Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
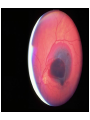
Retina and Vitreous Diseases vitreous Clear, avascular, gelatinous body Normally in contact with the posterior lens capsule, the zoular fibers, the pars plana epithelium anteriorly, retina, and optic disk posteriorly 99% water, the remaining 1% include collagen and hyaluronic acid eye movements induce incessant stress forces, and with age, its composition and structure change Its role in the physiology and pathobiology of the eye is being increasingly appreciated, but its study is complicated due to its invisible nature. Retina The retina is the most complex of the ocular tissues. The macular is used primarily for central and color vision while the remaining retina, is utilized primarily for peripheral and night vision. Retina layer Sensory retina etinal pigment epithelium Examination direct or indirect ophthalmoscope slitlamp (biomicroscope) and contact or handheld biconvex lens Fundus photography and Fundus fluorescein angiography (FFA) B-Scan ultrasonography visual electrophysiologic Optical Coherence Tomography (OCT) OCT OCT is increasingly replace FFA as it is fast, non-invasive test that produces high resolution cross-sections and contour maps of the central retina Vitreous diseases Firm vitreoretinal attachments are observed in areas at the vitreous base, optic disk, fovea, and over the major retinal blood vessels . Vitreous age change The aging vitreous both liquefies and aggregates. Liquefies (synchysis), the process of vitreous gel liquefaction, first appears at around 4 years of age. The process begins in midlife and in most cases progresses slowly into late age Aggregation (syneresis) is a consequence of increased fibril concentration in the gel, associated with a decreased concentration and ultimate absence of fibrils in adjacent areas resulting in liquefaction Vitreous collapsed syneretic cavity Intravitreal cavity filled with liquid breakdown products of syneresis Vitreous floaters muscae volitantes They are usually seen against bright lights or a uniform light background, they might like spots or threads floaters Floaters maybe degeneration of the vitreous (syneresis) or caused by hemorrhage , inflammation or retinal detachment. Flashing lights photopsia A common symptom of an abnormal relationship between the retina and the vitreous Happened on moving eye Vitreous syneresis with focal vitreous traction on vitreoretinal lesions such as lattice degeneration Require no treatment, however, it can induce retinal tears Vitreous collapse Syneresis affects at least 65% of persons over 60 years. Myopies are especially With age, the center of vireous may undergo syneresis and become filled with liquid It should be assumed that patients with new floaters or photopsia have retinal tears or detachment until proved otherwise by thorough examination. Vitreous collapses downward and foreward to create a posterior vitreous detachment Posterior VitreousDetachment PVD refers to the separation of the posterior vitreous cortex from the ILM of the retina. Once liquefied, premacular vitreous can find its way to the retrohyaloid space through a break in the thinned posterior vitreous cortex overlying the macula. Floaters and photopsias are the most common symptoms reported with the abrupt onset of a PVD Floaters are caused by aggregations of collagen fibrils Photopsias caused by vitreoretinal traction are an ominous sign of a retinal tear, particularly when associated with the appearance of multiple floaters Anomalous adhesions between the posterior vitreous face and the retinal surface are the cause of numerous vitreoretinal complications, while the presence of an intact posterior hyaloid provides a scaffold for vascular growth and anteroposterior traction. The Vitreous, the Retinal Interface in Ocular Health and Disease - ResearchGate. Available from: [accessed Mar 27, 2015]. Vitreous collapse causing the retina to tear and detach Vitreous Condensation and Detachment 返回 posterior vitreous detachment, PVD PVD B-Scan 返回 Weiss circle PVD from the disk margin, a ring-shaped opacity on the back of the vitreouscan be seen. Vitreomacular interface (VMI) disease vitreomacular traction (VMT) macular holes epiretinal membrane (ERM) VMT defination The progression of PVD can lead to periods of excessive traction on the macula. Such traction can result in anatomic changes in the contour of the foveal surface, intraretinal pseudocyst formation, elevation of the fovea from theRPE, or a combination that typically results in reduced or distorted vision. VMT OCT scan (1) evidence of perifoveal vitreous cortex detachment