Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
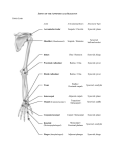
Anatomy Made Easy “MSS” part #10 11 هذا البارت يشمل التفريغ Done By :Dina Naag Edited by: Awn Academic team In this part, we are going to discuss : 1. The axilla boarders and contents 2. The gaps which are located within shoulder. 3. The definition and types of joints. 4. The shoulder joint. The Axilla = Armpit • The axilla extends from the root of the neck into the upper aspect of the medial surface of the humerus. • Axilla is a place where most of the structure that goes from the thorax to the upper extremities pass through, such as arteries and brachial plexus. Axilla • It located medial to the surgical neck of the humerus and lateral to the lateral aspect of the thorax upper part (2nd, 3rd, 4th, 5th costal ribs). • The axilla is pyramidal in shape , with : 1. The apex oriented toward the neck (small inlet) 2. The base practically is going down into the armpit and it is mainly covered by the skin (large outlet) • The base is called the axillary fossa, it is a depression within the axillary region, and it is rectangular in shape CONTENTS AXILLARY LYMPH NODES AXILLARY ARTERY & VEIN BRACHIAL PLEXUS BOUNDARIES APEX BETWEEN THE CLAVICLE,SCAPULA AND 1ST RIB BASE AXILLARY FASCIA ANTERIOR : 1. PECTORALIS MAJOR 2. Subclavius MUSCLE 3. clavipectoral fascia POSTERIOR 1. SUBSCAPULARIS 2. LATISSMUS DORSI 3. TERES MAJOR MEDIAL 1. FIRST 4 RIBS 2. SERRATUS ANTERIOR MUSCLE 1. LATERAL BICEPETAL GROOVE OF THE HUMERUS) Apex • • 1. 2. 3. Upper end of axilla or APEX is directed into the root of neck Its triangular in shape the clavicle participates anteriorly the upper border of the scapula posteriorly the first rib medially. Base • Lower end or Base is bounded in front by the anterior axillary fold formed by pectoralis major muscle • Behind by posterior axillary fold (lateral border of pectoralis) formed by the tendons of latissimus dorsi and teres major muscles • Medially by the chest wall • Lateraly by the long head of triceps Take a look at the transverse section of the shoulder, what can you see? 1. 2. 3. 4. The scapula The first rib The subscapularis that covers the scapula The serratus anterior which inserts into the vertebral border and the inferior angle of the scapula •Anterior wall: • By the pectoralis major,Subclavius, pectoralis minor, small part of the deltoid and clavipectoral fascia New => the deltoid participates in forming the upper part of the axilla. It has nothing to do with the base •Posterior • By the subscapularis, Latissimus dorsi and teres major muscles •Medial • wall: wall: By the upper 4 or 5 ribs and intercostal spaces covered by serratus anterior muscle *note: the long thoracic nerve goes above the serratus anterior •Lateral • wall: By the coracobrachialis and biceps muscles in the bicipital groove of humerus *note: The lateral wall is triangular in shape, and it’s much smaller than the medial wall . The lateral wall contain intertubercular sulcus, it usually fused with medial wall so sometimes we don’t consider it as a lateral wall because the intertubercular ligament covers the intertubercular sulcus. Contents of Axilla • Axillary artery and its branches (the main structure everything else is arranged around it) • Axillary vein and its tributaries • Lymph vessels and lymph nodes • Important nerve plexus the “Brachial Plexus” which innervates the upper limb *note: subclavian artery gives axillary and after it exits the axillary region it gives the brachial artery Axillary Artery • Is a continuation of subclavian artery • Begins at the lateral border of the 1st rib • • Ends at the lower border of teres major It continues as the brachial artery • Closely related to brachial plexus cords • Enclosed with them in the axillary sheath “” • Axillary sheath is continuous with the prevertebral fascia • Pectoralis minor divides it into 3 parts Axillary vein Axillary vein is also covered by the axillary sheath The subclavian vein will divide and give axillary and cephalic (the axillary will continue as basilic) Now this division happens at the level of the axilla The cords of brachial plexus are also covered by the axillary sheath (enveloped by the fascia??) Brachial plexus • comes out from the cervical region, then it goes all the way into the arm and split to give : 1) Radial nerve ‘radial side’ 2) Ulnar nerve ‘ulnar side’ 3) Median nerve ‘posterior aspect • The Brachial plexus is a lesser complex plexus of nerves that comes from the anterior rami of the intervertebral nerves. The Axillary lymph nodes: • are the lymphatics distribution in the axilla, all of them will drain into main subclavian nodes. • That’s why when we have an over-exercise in our hands, the subclavian nodes will be enlarged and we’ll be able to palpate them. • Practically we have the Pectoral nodes which are lateral and anterior, they will drain into the subscapular nodes. Then the subscapular nodes will drain into the central nodes that are located within the axilla. • There’s a connection between the central nodes and the apical nodes, these apical nodes drain the breast. Most of the time when we have breast cancer in a female or