Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
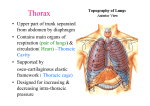
THORAX Cavity divided into: R+L pulmonary cavities: contain lungs and pleura Central mediastinum Superior thoracic aperture: 5x10cm Posterior: T1 Lateral: 1st ribs and costal cartilages Anterior: sup border of Manubrium Inferior thoracic aperture: Posterior: T12 Postlat: 11th and 12 ribs Ant lat: costal cartilages 7-10 (form subcostal angle) Anterior: xiphisternal joint Bony Characteristics True (vertebrocostal, 1-7) False (vertebrochondral, 8-10) Floating (vertebral, 11-12): do not articulate with transverse ligaments Head: 2 facets articulate with it’s vertebra and 1 above (except 1, 10, 11 which have only 1 facet); Costovertebral joints: synovial plane jt; demifacets separated by crest which attaches to IV disc by intra-articular ligament which separates into 2 synovial cavities; each joint surrounded by a capsule and anteriorly has radiate sternocostal ligament Tubercle: at junction of neck and body, have articular part which articulates with transverse costal facet of transverse process of vertebra at costotransverse joint (synovial plane jt, costotransverse, lat and sup CT ligs support); and nonarticular part for costotransverse ligament. Aperture of sup CT lig allows passage of spinal nerve and post branch of IC artery Body: internal surface has inf costal groove for intercostal nerves and vessels Costochondral joints: hyaline cartilaginous; no movement occurs at this joint Interchondral joints: plane synovial, strengthened by interchondral ligs; articulation between 9-10th ribs are fibrous 1st rib: only 1 facet, 2 grooves on sup surface – ant for subclavian vein, post for subclavian artery and brachial plexus - separated by scalene tubercle (attachment of scalenus ant muscle), behind post groove is attachment for scalenus medius; serratus ant attaches to lat aspect; no angle; has 1Y cartilaginous sternocostal joint 2nd rib: has tuberosity for serratus anterior, scalenus post also attached; has atypical synovial double cavity sternocostal joint 3-7 sternocostal joints are atypical synovial single cavity Costal cartilages 7-10 form costal margin Intercostal spaces named according to RIB ABOVE Space below 12th rib is subcostal space – subcostal nerve = ant rami T12 spinal nerve Vertebrae: sup and inf costal demifacets (except T1, 10-12); costal facets on transverse processes for articulation with tubercles of ribs Manubrium: has clavicular notches, below which is the syndochondrosis of 1st rib; jugular notch lies at inf border of T2, Manubrium at T3-4 – post is arch of aorta and merging of brachiocephalic veins to SVC (enters heart behind R 3rd costal cartilage; ½ facet for 2nd rib; manubriosternal junction is 2Y cartilaginous joint Sternum: 17cm; T5-9; costal notches up for 2-7th ribs; 3 transverse ridges mark fusion of sternal synchondroses at 3rd 4th and 5th articular depressions; sternal angle at T4-5 IV disc; ant to R heart; pec major and SCM attach to ant, sternohyoid and sternothyroid attach to posterior Xiphoid process: at T10; midline marker of sup aspect of liver; ½ facet for 7th rib; xiphisternal joint is 2Y cartilaginous, fuses by 40yrs Sternocostal joints: 1st is primary cartilaginous (syndochondrosis of 1 st rib), 2-7th is synovial plane (reinforced by radiate sternocostal ligs) Sternoclavicular: saddle type synovial; ant and post sternoclavicular and costoclavicular ligs; supplied by cervical plexus Manubriosternal: secondary cartilaginous Xiphisternal: primary cartilaginous; at T9; ossifies with age; costoxiphoid ligaments, diaphragm, transversis thoracis, linea alba and RA attach Note: domes of diaphragm rise to level of 4th ribs Females: smaller, sternum shorter, upper margin of sternum level with lower body T3 (males T2), upper ribs moveable Muscles of Chest Wall Serratus posterior sup: from nuchal lig, spinous processes C7-T3 sup borders 2nd-4th ribs; nerve = 2nd-5th IC nerves; action = elevate ribs Serratus posterior inf: from spinous processes T11-L2 inf borders 8th-12th ribs near angles; nerve = ant rami T9-12 thoracic spinal nerves; action = depress ribs Levator costarum: