary arrest, severe open head injury START Most commonly used triage system across country Not applicable for under 8 years old Initial eval – not final Time limited (plan <1 min/patient) Categorize and move on START “If you can hear me and are able, walk over here” GREEN triage done – still need individual evaluation, but can await more staff, allows initial rescuers to focus on more severely injured people. Gen 80% of victims will be green, self extricate (may self transport – eases burden on field but hard on hospitals) START EVAL (and tag) those unable to walk for transport: RPM Resp: no => open airway= still no then reposition airway = still no =>BLACK if yes => RED (immediate). Spont resp >30 => RED/ under 30 => next item of assessment START Perfusion: cap refill > 2 sec => control bleeding, label RED; <2 sec, next item Perfusion: Radial Pulse => if no label RED; if yes then next item Mental status: Cannot follow simple commands => RED; CAN follow simple commands (and has cap refill < 2 sec and spont resp < 30) => YELLOW (delayed) START As soon as one can categorize a patient, STOP evaluating (if they are RED for breathing, they won’t be seen any faster for additional problems) and move on. Minimal treatment during triage: airway maneuver (chin tilt, jaw thrust) and dress active blood loss (not scrapes). Pediatric Triage Pediatric Triage Triage of children and adults is typically done simultaneously during a disaster It is important to remember that although the injury process may be the same, a child’s vulnerability to that injury may be very different - Specifically, their response to airway obstruction Pediatric Triage The standard adult triage tools do not take into account the specific vulnerability that children have to dying from airway obstruction Children may have a reversible period of respiratory arrest from which they may recover if treated promptly Pediatric Triage Due to this, a specific pediatric triage tool was developed and tested - JumpSTART Builds from the concepts of triage taught in START triage, which is commonly utilized Confused? If you remember the specific vulnerability children have to airway compromise, this makes sense The “Jumpstart” term refers to the extra chance we give a child to breathe before we declare them a BLACK TAG JumpSTART (under 8) Kids more airway dependent – rescue breaths attempted if pulse present (unlike adults) Resp 15-45 instead of <30 Vascular system clamps down sooner, so cap refill less reliable. Use peripheral pulse instead. Mental status AVPU instead of following simple commands JumpSTART “If you can hear me and you are able, walk over here for help.” Probably won’t work for children If they are ambulatory, then they are GREEN Use adults on scene to help corral the GREEN children JumpSTART Respirations: NO open airway => yes RED; no -> check peripheral pulse. NO pulse = BLACK Pulse 15 sec mask to mouth ventilation Spont resp: NO BLACK; YES RED JumpSTART Breathing: RR <15, >40 or irregular =RED RR 15-40, regular – check pulse No peripheral pulse: RED Peripheral pulse: check mental status AV (appropriate) YELLOW PU (inappropriate) RED Kids in triage Don’t follow commands. May actually hide from rescuers May be extricated by GREEN parents/ adults with delay in triage and treatment. Need distraction and dedicated supervisor able to run after wandering toddlers Examples Awake 8 yr old child brought in 3 days after earthquake with 20 others Can not walk Responds to voice Respiratory Rate 50 IMMEDIATE No obvious injuries Examples Unconscious 4 year old hit in head by debris moments ago In a room full of injured children Not breathing Obvious head injury Examples What do you do? How do you classify this child if he breathes? IMMEDIATE How do you classify this child if he does not breathe after 5 rescue breaths? DECEASED Examples You are receiving multiple casualties on a hospital ship Young child found breathing but sleepy Brought in by military helicopter with IV running Examples What do you want to assess? Respiratory Rate 30 Has a palpable pulse Arouses to touch and loud voice DELAYED Categorize the Following 1. 7 y.o. female, crying, unwilling to move right arm, 1° burn to anterior thigh GREEN 2. 10 y.o. male, deformed thigh, pale, pulse 120, BP 30/40, RR 30 RED 3. 20 y.o. female, apneic, severe head injury with visible grey matter BLACK 4. 2 y.o. male, 2-3° burns to face, neck and chest RED 5. 