Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
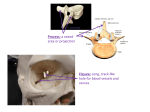
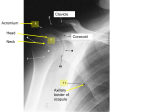
Journal of Dental and Oral Health Scient Open Access Exploring the World of Science ISSN: 2369-4475 Case Report Alternative Management Approach of Dislocation and Hemarthroses of the Mandibular Condyle into the Middle Cranial Fossa in a Mixed Dentition: A Case Report and Review of the Literature This article was published in the following Scient Open Access Journal: Journal of Dental and Oral Health Received February 11, 2016; Accepted October 07, 2016; Published October 14, 2016 Ida Anjomshoaa1* and Robert Pellecchia 2 The Brooklyn Hospital Center Division of Oral and Maxillofacial Surgery, 151 Ashland place, Brooklyn, NY, 11201, USA 2 Oral and Maxillofacial Surgery Program Director at Geisinger Medical Center, 100 North Academy Ave, Danville, PA 17822-1336, USA 1 Abstract This case represents an alternative and more feasible approach to successful reduction of an intact condyle into the middle cranial fossa in a child with mixed dentition. We describe the treatment of a 7-year-old female who fell off her bicycle resulting in right mandibular condyle dislocation into the middle cranial fossa. The patient was taken to the operating room and the right mandibular condyle was manually disimpacted. Brackets and orthodontic bands were cemented on teeth, and inter-arch stainless steel ligatures ties were placed for inter-maxillary fixation for a period of four weeks. Our conservative management was successful resulting in no relapse or ankylosis of the condyle. Orthodontic appliances can provide a good alternative to conventional approaches for maxillomandibular fixation. Arch bars in the mixed dentition are sometimes difficult to stabilize with compromise in maintaining adequate oral hygiene. For a child, orthodontic bracketing is a far more acceptable modality of treatment. Case Report Condyle dislocation is defined as displacement of the condyle out of the glenoid fossa while it still remains within the joint capsule [1]. The condyle can be dislocated in many directions, with antero-medial and anterior dislocation being the most common [2-4]. On the contrary, dislocation of an intact condyle into the middle cranial fossa is very rare [24,6]. In general the condyle has a large head size compared to the glenoid fossa which makes luxation out of the glenoid fossa much more difficult. 5 Impact to the condyle from trauma more commonly results in ipsilateral or contralateral neck fracture as a defense mechanism preventing the intrusion of the condyle into the brain [6-8]. Despite these characteristics of the condyle there have been cases reported where the intact mandibular condyle has been dislocated into the middle cranial fossa without the condyle fracturing itself. The purpose of this case report is to provide an alternative management of this type of dislocation in a young child in the mixed dentition. A 7-year-old female fell off her bicycle and struck her chin to the ground on June 15th, 2013. She was taken to the emergency room at a regional hospital where her chin laceration was repaired. According to the patient’s mother she did not have any loss of consciousness at the time of the incident. X-rays of the mandible were done and the patient was discharged home. The next day the mother came to Geisinger Medical Center stating that her daughter felt worse. She was complaining of headaches, jaw pain and dizziness with multiple episodes of nausea and vomiting. A maxillofacial computed tomography (CT) and a head CT were ordered. *Corresponding author: Ida Anjomshoaa, DMD, Chief Resident, The Brooklyn Hospital Center Division of Oral and Maxillofacial Surgery, 151 Ashland place, Brooklyn, NY, 11201, USA, Tel: 718-250-8956, Fax: 718-250-8539, Email: [email protected] Volume 2 • Issue 7 • 049 Upon clinical examination, the patient had moderate pinpoint tenderness to palpation in the right temporomandibular joint (TMJ) and preauricular area. Swelling and trismus were noted with a maximum incisal opening of 5 millimeters, and a slight deviation of the lower third of the face to the affected side. She was alert and oriented to person, place, and time and neurologically stable. She had no cranial nerve or sensory deficit. In the emergency department Trauma Surgery, Ear Nose Throat, Pediatric Neuropsychology, Oral and Maxillofacial Surgery (OMFS) and Neurosurgery were consulted. Maxillofacial CT revealed a comminuted fracture of the squamous portion of the right temporal bone fracture in the TMJ region and dislocation of the intact right mandibular condyle into the middle cranial fossa (Figures 1a and 1b). The patient was admitted to the Pediatric Trauma Surgery Service. From Neuropsychological and