Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
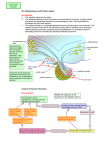
CASE REPORT Pituitary Apoplexy After Thyrotropin-releasing Hormone Stimulation Test in a Patient with Pituitary Macroadenoma Huei-Fang Wang1, Chia-Chang Huang1, Yu-Fang Chen1, Donald Ming-Tak Ho2,3, Hong-Da Lin1,3* 1 Division of Endocrinology and Metabolism, Department of Medicine, 2Department of Pathology and Laboratory Medicine, Taipei Veterans General Hospital, and 3National Yang-Ming University School of Medicine, Taipei, Taiwan, R.O.C. Pituitary apoplexy is a rare complication of pituitary tumors. We report a case of a 41-year-old female with acromegaly due to a pituitary macroadenoma, who developed pituitary apoplexy after a thyrotropin-releasing hormone (TRH) 200 µg intravenous injection stimulation test. Neither emergency computed tomography (CT) scans nor magnetic resonance imaging (MRI), performed 6 hours and 12 hours, respectively, after the active episode, disclosed the evidence of acute hemorrhage or infarction. Two days later, the pituitary mass, removed by transsphenoidal approach, showed ischemic necrosis and acute hemorrhage. The TRH test is generally safe for evaluating pituitary function, but pituitary apoplexy may occur after the procedure. CT and MRI may miss the diagnosis of pituitary apoplexy, especially if performed immediately after the acute episode. [J Chin Med Assoc 2007;70(9):392–395] Key Words: acromegaly, pituitary apoplexy, thyrotropin-releasing hormone, TRH Introduction Pituitary apoplexy is an uncommon clinical syndrome caused by sudden hemorrhage or infarction of pituitary tumors. It is characterized by acute onset of headache, accompanied by vomiting and frequently followed by visual deterioration and ophthalmoplegia. Apoplexy is usually spontaneous, but it may be associated with numerous pathologic states and medications, such as head trauma,1–3 arterial hypertension,2 increased intracranial pressure,1–3 radiotherapy,1,3 diabetic ketoacidosis,2–4 anticoagulation,1–3 estrogens,1,2 and bromocriptine.1,2,5 The possible relationship between the predisposing conditions and the occurrence of pituitary apoplexy may be pituitary necrosis, hemorrhage, or vasculopathy, although the exact mechanism is unclear.1,3–5 Pituitary apoplexy associated with dynamic testing of the pituitary gland is extremely rare.6–8 Patients with this medical emergency need prompt diagnosis for appropriate management. Computed tomography (CT) and magnetic resonance imaging (MRI) play important roles in confirming the diagnosis by revealing a pituitary tumor with hemorrhage and/or necrotic components. In this report, we present a patient who developed pituitary apoplexy 2 hours after injection of thyrotropinreleasing hormone (TRH). CT and MRI studies failed to demonstrate pituitary hemorrhage or infarction. Case Report A 41-year-old female presented to our clinic for further evaluation of her goiter, which was discovered recently. However, acromegaloid picture, accompanied by 5-year history of dysmenorrhea followed by 2-year history of amenorrhea made the presence of pituitary tumor highly probable. Thus, she was admitted to the hospital for investigation of pituitary tumor with acromegaly. At the time of admission, the patient’s blood pressure was 145/93 mmHg and heart rate was 91 beats per minute. Smooth respiratory pattern, goiter (grade II), galactorrhea, increased size of hands and feet, as well as coarse facial contours were noted. Visual acuity was 6/12 in both eyes, and visual field examination *Correspondence to: Dr Hong-Da Lin, Division of Endocrinology and Metabolism, Department of Medicine, Taipei Veterans General Hospital, 201, Section 2, Shih-Pai Road, Taipei 112, Taiwan, R.O.C. E-mail: [email protected] Received: December 7, 2006 Accepted: July 20, 2007 ● 392 ● J Chin Med Assoc • September 2007 • Vol 70 • No 9 © 2007 Elsevier. All rights reserved. Pituitary apoplexy after TRH test Table 1. Pituitary hormones and relative biochemical data GH (N < 5 ng/mL) IGF-1 (N 100–276 ng/mL) PRL (N 3–26 ng/mL) TSH (N 0.4–4 µIU/mL) Free T4 (N 0.8–1.9 ng/dL) T3 (N 82–179 ng/dL) ACTH (N 9–52 pg/mL) TgAb (N < 60 U/mL) TPOAb (N < 60 U/mL) Cortisol (AM) (N 5–25 µg/dL) Cortisol (PM) (N < 5 µg/dL) LH (IU/L) FSH (IU/L) E2 (pg/mL) ADH (N 0.4–2.4 pg/mL) Plasma osmolality (mOsm/kg) Urine osmolality (mOsm/kg) iPHT (N < 50 pg/mL) Ca (N 8.4–10.6 