5 day old infant, found on ground, appears unharmed YELLOW Pediatric Triage Focus on integration of children in to the triage system Once a child is classified as a color, quickly move them to a treatment area in order of severity - RED first, then YELLOW, then GREEN Preplanning Needs assessment of community Commitment on part of institutions and key personnel to treating injured children Consider children with special needs Consider evacuation process for NICU/PICU/SCU for newborns Lack of supervision Decontamination Decontamination of Children Special issues must be accounted for before undertaking decontamination of children Advance planning will make the difference Goal is to integrate care of children with that of the general population Decontamination of Children Parents - After a disaster or major emergency, most parents will not separate from their children - Decontamination patient flow must account for this - Takes longer than expected to decontaminate parent and child Decontamination of Children Temperature Extremes - Decontamination water must not be ice cold for young children Risk of hypothermia, especially in winter Children must be covered immediately - Risk of injury if too hot or chemicals used Do not use bleach in decon water Do not use rough scrubbing devices Decontamination of Children Special Equipment - Have a plan for special equipment on children or adults Wheelchairs Electronic equipment Firearms Decontamination of Children Special Issues - How long does it take a child to take a shower or bath normally? - Children may not be cooperative - Children will likely be frightened with protective suits - How do you track a non-verbal, naked child after decontamination? Child Likely To Need Specialized Care Shock SBP <80, HR>130<50 Resp distress RR>30<10, stridor GCS<9 Mechanism - MVA - Pedestrian/bicyclist thrown >15 feet - Penetrating injury to head, neck, trunk Child Likely To Need Specialized Care Specific injuries skull fracture pneumothorax, flail chest abd trauma with peritoneal signs amputation / degloving vascular injury burn with inhalation FB aspiration / ingestion Progression of Pediatric Shock Response to Shock Vascular resistance Percent of control 140 100 60 20 Cardiac output Compensated shock Blood pressure Decompensated shock Pediatric Assessment Triangle Pediatric Resuscitation Russian Field Hospital Nias, Indonesia 4/05 Treatment Patients frequently may outnumber transport, leading to time in field where treatment can be started Sort patients by category (GREEN, YELLOW, RED and BLACK) and treat within areas. If GREEN patients self triaged, they need evaluation. Limited initial treatment – don’t delay evacuation if vehicle available Treatment Kids will be mixed in – do you have enough supplies in kid size (oxygen, IVs, splints)? Does your locality stock a “disaster truck”? Does it have kid size equipment and kid sized doses of Hazmat antidotes? Do you have Broselow tapes to guide dosing? Field Stabilization Airway - chin lift, jaw thrust, oro- or nasopharyngeal airway Breathing - supplemental O2 as available - limited resources for mechanical/manual ventilation Circulation - hemorrhage control - direct pressure, dressings (rotating tourniquets) - limited resources for IVF Fracture Stabilization - using resources available Field Stabilization There is little role for initiation of CPR in disaster situations Consider on site organization of arriving personnel and arriving resources Consider establishment of clearing/staging until: - triage patients for treatment on site or transport to hospital/health care facility - efficient utilization of resources, personnel, and supplies Resuscitation/Stabilization Simple measures that do not require sophisticated equipment are most appropriate. Needs must be evaluated and balanced against available resources. The principle of “doing the greatest good for the greatest number”. Consider IV Access in the Following: Time to definitive care 30-60 minutes Prolonged extrication / entrapment Dehydration > 15% Multiple fractures Scalp lacerations with significant blood loss IV Access Attempt peripheral access if unsuccessful in <90 sec. consider IO. Estimated body weight in kg: (age in yrs x 2) + 10 Blood volume = 80 mls/kg x body weight Estimate blood loss: # pelvic ring = 10% total blood volume, # femur up to 20%. IO access sites - distal femur - proximal tibia - med/lat malleolus - iliac crests High success rate, up to 80% in less than one minute Treatment: Dressings – rinse gross dirt with sterile fluids or tap water if available, sterile cover to prevent further contamination Pressure dressing for active bleeding - Recruit neighbor to help hold pressure during triage while awaiting transport/evacuation Splint – extremity injuries Treatment Medications: pain control, specific antidotes with Hazmat event/team Monitoring: repeat assessment after triage, re-categorize if necessary (to worse, never better – they still have the same underlying injury) Further field care Depends on local plans