Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
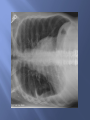
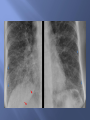
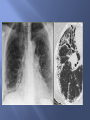
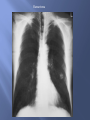
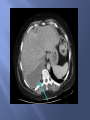
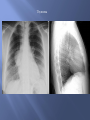
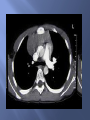
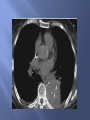
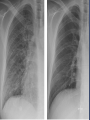
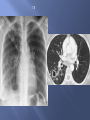
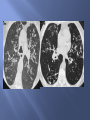
2014/2015 Hassan Al-Balas, MD Imaging modalities in chest evaluation. Chest pathology: Lung parenchymal pathology Mediastinal pathology. Pleural pathology. Specific Entities: Pulmonary edema. TB. Airway disease. Pneumothorax. Chest X-Ray: PA and Lateral views: PA view is obtained with patient in standing position and in full inspiration. Lateral chest view is obtained with left side against the cassette to minimize cardiac magnification. AP view: Portable view is obtained with patient in supine or sitting patient. Because of decreased X Ray source patient distance, there is significant magnification factor. Usually obtained in sick patients in ICU and is less useful than PA view. Evaluate PA CXR for adequate and proper technique: Penetration: Faint visualization of the thoracic disc spaces behind the cardiac shadow. Rotation: Thoracic spine process is midway between medial ends of the clavicles. Inspiration: Adequate inspiratory film should show the dome of the diaphragm below the 10th rib posteriorly. Chest X-Ray: Special views: Decubitus view: Obtained with patient on his lateral side. Is used to evaluate: Size and possible loculation of the pleural effusion. Small pneumothorax in patient an upright CXR is not possible. Air trapping. Lordiotic view: Obtained with patient leaning backward. Useful for evaluation of lung apices. CT Scan: Non-contrast CT: Is used to evaluate lung parenchyma, e.g. metastasis. Contrast enhanced CT: Essential for evaluation of mediastinal and hilar structures. High Resolution CT: Non contrast thin section images. For evaluation of interstitial lung disease. MRI: Very limited value for chest evaluation. Nuclear Ventilation/ perfusion scans: To evaluate for pulmonary embolism. Angiography: Evaluate vascular pathology. Individual alveoli are too small to resolve, but together they appear radiolucent. 12 Air space disease. Interstitial lung disease. Focal lung masses/ Nodules. Filling of alveoli by: water, blood, pus, proteinaceous fluid or cells - Ground glass - Consolidation 14 Also known alveolar lung disease. Features of Airspace disease: Air bronchogram. Respects lobar anatomy. Ill-defined borders except at fissures. Airspace disease could be: Partial: Ground glass opacity. Complete: Consolidation. Causes of ALD: Acute: Pulmonary edema. Pneumonias. Pulmonary hemorrhage. Chronic: Broncho-alveolar carcinoma. Lymphoma. Alveolar proteinosis. - Diffuse and bilateral. - May have regional distribution. 19 Normal interstitium is not seen on CXR unless is diseased. Four patterns of interstitial lung disease: Linear. Reticular. Nodular Reticulo-nodular End stage pattern of interstitial lung disease = honeycombing. Small sub-pleural cystic changes of the lung parenchyma. Most prominent in the lower lung lobes. Nonspecific finding represent end stage ILD secondary to several underlying pathology. Linear pattern: Thickened interlobular septa. Called kerley A and B lines: kerley A lines: Long lines(2-6cm). Centrally located radiating from hila. More common in upper and mid lung fields. Kerley B lines: Short (1-2cm). Peripheral sub-pleural location. More common in lower lung fields. Common etiology: Pulmonary edema: most common etiology. Interstitial pneumonia-viral or mycoplasma. Lymphangitis carcinomatosis. Reticular pattern: Result from summation of irregular linear opacities. Usually associated with low lung volumes. Classic example: Idiopathic pulmonary fibrosis. Asbestosis. Scleroderma. UIP Nodular pattern: Numerous small nodules (1mm-10mm in diameter). Miliary pattern: small nodules 1-2mm in diameter. Classic examples: Miliary TB. Sarcoidosis. Silicosis. Metastasis from thyroid, kidney, … Characterization of focal lung pathology: Size: Nodule(<3cm) vs. mass(>3cm). Number: Single vs. multiple. Cavitation: Presence and thickness of the cavity. Calcifications: Presence and pattern of calcifications. Margins: Rounded vs speculated. Bronchogenic carcinoma: Adenocarcinoma: Most common. Peripherally located. Broncho-alveolar carcinoma is a subtype. Squamous cell carcinoma: Second most common type. Strong smoking association. Centrally located. Most likely to cavitate. Large cell carcinoma: Rare type, peripherally located tumor. Small cell carcinoma: Strong smoking association. Centrally located. Very poor prognosis. Hamartoma Pleural effusion: Accumulation of transudate or exudate fluid in the pleural cavity. Signs of pleural effusion: Blunted costo-phrenic angle. Meniscus sign. Opacification of hemithorax. Loculated effusion: Usually seen in empyema or malignant effusion. Failure of layering on decubitus film. CT may show split pleural sign. Normal R costophrenic angle Blunted L costophrenic angle When 200-300cc of fluid accumulate in pleural space, the usually acute costo-phrenic angle becomes blunted Meniscus Sign l l l Pleural fluid tends to rise higher along its edge producing a meniscus shape medially and laterally Usually only lateral meniscus can be seen The meniscus