Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
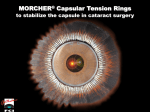
ORIGINAL ARTICLE ARCH SOC ESP OFTALMOL 2008; 83: 589-594 ANATOMICAL REPERCUSSION ON THE ZONULAR APPARATUS AFTER A CAPSULAR TENSION RING INSERTION IN SWINE EYES ESTUDIO EXPERIMENTAL SOBRE LA REPERCUSIÓN ANATÓMICA DE LA ZÓNULA DE ZINN TRAS LA INTRODUCCIÓN DE UN ANILLO ENDOCAPSULAR EN OJOS DE CERDO COLOMÉ-CAMPOS J1, ORTEGA-USOBIAGA J2, SHAHIN M1, FORCADELL M3, PINO A3, FORTEZA T3, BAUBÍ C3 ABSTRACT RESUMEN Purpose: To carry out an experimental and descriptive study that exhibits the anatomical repercussions on the zonular apparatus after a capsular tension ring (CTR) is inserted. Methods: CTRs were inserted in five swine eyes (four with forceps, one with an injector). Two additional eyes were left untouched for control purposes. The integrity of the suspensory ligament was examined by scanning electron microscopy. Results: We did not observe alterations in the integrity of the zonular apparatus. The suspensory ligaments adopted a new fold configuration. Conclusions: CTR insertion is a safe therapeutic tool to maintain the integrity of the lens zonules in elastic, large diameter capsular bags (Arch Soc Esp Oftalmol 2008; 83: 589-594). Objetivos: Valorar experimentalmente la integridad morfológica de los ligamentos suspensorios de la zónula de Zinn (LSZZ) tras la introducción de un anillo de distensión capsular (ADC) mediante un estudio descriptivo. Métodos: Se utilizaron siete ojos de cerdo a los cuales se realizó una extracción extracapsular de cristalino transparente. A cuatro se introdujo un ADC con pinzas y al quinto con inyector. Los otros dos se utilizaron como control. Se examinó la integridad anatómica y la nueva configuración de los LSZZ con un microscopio electrónico de barrido. Resultados: No se observaron alteraciones en la integridad de los LSZZ. Los LSZZ adoptan tras la introducción de un ADC una nueva trayectoria de repliegue consecuencia de la nueva disposición del saco capsular. Conclusiones: En un modelo experimental con ojos de cerdo no se encontraron lesiones en los LSZZ por lo que parece que, en cápsulas elásticas y Key words: Capsular tension ring, lens zonules, clear lens extraction, zonular dialysis. Received: 26/9/07. Accepted: 25/9/08. 1 Ph.D. in Medicine. Ophthalmology Service. Verge de la Cinta Hospital of Tortosa. Tortosa. Spain 2 Ph.D. in Medicine. Baviera Clinic. Bilbao. Spain. 3 Graduate in Medicine. . Ophthalmology Service. Verge de la Cinta Hospital of Tortosa. Tortosa. Spain Correspondence: Jordi Colomé Campos C/. Joan Miró, 3, esc. B 3.º 2.ª 43500 Tortosa Spain E-mail: [email protected] COLOMÉ-CAMPOS J, et al. de gran diámetro, la inserción de un ADC no produce roturas en los LSZZ. Palabras clave: Anillos de distensión capsular, zónula de Zinn, extracción extracapsular de cristalino transparente, diálisis zonular. INTRODUCTION The presence of defects in the integrity of the Zinn Zonule (SLZZ) suspensory ligaments is a circumstance that makes surgical intervention of the cataract by means of phacoemulsification difficult even in the hands of experienced surgeons. Different maneuvers are known to rectify this surgical problem, from the realization of classical and practically obsolete intracapsular or extracapsular surgery, to the introduction or placing of the intraocular lens in distinct locations of the capsule sac (CS) such as the anterior chamber or the ciliary sulcus. A nearly standard surgical resource is the introduction of a capsular tension ring (CTR) in the interior of the CS. The effectiveness that the CTR generates is well known since the beginning of its use in 1991(1) when we find ourselves against a weakness or dialysis of the SLZZ to conserve the anatomical integrity of the CS thanks to the forces of centrifugal traction that the CTR generates in the absence of the lens. In this way, it is normal to place the CTR in circumstances such as pseudo exfoliation syndrome, myopia