transverse processes T7-11 subjacent ribs between tubercle and angle; nerve = post rami C8-T11; action = elevate ribs Ex intercostal: inf border ribs sup border ribs; from tubercles of ribs to Costochondral junction where replaced by membrane; nerve = IC; action = elevate ribs in forced inspiration In intercostal: inf border ribs sup border ribs; from sternum to angle of rib then replaced by membrane; nerve = IC; action = depress/elevate ribs in forced expiration. Note innermost IC separated from in IC by IC nerves and vessels (pass 2 IC spaces) Subcostal: internal lower ribs near angles sup border ribs (2-3 below), running in same direction as in IC; nerve = IC; action = like in IC (pass 2 IC spaces) Transverse thoracic: post lower sternum internal costal cartilage; nerve = IC; action: weakly depress ribs Intercostal space: contains VAN from sup to inf Pectoral fascia: immediately post to breast Clavipectoral fascia: deep to above, suspended from clavicle Endothoracic fascia: deep to above, lines thoracic cage; becomes suprapleural membrane over apices Factoid: accessory muscles of inspiration: scalene, SCM, quadratus lumborum, erector spinae, pec major Accessory muscles of expiration: in TC, RA, ex oblique, in oblique, TA Upper ribs have pump-handle movement Nerves of Thoracic Wall Supplied by 12 thoracic nerves Ant rami: run in IC space; 12th forms subcostal nerve; run in endothoracic fascia between parietal pleura and in IC membrane in middle of IC space pass between innermost in IC and in IC, in costal groove; give rise to lat cutaneous branches (ant and post branches) at MAL, become ant cut branch (med and lat branches) near sternum. Also give off rami communicantes and collateral branches; collateral branches run along upper border of rib below Post rami: supply joint, skin and muscles of back NB: T1 gives sup branch to brachial plexus; 1st and 2nd IC nerves not in costal groove, but on in surface of ribs; 1st IC often doesn’t have ant or lat cut branches; 2nd IC nerve gives rise to large lat cut branch Intercostobrachial nerve and supplies axilla; 7-11th IC nerves form thoracoabdominal nerves Arteries of Thoracic Wall Thoracic Aorta: Subclavian Internal Thoracic: passes behind and just lat to sternum, divides into epigastric and musculophrenic arteries at 6th IC space; crossed near origins by phrenic nerve; runs ant to transverse thoracic muscle Anterior Intercostals: from internal thoracic (IC spaces 1-6, from subclavian) and musculophrenic arteries (IC spaces 7-9, from in thoracic); are paired; separated from parietal pleura by transverse thoracic muscle; supply IC’s, breast, skin, pecs; do not occur in lowest 2 IC spaces Supreme Intercostal Posterior Intercostals (IC spaces 1+2) Posterior Intercostals: R have longer course, pass post to oesophagus, thoracic duct, azygous vein; give off post branch which supplies spinal cord, vertebral column, back muscles and skin Subcostal Continuation of subclavian Axillary Superior Thoracic Lateral Thoracic Factoid: thoracoepigastric vein unites superior epigastric and lat thoracic veins, providing connection between IVC and SVC Nerves of Thoracic Wall Post IC veins azygous/hemiazgous venous system SVC (except 1st IC space, enter brachiocephalic vein directly); 2nd +3rd IC unite to form sup IC vein (R drains into azygous vein, L into brachicephalic) Lymphatic Drainage Above clavicles: to inf jugular LN’s Below clavicles: to axillary LN’s (from body wall and upper limb) Breasts From lat border of sternum to midaxillary line, from 2 nd to 6th ribs; nipple in 4th IC space lat to MCL; bed = pectoral fascia and fascia covering serratus anterior – covered by retromammary space (connective tissue). Tail of Spence extends along inflate edge of pec major towards armpit. Attached to dermis by extensory ligaments of Cooper which support mammary gland lobules. Lobules drained by lactiferous ducts which open onto nipple after a widened lactiferous sinus where milk stored. Also contain sebaceous glands. Blood supply: Subclavian internal thoracic ant IC branches Subclavian medial mammary branches Axillary lateral thoracic Axillary thoracoacromial Thoracic