in a male, these nodes will be palpated. • The central nodes are deep, where the apical and the subscapular nodes are superficial and can be visualized and palpated from the armpit immediately under the skin by holding the hand in an adduction position. • In the middle of the axilla we have a neurovascular bundle. This bundle is held into a sheath called the axillary sheath. • Inside it we have the medial, lateral and posterior cords of the brachial plexus in addition to axillary artery • More anterior and toward the medial aspect we have the axillary vein. • the Basalic vein and the cephalic vein join together at the level of superior aspect of the axillary region to form the axillary vein which will continue as the subclavian vein the clavipectoral fascia • It is a strong sheet of connective tissue that comes down from the inferior surface of the clavicle, it Splits above to enclose the subclavius muscle. Below it splits to enclose the pectoralis minor muscle, then continues downward as the suspensory ligament of the axilla which joins the fascial floor of armpit. • So the clavipectoral fascia begins at the clavicle and ends down into the skin • It is pierced by 4 important structures which are found in the anterior wall of the apex; 2 inwards and 2 outwards. The 2 inwards are: 1) Lymphatics 2) Cephalic vein: penetrates the axilla from superior and anterior aspect. The 2 outwards are: 1) Lateral pectoral nerve 2) Thoracoacromial artery or its branches: a- Pectoral b- Acromial c- Deltoid d- Clavicular • deep cervical fascia that covers the omohyoid and wind around the lateral aspect of scalenus anterior and scalenus medius. • pectoralis fascia that covers the pectoralis major • clavipectoral fascia that covers the Pectoralis minor and the posterior part of Pectoralis major • The continuation of the clavipectoral fascia is axillary fascia. In the muscles of the shoulder there are many gaps. These gaps are Important: 1. Quadrangular space 2. Triangular space. 3. Triangular interval. Triangular space Quadrangular space: • • • • Is made laterally by the surgical neck of the humerus superiorly by the inferior margin of the subscapularis muscle inferiorly by the superior margin of teres major medially by the long head of the triceps brachii • The structures passing through the quadrangular space are: 1. axillary nerve 2. Posterior circumflex humeral artery and vein. Triangular space: 1. The medial margin of the long head of the triceps brachii muscle 2. The superior margin of the teres major muscle. 3. The inferior margin of the subscapularis muscle or teres minor. • Structures passing through it: Circumflex scapular artery and vein. Triangular interval 1) The inferior margin of the teres major muscle 2) The shaft of the humerus 3) The lateral margin of the long head of the Triceps brachii • Structures passing through it radial nerve The Joints: The Joints: • A joint is the point where two or more bones meet. • There are 3 types of the joints: 1) Fibrous (immoveable): found in the sutures. 2) Cartilaginous (partially moveable): in which the end of a bone is cartilaginous and attached to another cartilaginous surface of another bone ex. The Ribs, the Vertebrae and symphysis pubis. 3) Synovial (freely moveable) joint • All of them contain a thin layer of hyaline cartilage and consist of two ends of bones covered by this layer of hyaline cartilage. • The movement depends on the amount of cartilage, in which the fibrous joints contain minimal amount of cartilage compared to the other types. • Most of the body joints are Synovial (movable) joints Synovial Joint: The bursae are pockets of synovial fluid located between the ligaments and the bones or between the muscles and the bone. This will reduce the friction between them. So you can see the bursae underneath the tendon, and you can see it located between two bones as in the shoulder joint. Also you can see the bursae covering the capsule to protect it. Note =>The bursitis is the inflammation of the bursa Synovial Joints: • Two bones that come along the side of each other and they have to be covered • • • • • • by joint cartilage which is Hyaline cartilage “Articular cartilage”. There’s a distance in the middle of the joint to allow the joint to move, and this distance is a very sterile space called “synovial cavity” . The sterility comes from a membrane called “synovial membrane” The synovial cavity contains a fluid which allow a free movement of the joint, reduce the pressure and reduce the friction and erosion of the articular cartilage. Outer to the synovial membrane, we find a tougher structure called the Capsule. The capsule could be tight or loose. When a joint is greatly movable, its capsule will be loose and vice versa. Outer to the capsule there are Ligaments. These ligaments will hold the joint together and limit its movement In addition, there are muscles that act upon the joint and allow certain movements (flexion, extension, abduction, adduction ...). The Articular disc(meniscus) is made of hyaline cartilage and located within the synovial cavity. It’s found in particular joints in the body such as the Knee, the TMJ and the sternoclavicular