from the retinal surface; (2) macular attachment of the vitreous cortex within a 3-mm radius of the fovea; (3) association of attachment with distortion of the foveal surface, intraretinal structural changes, elevation of the fovea above the RPE, or a combination thereof, but no fullthickness interruption of all retinal layers. epiretinal membrane (ERM) nearly half of all eyes with PVD remains residal vitreous on the surface of the retina. This residual vitreous may proliferate to form an epiretinal membrane (ERM) Epiretinal membrane contracture causes macular traction. ERM Macular Hole (MH) macular hole is an anatomic defect in the fovea featuring interruption of all neural retinal layers from the ILM to the RPE. The edge of the hole usually is rounded and may contain intraretinal pseudocysts MH The Gass classified MH into 4 stages. Stage Stage Stage Stage 1 2 3 4 impending hole. occult hole hole with pseudo-operculum hole after PVD MH statge Vitreous hemorrhage Vitreous hemorrhage cause Retinal tear Retinal neovasularization Hypertension Eales’ disease Retinal disorders Diseases of the macula Diseases of the peripheral retina Retinal vascular disease Diseases of the macula Age-related macular degeneration Central serous chorioretinopathy Macular edema Inflammatory disorders involveing the macular Myopic macular degeneration Macular hole Epiretinal macular membrane Macular dystrophies Age-related macular degeneration (AMD) AMD Definition AMD is the leading cause of permanent blindness in the elderly. The incidence increases with each decade over age 50. It is usually bilateral, but may not be symmetrical AMD is classified into two categories Non-exudative (dry or atrophic ) Exudative (wet or neovascular) Exudative AMD has a prevalence rate of 1.2% and dry AMD has a prevalence of 15.6% among adults aged 43 and older. Nonexudative macular degeneration Signs discrete, round, yellow-white deposits of variable size beneath the pigment epithelium and scattered throughout the macula and posterior pole With time, drusen can enlage, coalesce and increase Histopathologically eosinophilic material lying between the pigment epithelium and Bruch’s membrane Visual impairment may be minimal But the exudative stage may develop suddenly at any time Nonexudative AMD macular drusen, clumps of pigments in the outer retina and eventually progress to geographic atrophy of RPE and choriocapillaris which is the main cause of severe loss of central vision. Typical clinic representation hard drusen Commonly present in all ages on fundus photograph. The incidence and prevalence of hard drusen is not age related. Their presence alone is not sufficient to diagnose early age related maculopathy. Hard drusen is not associated with increased risk for the development of choroidal neovascularization. Histologically are globular deposits of hyaline material. Clinical features: Symptoms: typically asymptomatic Signs: Small, hard drusen has been defined as being < 64 µm in diameter Discrete, yellow-white deposits that are external to RPE Almost always have distinct and well-defined border Fluorescein angiogram usually demonstrates pin-point window defect. Fundus photograph demonstrates multiple hard drusen Soft drusen Considered to be a feature of AMD. Their presence is associated with increased risk of the development of RPE abnormalities, geographic atrophy and choroidal neovascularization. Clinical features: Symptoms: may have decreased vision or metamorphopsia Signs: Defined as greater than 63µm in diameter Vary in size and shape Occasionally seen as confluent structures with indistinct margins Fluorescein angiogram demonstrates: Early hyperfluorescence Either fading of fluorescence or staining of diffuse drusen in the late phase depending on the phospholipid content Pooling of dye within focal detachments of Bruch's membrane Multiple soft, confluent drusen. exudative or neovascular AMD (wAMD) subretinal choroidal neovascular membrane Symtomps: blurred vision, distortion, scotoma Signs: subretinal hemorrhage, exudate, greyish-green choroidal lesion in macula Fluorescein or indocyanine green angiogram OCT Central scotoma Macula of an eye with exudative age-related macular degeneration. The brownish-colored membrane in the center of the macula is subretinal neovascularization. AMD demonstrating pigment epithelial detachment associated with soft drusen. Note also some hard drusen and areas of pigment clumping Retinal Hemorrhages Secondary To "Age Related" Disciform Macular Degeneration CNVM causing a macular scar Development Of A Hard Disciform Type Scar Treatment Anti-VEGF theraphy: intravitreal iniection 3 times+prn