aorta post IC arteries Venous drainage: axillary and in thoracic vein Nerve: ant and lat branches of 4th-6th IC nerves Lymph: Nipple, areola and lobules subareolar lymphatic plexus lat breast to axillary (ant and pectoral) LN’s clavicular (infra and supra) LN’s subclavian lymphatic trunk med breast to parasternal LN’s bronchomediastinal lymphatic trunk inf breast to abdo LN’s (subdiaphragmatic inf phrenic LN) Skin axillary, inf deep cervical, infraclavicular, parasternal LN’s Bronchomediastinal and subclavian trunks join to form jugular trunk open into junction of in jugular and subclavian vein (venous angle) form brachiocephalic vein Lungs Pleura: serous pleural sac; split into costal (covered by endothoracic fascia), mediastinal, diaphragmatic (connected to diaphragm by phrenicopleural fascia) and cervical (extends 2-3cm above med 1/3 of clavicle; covered by suprapleural membrane) parts; inf to root of lung is pulmonary ligament where visceral meets parietal pleura ant to oesophagus; costodiaphragmatic and costomediastinal (L>R 2Y to cardiac notch in L lung) recesses; arteries from IC, int thoracic, musculophrenic, thymic, pericardiac and bronchial vessels Root of lung: bronchi, bronchial vessels, pul arteries, sup and inf pul veins, pul plexuses of nerves (sym, paraS, visceral afferent), lymphatic vessels; surrounded by pleural sleeve / mesopneumonium (meeting of parietal and visceral) Apex: extends above 1st rib NB. Lingula slides in and out of costomediastinal recess cardiac notch, with lingula inf Trachea: 9-15cm; supported by 16-20 C-shaped rings of hyaline cartilage; C6-T5; blood from inf thyroid and bronchial arteries, lymph to post/inf deep cervical; cricoid cartilage sits at sternal angle; carina is downward and backward projection of last cartilage; bifurcates at T4-5 moving on respiration but not swallowing behind sternal angle; elastic; blood from inf thyroid and bronchial arteries; lymph to post/inf deep cervical; nerves vagus and recurrent laryngeal for pain and secretomotor, sym to BV and SM R main bronchus: wider, shorter, runs more vertically, PA lies above then infront of it; enters lung at T5; azygous vein arches over from behind, R PA lies below in then infront of it, gives off branches to upper lobe L main bronchus: inf to arch of aorta, ant to thoracic aorta; enters lung at T6 lobar bronchi segmental bronchi terminal bronchioles resp bronchioles alveolar ducts pulmonary alveolus Carina lies to L of midline R sup bronchus is epartenol bronchus Bronchopulmonary segments: separated from adjacent segments by connective tissue septa, each supplied by own bronchi and artery (not vein) Sup lobe R Lung Apical Posterior Anterior Middle lobe Inferior lobe Lateral Medial Superior Anterior basal Medial basal Lateral basal Posterior basal Sup lobe Inferior lobe L lung Apical Posterior Anterior Superior Inferior Superior Anterior basal Medial basal Lateral basal Posterior basal Pulmonary trunk L+R pulmonary arteries at sternal angle give off 1st branch to sup lobe before entering hilum enter hilum descend postlat to bronchus divide into lobar and segmental arteries on ant aspect of corresponding bronchus Pulmonary veins L atrium Thoracic aorta L+R (may come from post IC) bronchial arteries pass along post aspect of bronchi. Supply up to resp bronchioles. Anastomose with pul arts distally. Bronchial veins: drain more prox part of lungs, otherwise drained by pul veins. Drain into R = azygous vein, L = accessory hemiazyous vein/L sup IC vein Bronchial arteries: 2 to L (from thoracic aorta), 1 to R (from either thoracic aorta or superior bronchial artery on L side) Lymph: Superficial lymphatic plexus lies deep to visceral pleura and drains lung parenchyma and visceral pleura bronchopulmonary LN’s sup and inf tracheobronchial LN’s (sup and inf to bifurcation of trachea and bronchi respectively) R+L bronchomediastinal lymph trunks terminate at venous angle (R may form lymphatic duct first, L may terminate in thoracic duct) Deep lymphatic plexus lies in submucosa of bronchi pulmonary LN’s bronchopulmonary LN’s Lymph from parietal pleura drains into intercostal, parasternal, mediastinal and