is a good indicator of the presence of a pleural effusion DDX: Total lung collapse/ atelectasis. Entire lung consolidation. Large pleural effusion. Post pneumonectomy. Opacified hemithorax l l l l In atelectasis, there is s shift toward the side of the opacification. In pleural effusion, there is a shift away from the side of the opacification. In pneumonia, there is no shift. In pneumonectomy, the 5th rib is usually absent. Mediastinal masses can be differentiated from lung parenchymal lesions by their smooth contour since they are covered by parietal pleura. The mediastinum is divided anatomically into four compartments: Superior. Anterior. Middle. Posterior. Superior mediastinum: Located between the thoracic inlet and a line connecting sterno-manubrial joint with T4 body. DDX of superior mediastinal mass: Lesion extending from the neck e.g. thyroid mass, cystic hygroma. Lymphadenopathy. Vascular abnormalities e.g. aneurysm. Anterior mediastinum: Also known pre-vascular space. Located between the stenum anteriorly and pericardium and great vessels posteriorly. It contains lymph nodes and thymus. DDX of anterior mediastinal mass are: 4 T’s Thymoma Teratoma Thyroid Terrible lymphoma. Lymphadenopathy Thymoma Middle mediastinum: Also known vascular space. Located between the anterior and posterior mediastnum. Contains the heart, pericardium, trachea and major arteries and veins. DDX of middle mediastinal masses: 3 A’s. Vascular/ aneurysm. Lymphadenopathy. Congenital lesions. Posterior mediastinum: Post vascular space. Located posterior to the heart and anterior to the spine. Content: descending aorta, esophagus, sympathetic chains and lymph nodes. DDX of posterior mediastinal masses: Neurogenic tumors-most common. Others e.g. lymphoma, descending aortic aneurysm, esophageal varices, hiatal hernia,.. Usually results from congestive heart failure. It may/ may not be associated with cardiomegaly. Other causes of pulmonary edema includes: Renal failure. fluid overload. Two types of pulmonary edema: Interstitial pulmonary edema. Alveolar pulmonary edema. Congestive Heart Failure Four Signs of Pulmonary interstitial edema l Thickening of the interlobular septa: n l Kerley B lines Peribronchial cuffing: n Wall is normally hairline thin l Thickening of the fissures l Pleural effusions Peribronchial Cuffing l Bronchial wall is usually not visible l Interstitial fluid accumulates around bronchi l Causes thickening of bronchial wall l When seen on end, looks like little “doughnuts” l Meaningful when seen distal to hilar area 70 Fluid in The Fissures l Fluid collects in the subpleural space n l l Between visceral pleura and lung parenchyma Normal fissure is thickness of a sharpened pencil line Fluid may collect in any fissure n Major, minor, accessory fissures, azygous fissure Fluid in the minor fissure 73 Congestive Heart Failure Pulmonary alveolar edema l Fluffy, indistinct patchy densities l Outer third of lung frequently spared n l Bat-wing or butterfly configuration Lower lung zones more affected than upper Minor fissure Pulmonary Edema 154 slides 75 75 Normal cardiothoracic ratio is less than 50%. Several entities may cause apparent cardiomegaly: Portable AP view. Obesity. Ascites. Pectus excavatum. Cardio-thoracic Ratio <50% Two forms of TB: Primary: Usually is a disease of childhood. Usually resolves without trace or may leave Ghon complex. Usually mild consolidation associated with unilateral hilar and mediastinal lymphadenopathy. Reactivation TB: Ill-defined opacity associated with cavitation and satellite lesions. Affects mostly posterior segment of the upper lobes or superior segment of the lower lobes. TB Includes: COPD. Emphysema. Chronic bronchitis. Bronchiactasis. Cystic vs. cylindrical. Focal vs. diffuse l l l l l There are two layers of pleura- parietal and visceral-the pleural space between them . Normally there is no air in the pleural space. The visceral pleura is inseparable from the lung parenchyma and moves with the lung. When air enters the pleural space, the parietal and visceral pleura separate making the visceral pleura visible The thin white line of the visceral pleura is called the visceral pleural white line You must see the visceral pleural white line to make diagnosis of pneumothorax A pneumothorax will be visible as a thin white line - the visceral pleural white line Bullous Emphysema Enlarged Retrosternal Air Space 154 slides Flattened Diaphragms 89 89 Skin fold vs. Pneumothorax l l A fold of the patient’s skin may become trapped between the patient and cassette Skin folds are common n l Especially in patient’s who have lost a great deal of weight This skin fold can mimic a pneumothorax This is an edge Dense Lucent Skin Fold The key difference is that a skin fold is an edge consisting of a density (light) and then a lucency (dark) This is a line Lucent Dense Lucent Pneumothorax Whereas the visceral pleural line is a thin white line with a lucency (darker) on both sides of it Skin Fold Pneumothorax Types of Pneumothoraces l Two major types of pneumothorax n Simple: n n n In a simple pneumothorax, there is no shift of the heart or mediastinal structures (trachea). Air in left hemithorax balances the air in the right hemithorax. Tension: l Progressive loss of air into pleural space causing a shift of the heart and mediastinal structures away from side of pneumothorax l Opposite lung is compressed l Respiratory function severely compromised Tension pneumothorax