Retinal Detachment Denotes separation of the sensory retina from the underlying retinal pigment epithelium. Three main types Rhegmatogenous detachment Tractional detachment Exudative detachment Symptoms: Blurry or various degree of decreased visual acuity “dark curtain” that obscures peripheral vision Photopsia (subjective visualization of flashing lights) Risk factors: Myopic eyes Family history of retinal detachment Vitreoretinal syndrome Aphakia Rhegmatogenous retinal detachment The most commonly seen retinal detachment. Usually there is/are retinal break(s) induced by posterior vitreous detachment. Fluid from liquefied vitreous can pass through the break(s), enter the potential subretinal space and undermine the retina from the RPE. Signs: Retinal break(s) Undulating bulla, retinal tear flap, or corrugated folds Pigment in vitreous (tobacco dusts) Low intraocular pressure Rhegmatogenous Retinal Detachment Anterior circumferential tear (retinal dialysis) rhegmatogenous retinal detachment Elevation of the transparent detached sensory retina Management: Scleral buckling, cryotherapy or laser to promote firm chorioretinal adhesion. Pneumatic retinopexy for selected superior detachment. Vitrectomy. 治疗 (1) Careful localizatin of retinal break and treatment with cryotherapy or laser in order to create an adhesion between the pigment epithelium and the sensory Retina. (3) Sclera buckling (2) Sclerotomy & drainage of subretinal fluid (4) Pneumatic retinopexy Protocol of rhegmatogenous retinal detachment surgery Traction retinal detachment May be caused by proliferative diabetic retinopathy, proliferative vitreoretipathy, retinopathy of prematurity, or ocular trauma Tractional retinal detachment from proliferative diabetic retinopathy. Commonly associated with: Proliferative diabetic retinopathy Proliferative sickle-cell retinopathy Retinopathy of prematurity Proliferative vitreoretinopahy (PVR) Signs: Proliferative fibrous membrane Smooth, concave detachment toward the anterior segment Vitreoretinal traction Normal intraocular pressure Tractional retinal detachment caused by proliferative vitreoretinopathy (PVR) demonstrating a single starfold associated with diffuse retinal contraction. Management: release of vitreoretinal traction by vitrectomy and membrane dissection. Serous & hemorrhagic retinal detachment Absence of either retinal break or vitreoretinal traction. Be the result of a collection of fluid beneath the sensory retina and are caused by diseases of the retinal pigment epithelium and choroid. Diabetic Retinopathy DR How are the eyes affected? Basically, diabetes is a disease of blood vessels. With large amounts of glucose coursing through the circulatory system DR the most accurate predictor of retinopathy is duration of diabetes. After 10 years, more than half of patients will show signs of retinopathy, and after 15 years this number increases to nearly 90%. • FIGURE 1 Stages of diabetic retinopathy: (a) R1 (background retinopathy: multiple microaneurysms and occasional haemorrhages); (b) R2 (preproliferative retinopathy: multiple blot haemorrhages, intraretinal microvascular abnormalities (IRMAs); (c) R3a (proliferative retinopathy): new vessels on disc and elsewhere (NVD and NVE); (d) M1 (maculopathy): hard exudates within the macula Colour fundus photograph, retinal thickness map and optical coherence tomography scan of patient with diabetic macular oedema. (b) Images from the same patient as (a), showing near resolution of macular oedema following repeated ranibizumab therapy for 12 months. There has been a reduction in the number of haemorrhages in the macula Two Types of Retinopathy A. Nonproliferative diabetic retinopathy (NPDR) Proliferative Retinopathy NPDR “background retinopathy.” The earliest signs of retinal damage arise from capillary wall breakdown, seen on the fundus exam as vessel microaneurysms. Injured capillaries can leak fluid into the retina and the aneurysms themselves can burst, forming “dot-and-blot hemorrhages.” NPDR With worsening retinopathy and vessel damage, the retina begins to show early signs of ischemia. Cotton-wool spots, seen with hypertension and stasis, are gray spots with soft edges that indicate ischemia/infarction of the superficial retinal nerve fibers. As vessel damage progresses, you can also see beading of the larger retinal veins and other vascular anomalies. NPDR Signs Microaneurysm, intraretinal hemorrhages, cotton wool spots and hard exudates Venous tortuosity or beading, capillary dropout and intraretinal microvascular abnormalities (IRMA) Increasing formation of microaneurysm leads to increased vascular permeability of the retinal