phrenic LN’s Nerves: from pul plexuses ant and post to roots of lungs Paras: vagus nerve bronchoconstriction, vasoD, secretomotor Provide reflexive visceral afferent fibres – cough reflex, stretch reception, Hering-Bruer reflexes, pressor receptors, chemoreceptors Provide nociceptive impulses for trachea Sym: sympathetic trunk bronchiD, vasoC, decr secretion Provide nociceptive impulses for visceral pleura and bronchi Pleura supplied by IC nerves (mediastinal by phrenic) Sternal line of pleural reflection Meet at sternal angle (2), diverge at 4, R is parasternal at 6, MCL 8, MAL 10, 12 posteriorly (@ lat border erector spinae, under 12th costoverterbal angle) – all these are 2 levels inf to actual lung. Oblique fissure from spinous process of T3 6th CC Horizontal fissure from 4th rib anteriorly to 5th rib in MAL Factoid: RUL bronchi and blood supply separate from ML and LL prior to entering lung Mediastinum Arch of aorta Bifurcation of trachea Central tendon of diaphragm Lying Sup to transverse thoracic plane At transverse thoracic plane Xiphisternal junction / T9 Standing At transverse thoracic plane Inf to transverse thoracic plane Middle of xiphoid process / T9-10 IV disc Superior: From sup thoracic aperture to sternal angle/IV disc of T4-5 (transverse thoracic plane) Inferior: to diaphragm; T5-12; subdivided into ant, middle (ie. Pericardium) and post parts by pericardium Posterior: contains thoracic aorta, thoracic duct, lymphatic trunks, post mediastinal LN’s, azygous and hemizygous veins, oesophagus, oesophageal nerve plexus Anterior: between sternum and pericardium; continuous with sup mediastinum at sternal angle; contains connective tissue, fat, lymphatic vessels, LN’s, branches of in thoracic vessels Thymus: Primary lymphoid; Post to Manubrium Arterial supply: ant IC and ant mediastinal branches of in thoracic arteries Venous drainage: to L brachiocephalic, in thoracic, inf thyroid veins Lymph: parasternal, brachiocephalic, tracheobronchial Trachea: ant to oesophagus; slightly to R of midline; divides at sternal angle; terminates sup to heart; not component of post mediastinum; bifurcates at lower limit of sup mediastinum Oesophagus: lies to R of AofA post to pericardium and RA and LA deviates to L to pass through hiatus at T10 ant to aorta with ant and post vagal trunks, oesophageal branches of L gastric, lymphatic vessels; has 3 compressions – by AofA, L main bronchus, and diaphragm; thoracic duct lies to L, deep to AofA; nerve supply vagus (via recurrent laryngeal); blood from inf thyroid, aortic branches and L gastric (going downwards); lymph to deep cervical, mediastinal, gastric (going downwards); lower border of cricopharyngeus muscles is narrowest part of oesophagus, NOT DIAPHRAGM Thoracic duct: originates in chyle cistern @ L2, to R of aorta ascends through aortic hiatus ascends through post mediastinum AA: 2.5cm wide, 5cm long; only branches are coronary arteries from sinuses; intrapericardial; in middle mediastinus (INF to transverse thoracic plane) AofA: begins post to 2nd R sternocostal joint @ level of sternal angle, post to R auricle and PA ascends ant to pul art and bifurcation of trachea to upper 2nd R CC, post to pericardium and R pleura passes over root of L descends post to root of lung, on L of T4; ; ligamentum arteriosum (remnant of fetal ductus arteriosus) from root of L pul art to inf surface of AofA lung Note L phrenic and L vagus nerves in relation to L side of AofA; NB. Recurrent branch of L vagus; phrenic and vagus are separated by highest L intercostal vein Thoracic aorta: from post to 2nd L sternocostal jt, at L inf border T4 post to root L lung inf border T12 enters border through aortic hiatus; displaces oesophagus to R; surrounded by thoracic aortic plexus; thoracic duct and azygous vein on R side pass through aortic hiatus with it Branches: ant, unpaired, visceral: oesophageal Lat, paired, visceral: bronchial (R often come from 3rd R post IC artery) Postlat, paired, parietal – post IC arteries Also: sup phrenic, pericardial Brachiocephalic trunk: arises @ upper border R 2nd CC; ant to trachea, post to L BC vein, sternohyoid and sternothryoid; ascends