Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
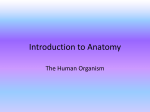
Lateral Decubitus Position Generates Discomfort and Worsens Lung Function in Chronic Heart Failure* Pietro Palermo, MD; Gaia Cattadori, MD; Maurizio Bussotti, MD; Anna Apostolo, MD; Mauro Contini, MD; and Piergiuseppe Agostoni, MD, PhD, FCCP Background: Lateral decubitus position is poorly tolerated by heart failure patients. Study objectives: To evaluated pulmonary function and lung diffusion in heart failure patients in the following five body positions: sitting, prone, supine, and left and right decubitus. Setting: Heart failure unit of a university hospital. Subjects: We studied 14 chronic heart failure patients in New York Heart Association class III and 14 healthy volunteers. Measurements and results: After 15 min of a selected position, subjects were evaluated by a discomfort scale, ear oximetry, and pulmonary function, which included FEV1, FVC, vital capacity (VC), alveolar volume, and diffusing capacity of the lung for carbon monoxide (DLCO) with subcomponent membrane resistance (DM) and capillary volume. In healthy subjects, we observed a reduction of DLCO and capillary volume in both lateral decubiti. Some discomfort was documented in both lateral decubiti when selected positions were compared with the sitting position. In the sitting position, pulmonary function suggested slight restriction ([mean ⴞ SD] FVC, 89.8 ⴞ 22.3% predicted; FEV1, 84.7 ⴞ 16.9% predicted, VC, 88.6 ⴞ 21.5% predicted; and FEV1/VC, 74 ⴞ 7) with low DLCO (73 ⴞ 19% predicted). Compared with sitting, lung mechanics were unchanged in prone and supine positions; FEV1, FVC, and FEV1/VC were lower when patients were lying on their side, with unchanged alveolar volume and VC. DLCO was similar when comparing sitting, prone, and supine positions, and it was lower in lateral decubitus because of the lower capillary volume (vs sitting) and DM (vs prone and supine). Body position-related FVC and DLCO reduction were greatest in the largest hearts (⌬FVC and ⌬DLCO vs left ventricle diastolic volume R ⴝ 0.524, p < 0.05 and R ⴝ 0.630, p < 0.02, respectively; ⌬FVC and ⌬DLCO vs cardiothoracic index R ⴝ 0.539, p < 0.05 and R ⴝ 0.685, p < 0.01, respectively). Conclusions: In heart failure, lateral decubitus airway obstruction and lung diffusion impairment become greater as heart dimensions increase. (CHEST 2005; 128:1511–1516) Key words: cardiomegaly; gravity; heart failure; lung diffusion; pulmonary function Abbreviations: Dlco ⫽ diffusing capacity of the lung for carbon monoxide; DM ⫽ membrane resistance; VC ⫽ vital capacity. t has frequently been observed that heart failure I patients report discomfort when lying on their side. It has also been shown1,2 that heart failure patients avoid the left lateral decubitus position during sleep. Although the idea that the heart can affect regional lung distension is nothing new,3 and the differences between erect, prone, and supine *From the Centro Cardiologico Monzino (Drs. Palermo, Cattadori, Bussotti, Apostolo, Contini, and Agostoni), Istituto di Ricovero e Cura a Carattere Scientifico, Institute of Cardiology, University of Milan, Milan, Italy; and Division of Respiratory and Critical Care Medicine (Dr. Agostoni), Department of Medicine, University of Washington, Seattle, WA. This study was supported by a Centro Cardiologico Monzino, Istituto di Ricovero e Cura a Carattere Scientifico research grant. www.chestjournal.org positions have been extensively studied in healthy subjects4 –7 and in patients with cardiac8 and lung9 diseases, to our knowledge, the effect of lying on one side, in terms of the mechanical properties of the lungs and of gas diffusion, has never been evaluated in heart failure patients. The present study was, Manuscript received April 23, 2004; revision accepted February 7, 2005. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (www.chestjournal. org/misc/reprints.shtml). Correspondence to: Piergiuseppe Agostoni, MD, FCCP, Centro Cardiologico Monzino, Istituto di Ricovero e Cura a Carattere Scientifico, Institute of Cardiology, University of Milan, 20138 Milan, Italy; e-mail: [email protected] CHEST / 128 / 3 / SEPTEMBER, 2005 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22030/ on 05/04/2017 1511 therefore, undertaken to assess whether the clinically reported complaints of breathing difficulties and/or general discomfort in the lateral position is associated with a difference in lung mechanics and gas diffusion in patients with chronic heart failure while in such body positions. Materials and Methods We studied 14 subjects with chronic severe heart failure (mean [⫾ SD] age, 62 ⫾ 8 years; one woman and 13 men) attributable to dilated cardiomiopathy. The study was carried out under stable clinical conditions with an optimized drug regimen for at least 2 months. Drug therapy included the following types: diuretics in all cases, -blocker in 12 of 14 cases, ACE-inhibitors in 7 cases, AT1 blockers in 6 cases, antialdosterone drugs in 12 cases, amiodarone in 8 cases, and digitalis in 2 cases. The etiology of dilated cardiomyopathy was coronary artery disease in eight cases and idiopathic cardiomiopathy in six cases. All of the patients were in New York Heart Association class III with a peak oxygen consumption of 14.4 mL/min/kg (⫾ 2.7; 50 ⫾ 11% predicted) and a ventilation/carbon dioxide production slope of 36 (⫾ 6). We also studied 14 healthy volunteers, recruited from hospital employees and friends (age, 61 ⫾ 8 years; 2 women and 12 men). Patient study inclusion criteria included a cardiothoracic index ⬎ 45% at chest radiograph and a left diastolic volume ⬎ 130 mL at echocardiography. Study exclusion criteria were as follows: (1) previous cardiac or thoracic surgery; (2) obesity defined as body mass index ⬎ 28; (3) presence of lung, pleural, chest wall, or muscular disease; and (4) presence of smoking history. The healthy subjects had a negative medical history, normal echocardiogram, and cardiopulmonary exercise test, and all of them were nonsmokers. The patients with heart failure had a chest radiograph for cardiothoracic index determination. This index was measured as the ratio of the transverse diameter of the heart in relation to the diameter of the thoracic cavity. Echocardiographic parameters were collected in all of the patients to determine left ventricle volumes and ejection fraction.10 We evaluated the standard pulmonary function, including FEV1, FVC, and vital capacity (VC), alveolar volume, and diffusing capacity of the lung for carbon monoxide (Dlco). To allow for measurements in the various body positions, a 30-cm rigid tube was inserted between the mouthpiece and the spirometer. This tube was used in all positions, as well as for instrument calibration. Morris et al11 prediction equations were used for FEV1 and FVC, and the equations of Crapo and Morris12 were used for Dlco. The alveolar volume was measured by using a standard single-breath technique with methane as an indiffusible gas. Dlco was measured with the single breath-constant expiratory flow technique (model 2200; SensorMedics; Yorba Linda, CA).13 Diffusion subcomponents, capillary volume, and membrane resistance (DM) were also measured by applying the method of Roughton and Forster.14 For this purpose, subjects inhaled gas mixtures containing 0.3% CH4 and 0.3% CO, with three different oxygen fractions equal to 20%, 40%, and 60%, respectively, and balanced with nitrogen. Ear oximetry was also recorded. Measurements were made on separate consecutive working days, while subjects were sitting, supine, prone, and recumbent