capillaries and result in retinal edema particularly in the macular area Fluorescein angiography demonstrates Scattered hyperfluorescence dots of microaneurysms which can be associated with minimal dye leakage Spots of hypofluorescense in the area of hemorrhages and exudates Areas of irregular capillary pattern or capillary closure Management Improve patients education and understanding about the disease process. Control of blood glucose, cholesterol and blood pressure. Photocoagulation in severe nonproliferative retinopathy. Annual check-up 5 years after onset for patient aged less than 30 years old, and at time of diagnosis for patients aged 30 and older. Frequency of scheduled check-up depends on the status of the retinopathy Proliferative Diabetic Retinopathy (PDR) PDR With ongoing injury to the retinal vasculature, the vessels occlude entirely, shutting down all blood supply to areas of the retina. In response, the ischemic retina sends out chemicals that stimulate growth of new vessels. This new vessel growth is called neovascularization, and is the defining characteristic of proliferative retinopathy. PDR demonstrating dot and blot hemorrhages, hard exudates and network of new vessels (NVE) with early fibrovascular proliferation tissue extend over the surface of the retina. Advanced proliferative diabetic retinopathy. Characterized by growth of new vessels on the surface of the retina. Symptoms: progressive loss of vision, particularly in those who are not properly followed or treated. Signs new vessels grow on the optic disc, neovascularization of the disc (NVD) or elsewhere (NVE) These new vessels may leak and resulting in retinal edema. They are also fragile and prone to bleed Opaque fibrovascular proliferation tissue often appears on the internal limiting membrane (adjacent to the new vessels) and becomes adherent to the vitreous. Contraction of this fibrovascular tissue may lead to: Distortion or dragging of the macula , Mild to extensive retinal detachment, avulsion of retinal vessels and vitreous hemorrhages Neovascularization of the disc (NVD) Neovascularization of the disc (NVD) • Neovascularization of the retina elsewhere (NVE) • Managements Strict blood glucose, blood pressure and cholesterol control. Photocoagulation for clinically significant macular edema prior to scatter (panretinal) photocoagulation. Consider PRP in severe proliferative diabetic retinopathy. the extent of vitreous hemorrhage or worsening of overall vitreoretinal condition need vitrectomy. Anti-VEGF PRP Diabetic Grading Classification None no diabetic retinopathy Background microaneurysms or hemorrhage venous loop any exudate any cotton wool spot Pre-proliferative venous beading venous reduplicaton multiple blot hemorrhage IRMA (intraretinal microvascula abnormality) Proliferative new vessles on disc new vessles elsewhere preretinal hemorrhage or vitreous blood preretinal fibrosis tractional retinal detachment DR conclusion As you can see, diabetic retinopathy is a big problem as a large percentage of our patients have diabetes. Retinal vessel damage leads to edema, and vessel occlusion stimulates neovascularization that can lead to trouble. Fortunately, better glucose control and surgical treatments have significantly decreased the incidence of visual loss in these patients. Central serous chorioretinopathy serous detachment of the sensory retina as a consequence of focal leakage of fluid from the choriocapillaris through a defect in the retinal pigment epithelium. young to middle-aged men and may be related to life stress events. Symtomps: sudden onset of blurred vision, micropsia, metamorphopsia, and central scotoma Signs: VA moderately decreased, serous detachment of the sensory retina FFA: dye leaking accumulate below the pigment epithelium or sensory retina Treatment 80% spontaneous resorption with 6 months Argon laser photocoagulation directed to the active leak significantly shortens the duration of the sensory detachment and hastens the recovery of central vision. Central retinal artery occlusion Central retinal artery occlusion Typically unilateral. More commonly affect older people in their midsixties, but can also occur in younger patients. Most common cause: systemic hypertension. Other etiologies: diabetes mellitus, emboli from valvular heart diseases, carotid atherosclerosis and circulatory compromise, coagulopathies, collagen vascular diseases, other vasculitides and trauma. Symptoms Sudden, painless loss of vision May have a history of amaurosis fugax ( antecedent transient visual loss) Signs Normal anterior segment in acute cases Pale, whitening, swelling retina especially in the