mg/dL) Pre-op 3 d post-op 353 1,076 4.03 1.19 1.39 147 AM 29, PM 14.5 6.2 24.7 18.42 7.73 0.24 1.33 16.58 0.97 290 193 42.05 9.6 4.11 869 0.13 0.34 0.85 56.79 AM 27 17 d post-op 2 mo post-op 3.96 686 0.11 1.25 1.26 152 0.42 1.37 119 15.8 10.2 9.264 0.18 0.07 16.09 0.78 0.72 20.58 24.10 op = operation; GH = growth hormone; N = normal; IGF-1 = insulin-like growth factor-1; PRL = prolactin; TSH = thyroid-stimulating hormone; T4 = thyroxine; T3 = triiodothyronine; ACTH = adrenocorticotropic hormone; TgAb = thyroglobulin antibody; TPOAb = thyroid peroxidase antibody; LH = luteinizing hormone; FSH = follicle-stimulating hormone; E2 = estradiol; ADH = antidiuretic hormone; iPTH = intact parathyroid hormone. L-dopa test GnRH test 1,000 L-dopa test GnRH test TRH test TRH test 7,000 6,000 800 600 4,000 3,000 400 GH (ng/mL) GH (ng/mL) 5,000 2,000 200 1,000 0 0 −40 −20 0 20 40 60 Time (min) 80 100 120 140 Figure 1. Serum growth hormone (GH) levels during L-dopa, gonadotropin-releasing hormone (GnRH) and thyrotropin-releasing hormone (TRH) tests. signified a bitemporal upper field defect. Extraocular muscle movements were normal. Fasting plasma glucose level was 154 mg/dL, and diabetes pattern was also noted by oral glucose tolerance test (OGTT). Basal growth hormone (GH) level (353 ng/mL) was J Chin Med Assoc • September 2007 • Vol 70 • No 9 high, and there was no suppression of GH during the OGTT. The basal endocrine function test results are shown in Table 1. Paradoxical GH responses to Ldopa, gonadotropin-releasing hormone (GnRH) and TRH are demonstrated in Figure 1. Plain skull X-ray 393 H.F. Wang, et al A B Figure 2. Magnetic resonance imaging coronal T1-weighted images show pituitary macroadenoma (arrow) without evidence of pituitary apoplexy: (A) before thyrotropin-releasing hormone (TRH) test; (B) after TRH test. films illustrated erosion and destruction of pituitary fossa. MRI performed the day before TRH stimulation test revealed a lobulated pituitary macroadenoma (38 × 31× 25 mm) with suprasellar extension, compression of optic chiasm, and invasion of left cavernous sinus (Figure 2A). About 2 hours after a bolus injection of 200 µg TRH, the patient had a sudden and intense headache, cold sweating, visual disturbance, ptosis, and diplopia. Blood pressure was 157/82 mmHg, heart rate was 50 beats per minute, and glucose level was 94 mg/dL. Emergency CT showed neither intratumoral hemorrhage nor infarction. Since pituitary apoplexy was highly suspected clinically, MRI was performed 12 hours after the episode, which disclosed no hemorrhage within the tumor (Figure 2B), but slight increase in tumor size (from 15.26 cm3 to 16.15 cm3) compared with the previous MRI image. The patient was administered hydrocortisone (300 mg/ day) intravenously, and her headache and diplopia partially improved. Two days later, the tumor was removed by transsphenoidal approach. Microscopic study indicated a picture of pituitary adenoma with fresh hemorrhage and ischemic necrosis. Immunohistochemically, the tumor was positive for GH, follicle-stimulating hormone, and alpha-subunit. On the second postoperative day, the symptoms mentioned above had all subsided except for diplopia. The follow-up hormone levels are shown in Table 1. One month after the operation, the patient was well without steroid hormone replacement. Three months after operation, her extraocular muscle 394 movements were nearly normal, and the diplopia had disappeared. Discussion The very high basal GH level, up to 353 ng/mL in our case, confirmed the diagnosis of active acromegaly. However, acromegalic patients have both increased plasma levels of GH and a deranged pattern of GH secretion. About 50–80% of acromegalic patients will have GH > 50% of the basal level after TRH stimulation, and less frequently in response to GnRH.9–11 In addition, half of acromegalic patients may have a paradoxical response to L-dopa.9,10 Elevation and suppression of GH after TRH and L-dopa disclosed abnormal GH secretion dynamics in our case. Pituitary apoplexy is a rare clinical syndrome caused by sudden hemorrhage or infarction of the pituitary gland. Headache is the initial and leading symptom of pituitary apoplexy.12 Ocular palsy is also frequent, due to functional impairment of cranial nerves III, IV and VI.2,13 Though apoplectic symptoms frequently occur within minutes or hours after pituitary apoplexy, it has