on the left and right side. Patients remained in the selected position for 15 min before any measurements were taken. The order of the positions was random. We also evaluated subjects’ discomfort by asking how they felt in a specific body position when compared with the sitting position. The relative discomfort scale was numerical, from 1 to 5, with 3 being equal to the sitting position, 1 being much worse, 2 being slightly worse, 4 being slightly better, and 5 being much better. The discomfort evaluation was carried out immediately before the pulmonary function evaluation. With the exception of the chest radiograph, all of the control subjects underwent the same research protocol as the patients. Statistical Analysis Data were reported as the mean ⫾ SD. Comparisons between heart failure and healthy subjects were done in the sitting position by an unpaired t test. Comparisons within each group were made with the sitting position by a paired t test after an analysis of variance evaluation by applying the Bonferroni correction as needed (four comparisons). Correlations were evaluated by linear regression analysis. The discomfort scale is reported both in numerical values and in percentages and was statistically evaluated by a signed-rank test. Results All of the patients tolerated each study body position without major complaints. In the patient group, discomfort scale results relative to the sitting position showed an increase in discomfort in the left-side and right-side positions (p ⬍ 0.05; median, 3, 3, 2, and 2, respectively in prone, supine, left-side, and right-side positions). The percentage of distribution of the discomfort scale is reported in Table 1. The cardiothoracic index was 57.4 ⫾ 6.4%. Echocardiographic parameters revealed the following: left ventricular diastolic volume 220 ⫾ 81 mL, left ventricular systolic volume 152 ⫾ 72 mL, and left ventricular ejection fraction 33 ⫾ 7%. In the standard sitting position, pulmonary function tests suggested a slight restrictive disease as evidenced by the FVC, FEV1, VC, and FEV1/VC data (Table 2). No major changes were observed, in terms of lung mechanics (Table 2), among the sitting, prone, and supine positions. The FVC was greatest in sitting, prone, and supine position in seven, five, and two of the subjects, respectively; and FEV1 was greatest in sitting, prone, and supine position in eight, four, and two subjects, respectively. Compared with the sitting position, FEV1, FVC, and FEV1/VC were lower when patients were lying on one side, whereas the alveolar volume and VC were unchanged (Table 2). Table 1—Discomfort Scale Relative to Sitting Position* Discomfort Scale Position 1 2 3 4 5 Prone Supine Right decubitus Left decubitus 0 (0) 0 (0) 2 (14.3) 3 (21.4) 3 (21.4) 4 (28.6) 8 (57.1) 6 (42.9) 9 (64.3) 9 (64.3) 3 (21.4) 3 (21.4) 1 (7.1) 1 (7.1) 1 (7.1) 2 (14.3) 1 (7.1) 0 (0) 0 (0) 0 (0) *Values given as No. of patients and (% distribution). 1 ⫽ much worse; 2 ⫽ slightly worse; 3 ⫽ sitting position; 4 ⫽ slightly better; 5 ⫽ much better. 1512 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22030/ on 05/04/2017 Clinical Investigations Table 2—Pulmonary Function in Different Body Positions in Heart Failure Patients* Variables Sitting Prone Supine Right Side Left Side FEV1, L/s FEV1 % predicted FVC, L FVC % predicted VC, L VC % predicted FEV1/VC Alveolar volume, L Hb saturation, % 2.5 ⫾ 0.5 84.7 ⫾ 16.9 3.4 ⫾ 0.9 89.8 ⫾ 22.3 3.5 ⫾ 0.9 88.6 ⫾ 21.5 74 ⫾ 7 4.9 ⫾ 0.8 95.9 ⫾ 1.7 2.5 ⫾ 0.4 83.1 ⫾ 14.1 3.4 ⫾ 0.7 89.2 ⫾ 19.2 3.4 ⫾ 0.8 88.9 ⫾ 18.7 74 ⫾ 5 4.7 ⫾ 0.7 94.4 ⫾ 1.3 2.5 ⫾ 0.5 83.1 ⫾ 15.6 3.3 ⫾ 0.8 87.5 ⫾ 21.6 3.4 ⫾ 0.9 89.7 ⫾ 21.1 74 ⫾ 6 4.7 ⫾ 0.9 96.3 ⫾ 1.5 2.3 ⫾ 0.4† 76.3 ⫾ 13.0† 3.2 ⫾ 0.9† 84.5 ⫾ 22.2† 3.4 ⫾ 0.9 87.5 ⫾ 21.1 69 ⫾ 7† 4.7 ⫾ 0.7 95.7 ⫾ 1.6 2.4 ⫾ 0.5† 77.8 ⫾ 14.5† 3.2 ⫾ 0.8† 85.1 ⫾ 20.7† 3.4 ⫾ 0.9 88.1 ⫾ 21.4 69 ⫾ 7† 4.8 ⫾ 0.9 95.3 ⫾ 1.5 *Values given as mean ⫾ SD, unless otherwise indicated. Hb ⫽ hemoglobin. †p ⬍ 0.05 vs sitting position. Dlco was low in the standard sitting position and was 73 ⫾ 19% of the predicted value. On average, Dlco was similar when comparing the sitting, prone, and supine positions (Fig 1); the greatest Dlco value was observed as follows: while sitting, in eight subjects; while prone, in two subjects; and while supine, in four subjects. The capillary volume was lower in prone and supine positions when compared with sitting (Fig 2). Dlco was significantly lower with patients lying either on the left or the right side (Fig 1). This was attributable to a difference in capillary volume when comparing side positions with sitting and in DM when comparing side positions with prone or supine (Fig 2). On average, Dlco showed no difference between the left and right side, with the lowest Dlco measurements observed in nine and five of the patients, respectively on the left and right side. Ear oximetry was unaffected by the body position changes (Table 2). Compared with heart failure patients, healthy subjects had higher FEV1, FVC, VC, alveolar vol- ume, Dlco, and DM. In healthy subjects, body position changes did not generate any discomfort. Lung volumes and flows were unaffected by body position (Table 3). Dlco decreased when patients were lying on one side (Fig 1). This is attributable to a reduction in capillary volume (Fig 2). The body positions did not influence the hemoglobin oxygen saturation in healthy subjects (Table 3). We also evaluated the possibility (either by means of echocardiographic or radiograph measurements) that patients with the largest hearts were those with the greatest body position-related lung mechanics and Dlco changes. To do so, we correlated the maximal change (calculated as the difference between the greatest and the smallest value recorded of a selected parameter) with the left ventricle diastolic volume and cardiothoracic index. The correlation between FEV1 and FEV1/VC changes with both left ventricle diastolic diameter and the cardiothoracic index did not result in statistical significance (⌬FEV1 and FEV1/VC vs left ventricle diastolic volume: R ⫽ 0.218 with difference not significant and R ⫽ 0.229 with difference not significant, respectively; and ⌬FEV1 and FEV1/VC vs cardiothoracic index: R ⫽ 0.248 with difference not significant and R ⫽ ⫺0.219 with difference not significant, respectively). On the contrary, a significant correlation was observed with FVC and Dlco maximal body position-related changes, left ventricle diastolic volume, and the cardiothoracic index (Fig 3). No correlation was found between the Dlco changes and cardiac dimensions in the healthy subjects. Discussion Figure 1. Dlco in sitting, prone, supine, and right-side and left-side decubitus. White columns are heart failure patients and black columns are healthy individuals. * ⫽ p ⬍ 0.02 vs sitting. www.chestjournal.org In this study, the heart is viewed as a structure that occupies part of the intrathoracic space and that weighs differently on the lung in relation to body position.15,16 In congestive heart failure, the lungs are stiff and heavy, whereas the heart is large and heavy. As a consequence, the negative effects of CHEST / 128 / 3 / SEPTEMBER, 2005 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22030/ on 05/04/2017 1513 Figure 2. Lung diffusion for carbon monoxide subcomponents: DM and capillary volume in the five body positions evaluated. White columns are heart failure patients and black columns are healthy individuals. * ⫽ p ⬍ 0.02 vs sitting. lung-heart interdependence are increased.17 Indeed, it is known that, as the cardiac dimension increases, lung volume, mechanical function, and diffusion capacity