Neurosurgery testing, the patient was found to have normal www.scientonline.org J Dent Oral Health Citation: Ida Anjomshoaa, Robert Pellecchia (2016). Alternative Management Approach of Dislocation and Hemarthroses of the Mandibular Condyle into the Middle Cranial Fossa in a Mixed Dentition: A Case Report and Review of the Literature Figure 1a: Coronal CT scan representing the right mandibular condyle displaced superiorly into the middle cranial fossa. Page 2 of 5 Figure 2a: Patient in intermaxillary fixation with orthodontic appliances and stainless steel ligature ties. Figure 2b: Patient ten days post-operatively following placement of elastics. Figure 1b: Sagittal CT scan view revealing penetration of the condyle into the middle cranial fossa. cognitive ability and mental status with no evidence of psychiatric or neuropsychological problems including post-traumatic amnesia. Five days following the incident, the patient was taken to the operating room by OMFS and Pediatric Dentistry. The right mandibular condyle was manually disimpacted from the right middle cranial fossa without any complication. Occlusion was reestablished with repeatable occlusion demonstrated. Intra-operative radiographs including lateral skull and Towne views were taken to verify the position of the condylar head. Pediatric Dentistry placed orthodontic bands on the maxillary and mandibular permanent first molars. Orthodontic brackets were placed on the maxillary and mandibular permanent central incisors and primary canines. Upper and lower stainless steel arch wires, and inter-arch stainless steel ligatures ties were placed for inter-maxillary fixation (IMF) (Figures 2a and 2b). A post-operative maxillofacial CT was taken and the position of condyle in the glenoid fossa was confirmed (Figure 3). Neurosurgery determined that no further surgical intervention was needed unless the patient became symptomatic indicating a neurological deficit. The patient was kept in the hospital for one day post operatively by Pediatric Trauma Surgery and was followed by OMFS. Post-operatively the patient had continuing headaches and blurred vision in the right eye and was evaluated further by Ophthalmology and Neurosurgery. From their perspective the patient’s complaints were consistent with underlying post-concussive symptoms with no changes in vision. At the patient’s one-week follow-up appointment with OMFS, the patient’s light wire fixation was changed to elastic fixation for three Volume 2 • Issue 7 • 049 Figure 3: Post-operative Coronal CT scan image showing the right condyle in correct position in relation to the glenoid fossa. weeks (Figure 2b). The patient was followed up on a weekly basis. At one month follow-up, the elastic fixation was removed. Orthodontic appliances were left affixed to the mixed dentition. Following release of the elastic traction, the patient had marked limited and painful opening with maximum incisal opening of five millimeters. The patient also continued to complain of occasional headaches, however the blurred vision had resolved. A maxillofacial CT was performed again and revealed bone like deposition around the condylar head, which appeared reactive in nature without gross displacement into the skull. Based on these findings possible hemarthrosis with subsequent ankylosis of the condyle was suspected (Figures 4a and 4b). Based on the clinical presentation and radiographic findings the patient was taken back to the operating room for manipulation of the TMJ under general anesthesia. On August 13th, 2013 the patient was evaluated intraoperative to ascertain the movement of the right condyle including translator movements. Following manual manipulation of the TMJ the patient was opened to 30 mm. After the patient was stabilized in Post Anesthesia Care Unit, she was discharged to home and followed-up as an outpatient. www.scientonline.org J Dent Oral Health Citation: Ida Anjomshoaa, Robert Pellecchia (2016). Alternative Management Approach of Dislocation and Hemarthroses of the Mandibular Condyle into the Middle Cranial Fossa in a Mixed Dentition: A Case Report and Review of the Literature Page 3 of 5 This may be due to underdeveloped medial and lateral poles of the condyle in younger patients [11,14,15]. Figure 4a: One month post-operative maxillofacial CT revealing bone-like deposition around the condylar head. Signs and symptoms during clinical presentation of patients with condyle displacement into the middle cranial fossa immediately following the injury are valuable diagnostic clues to ensure prompt identification and treatment of this injury. Common clinical presentations include facial asymmetry with chin deviation towards the affected side, malocclusion, trismus, anterior open bite, pain in the preauricular region, and