Send personnel and supplies to site, or bring patients to hospital (personnel and supplies) - EMS –patient to hospital - NDMS – personnel and supplies to site Transport Decides which patients leave scene first and where they’re going Helpful bystanders and self transporters will fill the nearest hospitals first. Includes decisions about longer transport times for specialty care Use helicopters for long distance transports Children with Special Health Care Needs Children with Special Health Care Needs (CSHCN) Children with special medical or physical needs - Wheelchair or crutches - Learning disability - Vision, hearing, or language impaired - Technology dependent Ventilator Dialysis Children with Special Health Care Needs (CSHCN) Children with Special Health Care Needs (CSHCN) Prevalence of CSHCN Based on a national survey - 1 in 5 households self identify as having a CSHCN - Approximately 1 in 8 children are identified by parents as being CSHCN Care of these children must be integrated in to the care of all children during a disaster Special Challenges for CSHCN Sheltering - Controversy: Together or separately? - Controversy: Should CSHCN be considered medical patients if they are not injured or ill? Decontamination - What is the best way to decontaminate medical hardware such as a wheelchair? - How do we decontaminate technology, such as a ventilator? Special Challenges for CSHCN Transportation - Take equipment with or leave behind during evacuation? For all of these topics, special advance planning is required to be successful in taking care of all children Sheltering for Children Hurricane Katrina taught us many harsh lessons about how important shelter planning is Sheltering Issues Hygiene - Children pose a special risk to maintaining hygiene in a shelter operation - Basic supplies such as wipes and diapers frequently overlooked - Children are at a special risk of acquiring gastrointestinal and respiratory diseases - Children are exceptionally good at spreading these diseases - Must plan for handwashing/sanitizing Sheltering Issues Safety and Supervision - Shelters are dangerous environments - Rarely childproofed - Children move quickly throughout environment - Easy to get lost - Possible criminal element Sheltering Issues Health Maintenance - Clean water and healthy food a challenge - Children require something to do Consider a recreational therapy group - Children require more sleep Shelters are frequently loud - Pediatric Health Screening important Prevention of disease Maintaining primary care for extended stays Resources PDLS is a start Much information exists to guide the preparation and care for children in disasters Resources U.S. Center for Disease Control - www.cdc.gov National Center for Disaster Preparedness - http://www.ncdp.mailman.columbia.edu/ American Psychological Association - www.apa.org Resources JumpSTART Triage Tool - www.jumpstarttriage.org American Academy of Pediatrics - http://www.aap.org/terrorism/topics/disaster_planning.html Pediatric Disaster Preparedness Consensus Conference Summary - http://www.bt.cdc.gov/children/pdf/working/execsumm03.pdf U.S. Department of Homeland Security - www.dhs.gov Disclaimer The information herein should NOT be used as a substitute of an appropriately certified and licensed physician or health care provider. The information herein is provided for educational and informational purposes only and in no way should be considered as an offering of medical advice. The authors, editors, and publisher of this site have used reasonable efforts to provide up-to-date, accurate information that is within generally accepted medical standards at the time of production. However, as medical science is ever evolving, and human error is always possible, PDLS does not guarantee total accuracy or comprehensiveness of the information on this site, nor are they responsible for omissions, errors, or the results of using this information. The reader should confirm the accuracy of the information in this article from other sources. In particular, all drug doses, indications, and contraindications should be confirmed in package inserts. Course Directors PDLS 2.0 content revision- March 2006 - Andrew L. Garrett MD, FAAP - Richard V. Aghababian, MD, FACEP University of Massachusetts Medical School PDLS course- 1999 - Richard V. Aghababian MD, FACEP Original Contributors Gregory Ciottone, MD Lucille Gans, MD Patricia Hughes, RN Frank Jehle, MD Taryn Kennedy, MD Gretchen Lipke, MD Mariann Manno, MD Robert McGrath, M.Ed. W. Peter Metz, MD John A. Paraskos, MD Carol Shustak, RN Elizabeth Shilale, RN A. Richard Starzyk Gina Smith, RN Michael Weinstock, MD Fred Henretig, MD Sharon Welsh, RN Theodore Cieslak, MD Lou Romig, MD