decrease.18,19 Body position may influence the lung-heart interaction. Indeed, in healthy, young subjects, Dlco is higher in the supine position, when compared with the sitting position,6,5 because of an increase in capillary volume.6,7 In patients with ARDS, the prone position eliminates compression of the lung by the heart,9 and in heart failure patients, Dlco is similar in the sitting and supine positions with relevant interpatient variability.8 However, a systematic evaluation of the effects of body position on lung function in congestive heart failure patients has never been carried out. This evaluation is important, because heart failure patients often complain of difficulties when lying on one side.1,2 Furthermore, lung function, both lung mechanics and lung diffusion (which are impaired in heart failure), correlates with exercise capacity and prognosis.17,20 –22 The main finding of the present study is that, as a patient lies on one side, right or left, the lung function deteriorates, and the larger the heart, the greater the deterioration. In the sitting position, our findings were similar to those previously reported8,18 –23 for chronic congestive heart failure. Indeed, we observed data that is suggestive of a light restrictive syndrome with a reduction in Dlco. The prone and supine positions did not influence the lung mechanics as evaluated by FEV1, FVC, VC, or FEV1/VC in both the healthy subjects and the heart failure patients. Overall, Dlco was unchanged.8 However, when comparing patients in the sitting position, the capillary volume decreased in both the supine and prone positions. This observation has never been reported, and the physiologic reasons cannot be resolved by our study; however, a speculative hypothesis is tempting. Indeed, redistribution of lung fluids and changes in ventilation/perfusion relationship, attributable to gravity, are likely. In the sitting position, heart failure patients, because of their elevated pulmonary capil- Table 3—Pulmonary Function in Different Body Positions in Healthy Subjects* Variables Sitting Prone Supine Right Side Left Side FEV1, L/s FEV1, % predicted FVC, L FVC, % predicted VC, L VC, % predicted FEV1/VC Alveolar volume, L Hb saturation, % 3.8 ⫾ 0.8 114 ⫾ 11 4.8 ⫾ 0.9 119 ⫾ 11 5.0 ⫾ 1.0 116 ⫾ 16 75 ⫾ 8 7.1 ⫾ 1.1 96.1 ⫾ 1.0 3.7 ⫾ 0.7 110 ⫾ 14 4.8 ⫾ 0.9 115 ⫾ 13 4.9 ⫾ 0.9 113 ⫾ 14 75 ⫾ 8 6.8 ⫾ 1.2 95.1 ⫾ 2.1 3.6 ⫾ 0.7 109 ⫾ 11 4.8 ⫾ 0.8 115 ⫾ 11 4.8 ⫾ 0.9 112 ⫾ 14 76 ⫾ 8 6.9 ⫾ 1.2 95.2 ⫾ 1.0 3.6 ⫾ 0.7 108 ⫾ 13 4.7 ⫾ 0.9 114 ⫾ 13 4.9 ⫾ 0.9 113 ⫾ 13 74 ⫾ 8 7.1 ⫾ 1.2 96.3 ⫾ 0.9 3.6 ⫾ 0.7 109 ⫾ 12 4.8 ⫾ 0.8 116 ⫾ 12 4.9 ⫾ 0.9 114 ⫾ 14 74 ⫾ 6 7.1 ⫾ 1.3 95.5 ⫾ 0.7 *Values given as mean ⫾ SD, unless otherwise indicated. See Table 2 for abbreviation not used in the text. 1514 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22030/ on 05/04/2017 Clinical Investigations Figure 3. Correlation between lung diffusion (⌬Dlco) and FVC (⌬FVC) maximal change, calculated as the difference between the greatest and the smallest value recorded in a selected parameter vs the cardiothoracic index (CTI) and left ventricle diastolic volume (LVDV). lary pressure, have a better perfusion of the upper lobes with above-normal capillary volume.23 Contrarily, in the prone and supine positions, the gravitational effect is lower, and capillary volume is reduced. In healthy subjects, pulmonary vascular pressures are low, and no significant gravitationalrelated changes in capillary volume can be detected among the sitting, prone, and supine positions. Although heart failure patients complain about lying on one side (as often reported by patients and as quantified by our discomfort scale), a reduction in hemoglobin oxygen saturation was not observed. This is not surprising, considering that, at sea level, heart failure patients do not desaturate