been reported that they may transpire several days later.6 The possible causes of pituitary apoplexy have been reported, but the precise mechanism of apoplexy is not fully understood.1,3,6–8 Pituitary stimulation tests are extremely rare causes of pituitary apoplexy.6–8 In a review of 22 reports of pituitary apoplexy after a pituitary function test, TRH was responsible for 15 cases J Chin Med Assoc • September 2007 • Vol 70 • No 9 Pituitary apoplexy after TRH test of apoplectic events.8 Direct vasospasm effect may be the cause of TRH-induced pituitary apoplexy. In our case, the pituitary apoplexy was noticed shortly after TRH injection, which was quite similar to other reports.6–8 This supported a causal relationship rather than spontaneous occurrence. CT is useful in the acute setting (24–48 hours), and the most reliable CT sign of pituitary apoplexy is the presence of a homogeneously dense lesion showing little or no enhancement of a high density fluid level inside the tumor.1,2 However, CT often fails to show a small hemorrhage or infarction. MRI is superior to CT in these aspects.14 Randeva et al reported that MRI correctly demonstrated 88% of pituitary tumors with hemorrhage, but it was only 21% for CT.13 One limitation of MRI scans is their inability to detect fresh bleeding, so they are performed at least 12 hours after the onset of symptoms to eliminate false-negative scan taken during the hyperacute stage.15 Also, MRI has been shown to be useful for identifying blood components in the subacute setting (4 days to 1 month).2 Although TRH test is a generally safe test for evaluation of pituitary function, pituitary apoplexy may occur after the procedure, especially in patients with a large adenoma. CT and MRI are good techniques for brain imaging, but occasionally, these examinations may miss the diagnosis of pituitary apoplexy, especially when performed immediately after the acute episode. References 1. Cardoso ER, Peterson EW. Pituitary apoplexy: a review. Neurosurgery 1984;14:363–73. J Chin Med Assoc • September 2007 • Vol 70 • No 9 2. Chanson P, Lepeintre JF, Ducreux D. Management of pituitary apoplexy. Expert Opin Pharmacother 2004;5:1287–98. 3. Reid RL, Quigley ME, Yen SSC. Pituitary apoplexy: a review. Arch Neurol 1985;42:712–9. 4. Lufkin EG, Reagan TJ, Doan DH, Yanagihara T. Acute cerebral dysfunction in diabetic ketoacidosis: survival followed by panhypopituitarism. Metabolism 1977;26:363–9. 5. Yamaji T, Ishibashi M, Kosaka K, Fukushima T, Hori T, Manaka S, Sano K. Pituitary apoplexy in acromegaly during bromocriptine therapy. Acta Endocrinol 1981;98:171–7. 6. Dokmetas HS, Selcuklu A, Colak R, Unluhizarci K, Bayram F, Kelestimur F. Pituitary apoplexy probably due to TRH and GnRH stimulation tests in a patient with acromegaly. J Endocrinol Invest 1999;22:698–700. 7. Drury PL, Belchetz PE, McDonald WI, Thomas DGT, Besser GM. Transient amaurosis and headache after thyrotropin releasing hormone. Lancet 1982;23:218–9. 8. Masago A, Ueda Y, Kanai H, Nagai H, Umemura S. Pituitary apoplexy after pituitary function test: a report of two cases and review of the literature. Surg Neurol 1995;43:158–65. 9. Duncan E, Wass JAH. Investigation protocol: acromegaly and its investigation. Clin Endocrinol 1999;50:285–93. 10. Shibasaki T, Hotta M, Masuda A, Imaki T, Obara N, Hizuka N, Takano K, et al. Studies on the response of growth hormone (GH) secretion to GH-releasing hormone, thyrotropin-releasing hormone, gonadotropin-releasing hormone, and somatostatin in acromegaly. J Clin Endocrinol Metab 1986;63:167–73. 11. Grisoli F, Leclercq T, Jaquet P, Guibout M, Winteler JP, Hassoun J, Vincentelli F. Transsphenoidal surgery for acromegaly: long-term results in 100 patients. Surg Neurol 1985;23:513–9. 12. Chen RF, Huang HS, Huang BY, Lin JD, Juang JH, Chang CN. Pituitary apoplexy: a study of eighteen cases. J Chin Med Assoc 1992;50:489–94. 13. Randeva HS, Schoebel J, Byrne J, Esiri M, Adams CBT, Wass JAH. Classical pituitary apoplexy: clinical features, management and outcome. Clin Endocrinol (Oxf) 1999;51:181–8. 14. Chen CC, Wang K, Jap TS, Teng MH, Won GS. Pituitary apoplexy diagnosed by magnetic resonance imaging: a case report. J Chin Med Assoc 1995;55:180–4. 15. Onesti ST, Wisniewski T, Post KD. Clinical versus subclinical pituitary apoplexy: presentation, surgical management, and outcome in 21 patients. Neurosurgery 1990;26:980–6. 395