magna, aniridia, uveitis and pigmentary retinosis, as well as cases of maximum expressions of weakness such as the zonular dialysis that we find in badly formed syndromes such as the Marfan, Ehlers-Danlos or Weill- Marchesani or even the post-traumatic or iatrogenic etiology (2) (3). There are extreme cases where these CTR require a suction support that makes it necessary to suture it in the walls of the ocular globe (4). The introduction technique of the CTR is manual, even with the help of forceps or perhaps an injector. However, when we proceed to place it there is a degree of aggression in the integrity of all the CS and its stabilization ligaments, even more at the area of initial introduction, which is where the maximum tangential traction (5) is generated. The aim of our study is to understand under electronic microscope and by means of a descriptive study the extent of aggression that the use of these rings cause. If so, then perhaps it is 590 worth considering that the use of CTR may, in some circumstances, generate possible risks that modify the practice of surgical intervention. SUBJECTS, MATERIAL AND METHODS Seven pig eyes of eight months from the municipal slaughterhouse were used. After sacrificing the animals, they were enucleated for 30 minutes. Afterwards they were placed in a recipient with saline phosphate 0.1 M tampon and conserved at 4ºC. At 12 hours of the enucleation and after the excision of the corneal-scleral cask and the iris a 5mm diameter capsulorrhexis was performed with the help of a cystotome and Utrata forceps proceeding from the extracapsular extraction of transparent lens after hydro-expression maneuvers. The cortex was aspirated with a Simcoe type cannula. Directly afterwards a series of CTR of PMMA, selected randomly, were introduced into each eye. The first four rings were introduced with a McPherson type forceps and the fifth with the help of an injector. For the first eye we used a CTR Corneal ® model ATC110 of 11mm of diameter, for the second a CTR Oculaid ® model PC275 of 12 mm, for the third eye a CTR Morcher ® type 14 of 12 mm, for the fourth eye a CTR Ophtec ® of 13 mm and for the fifth eye we introduced an CTR AMO Injector Ring ® of 11 mm (table I). As control we used two eyes, one which had only had a extracapsular extraction of transparent lens realized but without the introduction of ring, and the other where the lens had been conserved. To stop we proceeded to resect the posterior wall of the ocular globe with the aim of obtaining an anterior and posterior perspective of the SLZZ. The ocular globes were introduced into a fixing substance of glutaraldehyde at 6% according to the Karnovsky technique (6) and were conserved at a minimum of 4ºC for 2 hours prior to processing. The samples were washed with phosphate tampon and fixed with tetraosimio oxide to proceed ARCH SOC ESP OFTALMOL 2008; 83: 589-594 Endocapsular rings and Zinn zonule Table I. Capsular distention rings utilized in the study Capsular distention rings Material Diameter Corneal® ATC 110 Oculaid® PC275 Morcher® 14 Ophtec® AMO® Injector Ring PMMA PMMA PMMA PMMA PMMA 11 mm 12 mm 12 mm 13 mm 11 mm with dehydration by means of a series of alcohols of growing concentrations and finished in a solution of aniloacetate. After obtaining the critical point with CO2 the samples were recovered with gold by the «sputtering» procedure. The distance of work used was 39 mm and the scanning electron microscope used was a JSM-6400 property of the Universidad Rovira y Virgili. The SLZZ were selected from the quadrants of the four main meridians of each eye in steps of 130 micrometers and their integrity observed, measured in number of fibrillar fractures, and density, counting the number of fibers within the 130 micrometers. The configuration of the trajectory of the SLZZ was also studied to determine whether it maintained its normal straight line, and the insertion at the level of the capsular sac, registering the number of