cerebrospinal fluid leakage or bleeding from the ear on the injured side [10,11,13,14,16-19]. Neurological deficits can also manifest in these types of injuries including facial nerve injury, hearing loss and loss or altered state of consciousness [6,20-24]. For definitive diagnosis CT imaging has become the gold standard of imaging for this type of fracture11 .For optimal treatment many factors need to be considered on an individual basis including the patients age, treatment delay, extent of condyle displacement into the middle cranial fossa, neurological symptoms and involvement of adjacent vital structures including the middle meningeal artery, posterior cerebral artery, and dural tears [3,19]. Different treatment options have been presented based on these factors from closed to open reduction with or without reconstruction of the glenoid fossa. Figure 4b: Axial CT scan image revealing possible hemarthroses of the condyle. The patient began physical therapy after the second operation and progressed quite well without pain or significant restriction of motion with a stable occlusion. The patient was followed up inconsistently over seven months due to multiple broken appointments. In her last visit the orthodontic appliances were removed. Upon clinical examination the TMJ was non tender and without click or crepitus bilaterally with maximum mouth opening of more than 20 millimeters with mild deviation to the ipsilateral side. According to Kroertsch, et al. [14], closed reduction is a safer procedure as it minimizes neurological injury. They state that open reduction should be reserved for cases where other factors exist; such as if there has been a delay in the patient’s treatment and diagnosis, or closed reduction has failed. Neurological consultation is an important consideration as some patients may not initially present a neurological deficit but may develop deficits in a delayed manner. Similarly, in young children, closed reduction has been advocated for injuries that are diagnosed early within a four week post injury period where there is none urological deficit [10,11,13,17,22]. There are multiple factors that predispose a patient to displacement of the condyle into the middle cranial fossa, including the morphology of the condyle, such as a small and/or rounded condylar head [5,6]. Impact with an open mouth, unopposed posterior occlusion, temporal bone pneumatization, and congenital anomalies can all increase the risk of displacement of the condylar head into the middle cranial fossa [1,3,9-13]. In our case we chose to do closed reduction of the condyle and IMF utilizing orthodontic brackets. The patient did not have any neurological deficit and no significant fracture of the condylar itself. Of the reported cases of this injury in children with a mixed dentition no study was found to use orthodontic brackets to manage elastic IMF in the healing phase (Table 1). Our approach considers two important factors; one is the psychosocial aspect of using arch bars for IMF and secondarily the difficulty of placing arch bars in children with mixed dentition. Utilizing orthodontic brackets for IMF was much more feasible and acceptable to the patient and parent in this case. According to Rosa, et al. [13] there have been approximately 56 cases of displacement of the condyle into the middle cranial fossa with 37 of those cases reported in detail [13]. Of the reported cases there have been very few reports of this injury in young children with a mixed dentition (Table 1). Eleven cases of children under twelve years of age with intrusion of the intact condyle into the middle cranial fossa are represented in table. The case reports that involved fracture of the condyle itself was excluded in the table. Of the represented cases most were female with unilateral intrusion of the condyle. Eight cases (64%) were treated with closed reduction and the remaining three cases were treated with temporal craniotomy (Table 1). In general children and young adults have a higher tendency toward displacement of the condyle into the middle cranial fossa as compared to the elderly [14]. Some authors have suggested to reconstruct the glenoid fossa in order to prevent recurrence of displacement of the condyle back into the middle cranial fossa [14,15]. Defacianis, et al. [25], reported unsuccessful results ten days after an immediate closed reduction in a 6-year-old girl which led to open reduction and reconstruction of the glenoid fossa after seven months. However, the study did not disclose if there was a post-operative maxillofacial CT taken which would have indicated if the condyle had been successfully reduced in the first attempt, potentially eliminating the need for an open reduction procedure. In our case report the patient had no