even during exercise, regardless of the low Dlco values.20,21 We have not consistently measured ventilation while patients were in the different positions, but a small increase in ventilation can easily be the compensatory mechanism that explains the finding of an unchanged hemoglobin saturation. Different from some previous reports,4 –7 we did not observe significant Dlco changes among sitting, supine, and prone positions in healthy subjects. This is likely attributable to differences in the age of subjects, ours being significantly older than subjects www.chestjournal.org in previous reports.6,7 We observed a significant reduction of Dlco in both lateral decubiti. This observation was unexpected and deserves some comment. Indeed, the observed Dlco reduction is attributable to capillary volume reduction without evidence of alveolar edema, given that DM is unchanged.24 It should be remembered that capillary volume is, as per the technique of Roughton and Forster,14 the amount of pulmonary blood, or, more precisely, of pulmonary blood flow, through the capillaries that participate in the exchange of gas and not the total amount of capillary volume. It is likely, therefore, that the reduction of capillary volume we observed in the lateral decubitus position is attributable to the deterioration of the ventilation/perfusion mismatch. The absence of alveolar edema formation24 concurs with the absence of discomfort in the lateral decubitus position. To answer the clinical question we have raised, that is, why patients with heart failure often complain of discomfort in the lateral decubitus position and not in the supine or prone position, it is important to compare data on the prone and supine positions with right-side or left-side decubitus and not with data on the sitting position. Indeed, no CHEST / 128 / 3 / SEPTEMBER, 2005 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22030/ on 05/04/2017 1515 major differences in the height of the thorax are present when comparing prone, supine, or lateral decubitus. Our observation suggests that, in the lateral decubitus, either left or right, the heart weighs on one lung, compressing both airways and lung parenchyma; indeed, the reduction of FEV1/VC with unchanged alveolar volume and VC is suggestive of the occurrence of some obstruction that, when patients were in a lateral decubitus position, is likely attributable to airway compression. Dlco, because of a DM reduction, was lower in the lateral positions; this is suggestive of some alveolar edema formation.24 The finding of a greater FVC and Dlco position-related reduction in the largest hearts (Fig 3) reinforces the concept of some body positiondetermined variability in the compressive forces of the heart on the lungs. The lack of a significant correlation between the amount of FEV1 positionrelated changes and heart dimension is likely because of the somewhat greater impairment of FEV1 vs FVC observed in the sitting, prone, or supine positions (Table 1). All of the above, for example, the parallel appearance of some airway obstruction and the reduction of Dlco, are the likely explanations for the clinically reported discomfort in the lateral positions. In conclusion, this study reports evidence of the frequently reported presence of discomfort in heart failure patients while lying on one side and shows the transitory occurrence of airways obstruction and, additionally, gas diffusion impairment in such body positions. References 1 Leung RST, Bowman ME, Peker JD, et al. Avoidance of the left lateral decubitus position during sleep in patients with heart failure: relationship to cardiac size and function. J Am Coll Cardiol 2003; 41:227–230 2 Miyamoto S, Fujita M, Sekiguchi H, et al. Effects of posture on cardiac autonomic nervous activity in patients with congestive