disinsertions. The study was made from an anterior perspective comparing it with the control eyes and the images enlarged to10X, 75X, 150X, 200X, 250X, 300X, 400X, 600X, 1000X and 2500X were registered. Fig. 1: Scanning electron microscope image (x600) where the integrity of the suspensory ligaments is shown at its CS insertion (arrow) after the introduction of an CTR with injector. Fig. 2: Scanning electron microscope image (x150) showing the imprint generated by CS (*) on adapting to the small orifices in the present CTR (arrow). RESULTS No alterations in the SLZZ integrity were detected in any of the eyes studied, since in none of the evaluated quadrants, either for those that introduced a CTR, with an injector (fig. 1) or not (figs. 2, 3 y 5), or for the control eyes (fig. 4) were any fractures or disinsertions observed. The density was kept stable with average figures of 43 fibers per every 130 micrometers, very similar to that of the control eyes that was 46 fibers. However, alterations in the configuration or trajectory of the SLZZ were found when compared with the control eyes, as the presence of a capsular sac in absence of the lens but with the introduction of an CTR caused changes in the architecture of the tridimesional network of the SLZZ, in such a way Fig. 3: Scanning electron microscope image (x75) showing the relief of the edges of the capsulorrhexis (arrow) and of the Zinn zone (*). ARCH SOC ESP OFTALMOL 2008; 83: 589-594 591 COLOMÉ-CAMPOS J, et al. Fig. 4: Scanning electron microscope image (x100) showing the ciliar muscle (*) and the density of the fibers for one of the studied quadrants in the control eye. that these lost the normal straight line configuration presenting a new trajectory and arrangement in the shape of posterior angulation and fold (fig. 6). DISCUSSION The study of the present work has been carried out on young pig eyes. It is assumed that the integrity of all the suspensory system of the lens as well as the elasticity of the CS was completely conserved (7). On extrapolation the design of the work on humans it should be considered that the CTR is normally used on eyes that supposedly exhibit weakened zonules, where the resistance to traction in the course of the cataract operation is much less than under normal circumstances, as has been observed in ocular postmortem tinctions (8). For example it has been demonstrated that in pseudoexfoliative syndromes the resistance of the SLZZ to traction is four times less, and in some patients the fibers are even found broken or deteriorated before the surgical act (9). The CS of pig eyes are estimated to be a diameter superior to that of humans (10), but despite this, in our study, on treating young eyes we have observed a CS with an average diameter of 12.1 mm (fig. 7), slightly greater than CS of the human eye that is of 10.3 to 10.8 mm of diameter when it is empty (11, 12). We have used CTR designed for use in humans and of an average size of 11 mm. We could imagine that the introduction of an ADC in a SC of greater size requires less friction- resistance than the introduction in a SC of lesser size. 592 Fig. 5: Scanning electron microscope image (x100) showing the ciliar muscle (*) and the density of fibers in its insertion to the CS for one of the quadrants studied in an eye with CTR. Anatomical changes were not observed with respect to the control eye. The introduction maneuver of an ADC is relatively easy in normal conditions. However in some complex cases or if the entrance is made in an excessively traumatic manner, or even if the design of the CTR is not the most adequate, it could generate severe traction on the fornix of the CS that could even perforate it (2). It has been described that the use of CTR with the help of injectors could avoid or minimize the traction forces on the SLZZ and the CS. It is with this aim that we have used one of the eyes for observing the microscopic response after its introduction. The SLZZ exhibits an