posterior pole Cherry red spot as a presentation of orange reflex from the intact choroidal vasculature beneath the foveola surrounded by the retinal pallor Afferent pupillary defect is usually present Emboli may be seen After 4-6 weeks, the cloudy swelling retinal commonly resolves, leaving a pale optic disc, attenuated retinal vessels, segmentation or "boxcarring" of the blood column Final visual acuity is most often worse than 20/400 Visual acuity of better than 20/40 may be achieved with patent cilioretinal artery Fluorescein angiography demonstrates Delay in retinal arterial filling and arteriovenous transit time Segmentation of the blood column Choroidal vascular filling is usually normal Management Thorough evaluation of systemic etiology. May consider the following treatment to lower the intraocular pressure: ocular massage, anterior chamber paracenthesis. Inhaled Oxyen-carbon dioxide mixture Other treatments may include: oral vasodilator and systemic anticoagulants. Direct infusion of a thrombolytic agent into the ophthalmic artery Central retinal artery obstruction with diffuse superficial retinal whitening in the posterior pole. Note also the marked delay in arterial filling and incomplete venous laminar filling in the later phase of the study. Central retinal vein occlusion CRVO is the second most common retinal vascular disorder. Patients are usually 50 years or older, but it can occur in younger patients. Two clinical types: perfused (nonischemic) - 75%, and nonperfused (ischemic) - 25%. The second eye can develop vein occlusion in 6-17% of cases. Central retinal vein occlusion Symptoms: sudden, unilateral, painless visual loss that can range from better than 20/400 in nonischemic eyes to 20/400 or worse in ischemic eyes Fundoscopic findings Widespread retinal hemorrhages in all four quadrants, which vary in appearance from a small-scattered retinal hemorrhages to marked confluent hemorrhages Marked dilated and tortuous retinal vessels Cotton-wool spots Optic disc edema, macular edema, and retinal thickening Vitreous hemorrhages may be present A relative afferent pupillary defect (RAPD) can be present in ischemic CRVO Collateral optociliary shunt vessels can develop The fundoscopic findings in nonischemic CRVO are relatively milder than the changes seen in ischemic CRVO Branch retinal vein occlusion is involving the superior temporal quadrant Ischemic Central Retinal Vein Occlusion Associated conditions include open-angle glaucoma or various systemic diseases such as diabetes mellitus, systemic hypertension or atherosclerotic cardiovascular diseases. Prognosis: Poor visual prognosis especially if involves a total area of at least 10 disc areas of retinal capillary nonperfusion and poor visual acuity at presentation. Prognosis is better in the nonischemic CRVO especially when initial visual acuity is 20/40 or better or at least better than 20/200. Two-thirds of eyes with ischemic CRVO may develop iris neovascularization or angle neovascularization and subsequent neovascular glaucoma. Retinal neovascularization is uncommon. Nonischemic type may progress to ischemic CRVO in 5-22% of cases. Permanent loss of central vision due to persistent macular edema. Management: Ocular work-up: best-corrected visual acuity, intraocular pressure, slit lamp biomicroscopy, gonioscopy and dilated fundus examination. Monthly visits. Treatment of associated systemic medical condition. Panretinal laser photocoagulation is indicated if neovascularization develops. Retinal degeneration and dystrophy retinitis pigmentosa Retinitis pigmentosa is a group of hereditary retinal degenerations characterized by progressive dysfuncion of the photoreceptors and eventual atrophy of several retinal layers signs Night blindness (nyctalopia) and gradually progressive peripheral visual field loss are the hallmark symptoms In early stage, there are scattered accumulations of pigment shaped as spider or bone-spicule formationon equatorial retina which may, cover a part of blood vessels. waxy-yellowish disc may be seen, with the developing of illness it becomes pale, atrophy with clear margin. Retinal blood vessels are markedly narrowed. In late stage, pigment expands to periphery and posterior pole, if the macula is involved, the central vision decreases obviously ERG is extinguished leukocoria Retinoblastoma Retinoblastoma is a rare but lifeendangering tumor of childhood. For small tumors within the eye, treatment consists of external beam radiation, photocoagulation (laser), or cryotherapy (precise freezing). When tumors are large or if there is little expectation that vision can be preserved, the eye is removed