joint. In those joints the synovial membrane is splitted, so we’ll find a complex synovial distribution there Notes Certain structures pass through the joint, such as the cruciate ligament in the knee , or the long head of the biceps femoris muscle. The synovial cavity contains nothing other than the synovial fluid, it's a sterile part of the joint, nothing penetrates it. Inflammation of this liquid that exists inside the synovial cavity is called synovialitis "or it could be due to inflammation of the membrane". When some people have pain in the knee joint, they may go to the doctor and inject cortisone there ,cortisone is very bad for the knee, you shouldn't inject cortisone inside the joint! Cortisone is a magical treatment ,it will reduce the inflammation and the infection in a certain part, but it'll never give you a cure.You get the cure by exercising, always by exercise, that will strengthen the joint itself and reduce the amount of fluid that's secreted inside the synovial joint, reduce the inflammation and help the patients to cope with the pain. Bursae Bursae are nothing but synovial membranes; pockets.They are found at the level where there is friction between a tendon and a bone, or between a ligament and a capsule or a muscle and a capsule.. 1- Small pockets of gelatinous structure 2- sterile 3- very tightly packed ** the connective tissue layer is a very tough membrane ,it could burst ,it could be inflated ,and inflammation and infection may occur at this level. It separate certain parts that are located around the joints mainly or between ligaments and bones and will reduce the friction between the two structures. **Subacromial bursa is located underneath the acromion, below the coracoacromial ligament. **If It's inflamed you won't be able to elevate your shoulder, it'll be very painful. Acromion of scapula Coracoacromial ligament Subacromial bursa Fibrous articular capsule Coracoacromial ligament Subacromial bursa Cavity in bursa containing Glenoid cavity synovial fluid containing synovial fluid Hyaline cartilage Tendon sheath (b) Synovial membrane Fibrous capsule Tendon of long head of biceps brachii muscle (a) Humerus If you look over here, you'll be able to see that the long head of the biceps of the humerus enters inside the cavity of the shoulder and reaches the upper portion of the glenoid cavity (it originates from here) Acromion of scapula Coracoacromial ligament Subacromial bursa Fibrous articular capsule Coracoacromial ligament Subacromial bursa Cavity in bursa containing Glenoid cavity synovial fluid containing synovial fluid Hyaline cartilage Tendon sheath (b) Synovial membrane Fibrous capsule Tendon of long head of biceps brachii muscle (a) Humerus Types of synovial joints: 1) Hinge joint: it produces flexion and extension. 2) Pivot joint: it exists between a head and a fossa. We can find it at the proximal ends of the radius and the ulna that’s where the supination and pronation. In this joint, one bone will wind around itself and it’ll be held by the Annular ligament which will fix the joint and allow only the movable bone to move. 3) Ball-and-socket joint wide-range movement joint. It exists between a head of a bone and a depression of another bone. Ex : the head of the femur and the acetabulum. • These joints are complex, with few ligaments, large amount of muscles and loose capsule 4) The condyloid joint: exists within the carpal bone allow movement on two axes: flexion and extension; it can also be tilted sideways (toward the radius and ulna). 5) The gliding joint: Surfaces of these joints are relatively flat and not very mobile; they allow only a narrow gliding range (e.g., vertebrae, certain bones of the carpus). 6) The saddle joint: between the carpal and metacarpal. It’s like riding on a horse’s back and only movable in 2 directions (abductionadduction). Resembles the condyloid joint but allows a wider range of motion; this type of joint is rare • These are synovial joints that exists in the upper and lower extremities (the hand and the foot). TMJ • In the TMJ we have two synovial cavities, one above the disc and the other below, but these synovial cavities adhere at the lateral border of the disc and it appears that the disc is inside the synovial cavity but actually it’s not. So the articular disc is usually inter-capsular but not intersynovial. • The articular discs have different shapes. They could be rounded or semilunar The temporomandibular (jaw) joint it occurs between the articular lower anterior surface of the temporal bone (mandibular fossa) and the head of the mandible (mandibular condyle). Both the fossa and the condyle are covered by hyaline cartilage The Shoulder joint Shoulder Joint it's a complex and a simple joint at the same time..it's complex because of the muscles that surround the joint and affect its movement, and because of the wide range of movement that occurs at this level. It's simple because it has few ligaments and a bigger capsule and because its synovial membrane is straightforward. but this joint occurs between two parts, one part coming from the humerus ,which is the incomplete/half-a-ball part and the very shallow glenoid