enormous distending capacity and an important firmness in capsular and ciliar insertions (13). It has been described that the fibers could increase in length four times their orig- Fig. 6: Scanning electron microscope image (x300) showing the back of the equator of the lens CS (*) after the introduction of a CTR and the new configuration of the posterior fold that the suspensory ligaments adopt (arrow). ARCH SOC ESP OFTALMOL 2008; 83: 589-594 Endocapsular rings and Zinn zonule Fig. 7: Diameter of the lens of one of the pig eyes used. inal size (14, 15) without evidence of breaks, fissures or disinsertions. However with the passing of time the SLZZ become finer and decrease in number which causes an important interpersonal variability of traction resistance (16), circumstances to consider when performing maneuvers that could alter the previously debilitated anatomical integrity. We have found alterations in the trajectory of the SLZZ compared with control eyes, and we assume that they are due to the fact that the CTR generate centrifugal forces on the equator of the CS that provokes certain distension on the SLZZ. It will also have to be contemplated that with the extraction of the lens the biconvexity of the CS remains reduced, a factor to consider for interpreting the new disposition of the SLZZ and its possible repercussion in the mechanism of accommodation. REFERENCES 1. Hara T, Hara T, Yamada Y. «Equator ring» for maintenance of the completely circular contour of the capsular bag equator after cataract removal. Ophthalmic Surg 1991; 22: 358-359. 2. Menapace R, Findl O, Georgopoulos M, Rainer G, Vass C, Schmetterer K. The capsular tension ring: designs, applications, and techniques. J Cataract Refract Surg 2000; 26: 898-912. 3. Pitrová S. A distance ring for stabilization of the lens capsule (a multicenter clinical study). Cesk Slov Oftalmol 1998; 54: 299-304. 4. Tokuda Y. In the bag IOL suture fixation represents a new approach to zonular dehiscence. Ocular Surgery News 1997; 8: 9. 5. Colomé Campos J, Pérez Moreda F, Belmonte Martínez J. Estudio experimental de la acción de los anillos endocapsulares en relación a la extensión de la diálisis zonular. Microcirugia Ocular 1999; 7: 33-38. 6. Karnovsky MJ. A formaldehyde-glutaraldehyde fixative of high osmolality for use in electron microscopy. J Cell Biol 1965; 27: 137-138. 7. Krag S, Olsen T, Andreassen TT. Biomechanical characteristics of the human anterior lens capsule in relation to age. Invest Ophthalmol Visc Sci 1997; 38: 357-363. 8. Wilson DJ, Jaeger MJ, Green WR. Effects of extracapsular cataract extraction on the lens zonules. Ophthalmology 1987; 94: 467-470. 9. Guzek JP, Holm M, Cotter J, Cameron JA, Rademaker WJ, Wissinger DH, et al. Risk factors for intraoperative complications in 1000 extracapsular cataract cases. Ophthalmology 1987; 94: 461-466. 10. Lee DH, Lee HY, Lee KH, Chung KH, Joo CK. Effect of a capsular tension ring on the shape of the capsular bag and opening and the intraocular lens. J Cataract Refract Surg 2001; 27: 452-456. 11. Galand A, Bonhomme L, Collée M. Direct measurement of the capsular bag. J Am Intraocul Implant Soc 1984; 10: 475-476. 12. Richburg FA, Sun HS. Size of the crushed cataractous capsule bag. J Am Intraocul Implant Soc 1983; 9: 333335. 13. Streeten BW, Licari PA. The zonules and the elastic microfibrillar system in the ciliary body. Invest Ophthalmol Vis Sci 1983; 24: 667-681. 14. Raviola G. The fine structure of the ciliary zonule and ciliary epithelium. With special regard to the organization an insertion of the zonular fibrils. Invest Ophthalmol 1971; 10: 851-869. 15. Canals M, Potau JM, Costa J. Estructura y propiedades elásticas de la zónula cristaliniana. Arch Soc Esp Oftalmol 1999; 74: 131-136. 16. Buschmann W, Linnert D, Hofmann W, Gross A. The tensile strength of human zonule and its alteration with age. Albrecht Von Graefes Arch Klin Exp Ophthalmol 1978; 206: 183-190. ARCH SOC ESP OFTALMOL 2008; 83: 589-594 593