heart failure. J Am Coll Cardiol 2001; 37:1788 –1793 3 Brookhart JM, Boyd TE. Local differences in intrathoracic pressure and their relation to cardiac filling pressure in the dog. Am J Physiol 1947; 148: 434 – 444 4 Sundröm G. Influence of body position on pulmonary diffusing capacity in young and old men. J Appl Physiol 1975; 38:418 – 423 5 Stam H, Kreuzer FA, Versprille A. Effect of lung volume and positional changes on pulmonary diffusing capacity and its components. J Appl Physiol 1991; 71:1477–1488 6 Chang SC, Chang HI, Liu SY, et al. Effects of body position and age on membrane diffusing capacity and pulmonary capillary blood volume. Chest 1992; 102:139 –142 7 Pistelli R, Fuso L, Muzzolon R, et al. Factors affecting variations in pulmonary diffusing capacity resulting from postural changes. Respiration 1991; 58:233–237 8 Faggiano P, D’Aloia A, Simoni P, et al. Effects of body position on the carbon monoxide diffusing capacity in patients with chronic heart failure: relation to hemodynamic changes. Cardiology 1998; 89:1–7 9 Albert RK, Hubmayr RD. The prone position eliminates compression of the lungs by the heart. Am J Respir Crit Care Med 2000; 161:1660 –1665 10 American Society of Echocardiography, Committee on Standards. Recommendations for quantification of the left ventricle by two-dimensional echocardiography. J Am Soc Echocardiogr 1989;2: 338 –367 11 Morris JF, Koski A, Johnson LC. Spirometric standards for healthy nonsmoking adults. Am Rev Respir Dis 1971; 103: 57– 67 12 Crapo RO, Morris AH. Standardized single breath normal values for carbon monoxide diffusing capacity. Am Rev Respir Dis 1981; 123:185–189 13 Huang YC, Helms MJ, MacIntyre NR. Normal values for single exhalation diffusing capacity and pulmonary capillary blood flow in sitting, supine positions, and during mild exercise. Chest 1994; 105:501–508 14 Roughton J, Forster RE. Relative importance of diffusion and chemical reaction rates in determining rate of exchange of gases in the human lung, with special reference to true diffusing capacity of pulmonary membrane and volume of blood in the lung capillaries. J Appl Physiol 1957; 11:290 –302 15 Butler J. The heart is in good hands. Circulation 1983; 67:1163–1168 16 Butler J. The heart is not always in good hands. Chest 1990; 97:453– 660 17 Agostoni PG, Marenzi GC, Sganzerla P, et al. Lung-heart interaction as a substrate for the improvement in exercise capacity after body fluid volume depletion in moderate congestive heart failure. Am J Cardiol 1995; 76:793–798 18 Hosenpud JD, Stibolt TA, Atwal K, et al. Abnormal pulmonary function specifically related to congestive heart failure: comparison of patients before and after cardiac transplantation. Am J Med 1990; 88:493– 496 19 Agostoni P, Cattadori G, Guazzi M, et al. Cardiomegaly as a possible cause of lung dysfunction in patients with heart failure. Am Heart J 2000; 140:E24 20 Wasserman K, Zhang YY, Gitt A, et al. Lung function and exercise gas exchange in chronic heart failure. Circulation 1997; 96:2221–2227 21 Agostoni PG, Bussotti M, Palermo P, et al. Does lung diffusion impairment affect exercise capacity in patients with heart failure? Heart 2002; 88:453– 459 22 Guazzi M, Pontone G, Brambilla R, et al. Alveolar– capillary membrane gas conductance: a novel prognostic indicator in chronic heart failure. Eur Heart J 2002; 23:467– 476 23 Puri S, Baker BL, Dutka DP, et al. Reduced alveolar-capillary membrane diffusing capacity in chronic heart failure: its pathophysiological relevance and relationship to exercise performance. Circulation 1995; 91:2769 –2774 24 Agostoni P, Cattadori G, Bianchi M, et al. Exercise-induced pulmonary edema in heart failure. Circulation 2003; 108: 2666 –2671 1516 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/22030/ on 05/04/2017 Clinical Investigations