cavity which belongs to the lateral upper part of the scapula. The cavity is very shallow (not deep) ,so we need to deepen this cavity in order for the head to fit ,we need to have a cartilaginous structure that makes this cavity deeper, and that's what we call "the glenoid labrum" triangular shaped The glenoid fossa of the scapula is a depression on the head of the scapula, between the acromion and coracoid processes. It joins with the head of the humerus. The glenohumeral joint is a multiaxial synovial ball and socket joint. The glenoid labrum is a fibrocartilaginous rim attached around the margin of the glenoid cavity in the scapula. It is continuous above with the tendonof the long head of the Biceps brachii. It deepens the articular cavity,and protects the edges of the bone. goes outside in a triangular way. Due to the very limitedinterface of the humerus and scapula, it is the most mobile joint of the human body.H O W ? When we have a ball that fits in one socket which is big such as the acetabulum (in the hip joint) ,the movement will be limited , now in this case the movement is wider because an "incomplete" head will fit in the glenoid cavity even though we have the labrum. Note The labrum will act in a different way with the long head of the biceps brachi which originates from the supraglenoid tubercle " a small tubercle superior to the glenoid cavity" ,when it comes to the joint, this tendon will spread laterally and inferiorly to be part of what we call "the glenoid labrum" so it'll help the labrum to be stable and will drag it somehow to prevent the head (of the humerus) from dislocation In case of flexion and extension of the shoulder joint. Capsule surrounds the joint and is attached ◦ medially to the margin of the glenoid cavity outside the labruum ◦ laterally it is attached to the anatomic neck of the humerus. the capsule will run from the edges of the glenoid surface more lateral to the anatomical neck of the humerus reaching the two elevations on the lateral aspects of the humerus. The capsule is thin and lax, allowing a wide range of movement. It is strengthened by fibrous slips from the tendons of the the rotator cuff muscles. Note The loosest part of this capsule is the inferior part, the inferior part is like a pocket, it'll allow the abduction and the extension of the arm at the shoulder level .if it was tight and runs obliquely from the inferior aspect of the anatomical neck of the humerus to the lower part of the glenoid cavity ,the movement will be limited ,that's why the capsule is lax and big. Synovial membrane : This lines the capsule and is attached to the margins of the cartilage covering the articular surfaces. It forms a tubular sheath around the tendon of the long head ofthe biceps brachii This is the synovial membrane, encircling the inside, this synovial membrane on the anterior aspect will expand and form a small bursa and that will reduce the friction between the subscapularis muscle and joint capsule. There are three glenohumeral ligaments (between the glenoid cavity and the humerus) in the glenohumeral joint. (1)The superior glenohumeral ligament (SGHL).This ligament resists inferior translation of the humeral head in the adducted shoulder. (2)The middle glenohumeral ligament (MGHL).This ligament resists inferior translation in the adducted and externally rotated shoulder. (3)The inferior glenohumeral ligament (IGHL). This resists humeral head anterior and posterior translation. Coracoacromial ligament (in the coracoacromial join) prevents the superior dislocation of the joint Coracoclavicular ligament which Is composed of Trapezoid and Conoid ligaments The shoulder is made of three joints practically, but the most important is the glenohumeral joint. The capsule of the shoulder is reinforced by the coracohumeral ligament The transverse humeral ligament is another ligament into which the tunnel between the two elevations on the lateral aspect of the humerus, allow the synovial sheet that covers the long head of the biceps to pass through to the inside of the capsule but not inside the synovial membrane. The coracoclavicular ligament is made of two bands that connect the inferior surface of the clavicle with the superior surface of the coracoid process. The transverse humeral ligament strengthens the capsule and bridges the gap between the two tuberosities. The coracohumeral ligament strengthens the capsule above and stretches from the root of the coracoid process to the greater tuberosity of the humerus. Remember : bursae in the capsule that aid mobility: Subacromial bursa (between joint capsule and acromion of scapula). Subscapular bursa (between joint capsule and tendon of subscapularis muscle) The movements of this joint are: • • • • Flexion , Extension Abduction , Adduction Lateral Rotation , Medial Rotation Circumduction . Clinical aspect • A subglenoid displacement of the head of the humerus into the quadrangular space can cause damage to the axillary nerve. This is indicated by paralysis of the deltoid muscle and loss of skin sensation over the lower half of the deltoid. • Downward displacement of the humerus can also stretch and damage the radial nerve.