recurrences, and no problem with joint function or facial asymmetry. However, despite a short period of IMF as the initial management, a hemarthroses did develop [26,27]. Discussion Volume 2 • Issue 7 • 049 www.scientonline.org J Dent Oral Health Citation: Ida Anjomshoaa, Robert Pellecchia (2016). Alternative Management Approach of Dislocation and Hemarthroses of the Mandibular Condyle into the Middle Cranial Fossa in a Mixed Dentition: A Case Report and Review of the Literature Years Number of Unilateral Gender/ Mechanism days prior or Operation Age of Injury to surgical Bilateral intervention Authors Present Anjomshoaa et al case 2007 Magge et al. F/7 F/12 U Collided with another Immediate child Right frontotemporal craniotomy, reduction of condyle externally 30 with traction and stabilization with MMF yes NS 1 year NS Open reduction separating condylar neck and leaving none the head in middle cranial fossa no NS not reported Not reported Immediate Open reduction by temporal craniotomy 21 days and MMF yes no 6 months Deviation to the right on wide opening U Rosa et al. F/5 U 2005 Cilloet al M/7 U MVA and struck chin on the ground U MVA and struck chin on the window 2002 Barron et al. 2001 F/6 F/8 Defabianis et al F/6 Post Operation/ relapse Neurologic Follow-up deficit Closed reduction with MMF using orthodontic brackets,light wires and elastics 2006 Kroetsch et al. Glenoid Fossa reconstruction Fell off bicycle and 5 days struck her chin Possible MVA 3 years prior 2001 Duration of stabilization (days) Page 4 of 5 7 days in light wire and no 21 days in elastics no Mild deviation to the contralateral side 7 months Slight deviation of jaw to the right from loss of lateral pterygoid function MMF 14 days in MMF then 14 days in training elastics no no 24 months Slight deviation to the left, progressive facial asymmetry U Fell off bicycle and unknown struck her chin MMF 7 days no no 24 months Slight deviation 2mm to the right U Accidental fall during playing Closed reduction with MMF requiring 10 days secondary treatment with open reduction yes no 10 months Improvement in facial asymmetry, mouth opening and deviation Failed closed reduction with manipulative reduction secondarily used 14 days Fergusson gag between teeth on ipsilateralside of the injury with MMF and elastics no no 24 months Degenerative changes of condyle no no 10 months Minimal deviation 2 days Immediate 1990 Baldwin et al M/10 U Chin blow by an opponent's 1 day knee in a game 1989 Paulette et al F/11 U Fell off bicycle and 7 days struck her chin Closed reduction using towel clip with unknown MMF with wires and elastics Closed reduction using a molt mouth prop and secondary direct manual reduction with MMF 21 days in MMF then 14 days in training elastics no no 8 months Minimal deviation and slight resorption of condyle after 8 months Closed reduction with manipulation, no MMF N/A no no 18 months Mild deviation, progressive remodeling of the condyle 1985 Copernhaver et al F/9 U Fell off bicycle and 2 days struck her chin 1983 Ihalainen&Tasanen F/11 U Fell off bicycle and Immediate struck her chin F-female; M-male; U-unilateral; MVA-motor vehicle accident; MMF- maxillomandibularfixtion; NS-not stated; NA-not applicable. Table 1: Reported Cases of Intrusion of Intact Mandibular Condyle into the Middle Cranial Fossa for patients under age of 12. Conclusion Use of orthodontic appliances can provide a good alternative to conventional approaches for maxillomandibular fixation. Our conservative management was successful resulting in no relapse or Volume 2 • Issue 7 • 049 ankylosis of the condyle. However, a second procedure was required in this case due to patient non-compliance with physiotherapy. The use of orthodontic appliances affords clinicians options regarding elastic traction especially in the immediate post-traumatic www.scientonline.org J Dent Oral Health Citation: Ida Anjomshoaa, Robert Pellecchia (2016). Alternative Management Approach of Dislocation and Hemarthroses of the Mandibular Condyle into the Middle Cranial Fossa in a Mixed Dentition: A Case Report and Review of the Literature period. Arch bars in the mixed dentition are sometimes difficult to stabilize with compromise in maintaining adequate oral hygiene. For a child, orthodontic bracketing is a far more acceptable modality of treatment. The importance of long-term follow-up with clinical examination and CT imaging cannot be overstated particularly in children under age 10 as ankylosis and/or facial asymmetries are potential sequel following condylar injury in the growing patient [1]. Acknowledgements Alison E Gomez, DMD Resident, Pediatric Dentistry at Geisinger Medical Center 100 North Academy Ave, Danville, PA, 17822-1336 Karen Uston DDS, MS Page 5 of 5 Fracture of glenoid fossa and traumatic dislocation of mandibular condyle into middle cranial fossa. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93(6):640-642. 12.Stoltmann HF. Fracture dislocation of the temporomandibular joint: Report of two cases. J Neurosurg. 1965;22:100. 13.Rosa VL, Guimaraes AS, Marie SK. Intrusion of the mandibular condyle into the middle cranial fossa: case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(1):e4-7. 14.Koretsch LJ, Brook AL, Kader A, Eisig SB. Traumatic dislocation of the mandibular condyle into the middle cranial fossa: report of a case, review of the literature, and a proposal management protocol. J Oral Maxillofac Surg. 2001;59(1):88-94. 15.Cillo JE, Sinn DP, Ellis E. Traumatic dislocation of the mandibular condyle into the middle cranial fossa treated with immediate reconstruction: a case report. J Oral Maxillofac Surg. 2005;63(6):859-865. 16.Kallal RH, Gans BJ, Lagrotteria LB. Cranial dislocation of mandibular condyle. Oral Surg Oral Med Oral Pathol. 1977;43(1):2-10. Faculty at Geisinger Medical Center References 17.Ohura N, Ichioka S, Sudo T, Nakagawa M, Kumaido K, Nakatsuka T. Dislocation of the bilateral mandibular condyle into the middle cranial fossa: review of the literature and clinical experience. J Oral Maxillofac Surg. 2006;64(7):1165-1172. 1. Baldwin AJ. Superior dislocation of the intact mandibular condyle into the middle cranial fossa. J Oral Maxillofac Surg. 1990;48:623. 18.Seymour RL, Irby WB. Dislocation of the condyle into the middle cranial fossa. J Oral Surg. 1976;34:180. 2. Worthington P. Dislocation of the mandibular condyle into the temporal fossa. J Maxillofac Surg. 1982;10:24. 19.Sandler NA, Ozaki WH, Ochs MW, Marion DW. Intracranial reduction of an intact mandibular condyle displaced into the middle cranial fossa. J Oral Maxillofac Surg. 1996;54(4):506-510. 100 North Academy Ave, Danville, PA, 17822-1336 3. Copenhaver RH, Dennis MJ, Kloppedal E, Edwards DB, Scheffer RB. Fracture of the glenoid fossa and dislocation of the mandibular condyle into the middle cranial fossa. J Oral Maxillofac Surg. 1985;43(12):974-977. 4. Yoshii T, Hamamoto Y, Muraoka S, Teranobu O, Shigeta Y, Komori T. Traumatic dislocation of the mandibular condyle into the temporal fossa in a child. J Trauma. 2000;49(4):764-766. 5. de Fonseca GD. Experimental study on fractures of the mandibular condylar process (mandibular condylar process fractures). Int J Oral Surg. 1974;3(3):89-101. 20.Zachariades N. Glenoid fossa fracture and facial nerve palsy. Int J Oral Surg. 1985;14(6):564-566. 21.Tornes K, Lind O. Cranial dislocation of the mandibular condyle. A case report with unusual hearing loss. J Cranio Maxillofac Surg. 1995;23(5):302-304. 22.Melugin MB, Indresano AT, Clemens SP. Glenoid fossa fracture and condylar penetration into the middle cranial fossa: Report of a case and review of the literature. J Oral Maxillofac Surg. 1997;55(11):1342-1347. 6. Chuong R. Management of mandibular condyle penetration into the middle cranial fossa: case report. J Oral Maxillofac Surg. 1994;52(8):880-884. 23.Long X, Hu C, Zhao J, Li J, Zhang G. Superior dislocation of mandibular condyle into the middle cranial fossa. A case report. Int J Oral Maxillofac Surg. 1997;26(1):29-30. 7. Engevall S, Fischer K. Dislocation of the mandibular condyle into the middle cranial fossa: Review of the literature and report of a case. J Oral Maxillofac Surg. 1992;50:524. 24.Ihalainen U, Tasanen A. Central luxation or dislocation of the mandibular condyle into the middle cranial fossa. A case report and review of the literature. Int J Oral Surg. 1983;12(1):39-45. 8. Pepper L, Zide MF. Mandibular condyle fracture and dislocation into the middle cranial fossa. Int J Oral Surg. 1985;14(3):278-283. 25.DeFabianis P. Penetration of the mandibular condyle into the middle cranial fossa: Report of a case in a 6-year-old girl. J Clin Pediatr Dent. 2001;26(1):2935. 9. Musgrove BT. Dislocation of the mandibular condyle into the middle cranial fossa. Br J Oral Maxillofac Surg. 1986;24(1):22-27. 10.Barron RP, Kainulainen VT, Gusenbauer AW, Hollenberg R, Sandor, George KB. Management of traumatic dislocation of the mandibular condyle into the middle cranial fossa. J Can Dent Assoc. 2002;68(11):676-680. 11.Barron RP, Kainulainen VT, Gusenbauer AW, Hollenberg R, Sandor GK. 26.Magge SN, Chen HI, Heuer GG, Carrasco LR, Storm PB. Dislocation of the mandible into the middle cranial fossa. Case report. J Neurosurg. 2007;107(1 Suppl):75-78. 27.Paulette SW, Trop R, Webb MD, Nazif MM. Intrusion of the mandibular condyle into the middle cranial fossa: Report of a case in an 11-year-old girl. Pediatr Dent. 1989;11(1):68-71. Copyright: © 2016 Ida Anjomshoaa, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Volume 2 • Issue 7 • 049 www.scientonline.org J Dent Oral Health