on R of trachea R common carotid and subclavian; gives off thyroidea ima artery NB. R phrenic nerve lies on R L common carotid: arises post to Manubrium, post and to L of BC trunk ant to L subclavian, to L of trachea passes post to L SC joint; no branches in mediastinum L subclavian: arises from post AofA, post L common carotid passes post to L SC joint Brachiocephalic vein: formed by union of subclavian and in jugular veins @ level of 1 st CC; L >2x longer than R; R: R phrenic nerve on R of R brachiocephalic vein; branches include R vertebral, R in thoracic and R inf thyroid veins; L: passes ANTERIOR to roots coming from aorta; begin behind sternal end of L clavicle and passes behind Manubrium, sternohyoid and sternothyroid; branches include L vertebral, L in thoracic, L inf thyroid and L highest IC veins SVC: returns blood from all structures sup to diaphragm except lungs and heart; enters RA at 3 rd CC; lies antlat to trachea, postlat to ascending aorta; passes from sup to middle mediastinum; forms post boundary of transverse pericardial sinus; behind are root of R lung and R vagus nerve; receives azygous vein before piercing pericardium Azygous vein: drains back, mediastinal viscera and thoracoabdominal walls; begins opposite 1st-2nd lumbar vertebra by a branch from ascending lumbar/R renal/IVC passes through aortic hiatus passes on R side of bodies of inf 8 thoracic vertebrae arches over sup aspect of roof of R lung to join SVC; receives R subcostal and IC, hemiazygous, oesophageal, mediastinal and pericardial veins Hemiazygous vein: begins on L side in L ascending lumbar/renal vein enters thorax through L crus ascends on L side vertebral column post to thoracic aorta to T9 crosses to R, post to aorta, thoracic duct and oesophagus joins azygous vein; receives inf 3 post IC, inf oesophageal veins Vagus: descend postlat to common carotids enters sup mediastinum post to SC joint and BC vein pass POST to roots of lungs R: passes ant to R subclavian artery passes postinf on R of trachea post to R BC vein, SVC and root of R lung branches contribute to R pul plexus passes to oesophagus, forming oesophageal and deep cardiac plexus Gives rise to R recurrent laryngeal nerve which hooks under R subclavian artery ascends between trachea and oesophagus L: enters mediastinum between L common carotid and L subclavian passes post to AofA and root of L lung branches contribute to pul plexus oesophageal nerve plexus Gives rise to L recurrent laryngeal nerve which hooks under AofA lat to ligamentum arteriosum ascends in groove between trachea and oesophagus Phrenic: enter sup mediastinum between subclavian artery and origin of BC vein pass ANT to roots of lungs R: along R of BC vein, SVC and pericardium over RA descends on R of IVC to diaphragm pierces near caval opening L: crosses L surface of AofA ant to L vagus passes over L sup IC vein descends ant to root superficial to LA and LV pierces diaphragm Post mediastinal LN’s: post to pericardium and oesophagus; receive lymph from oesophagus, post pericardium and diaphragm, middle post IC spaces; R lymphatic/thoracic duct Thoracic sym trunks: lie against heads of ribs then Costovertebral joints then sides of vertebral bodies. Pericardium Fibrous pericardium is continuous with central tendon of diaphragm, tunica adventitia of great vessels (except IVC) at level of Manubriosternal joint; attached anteriorly to post surface of sternum by sup and inf sternopericardial ligaments (attach to Manubrium and xiphoid process) in L lower area of sternum and CC, otherwise covered anteriorly by pleura, posteriorly by loose connective tissue; lined with parietal layer; under this is visceral layer = epicardium; note IVC receives no covering from this layer; no adherent parietal pleura posteriorly where oesophagus contacts Aorta and pul artery are enclosed in arterial mesocardium; SVC, IVC and 4 pul veins enclosed in venous mesocardium. Between these is Oblique pericardial sinus: reflection of serous pericardium around great veins (permits pulsation of LA); and Transverse pericardial sinus: between aorta + pulmonary trunk / SVC, IVC, pul veins Artery: in thoracic pericardiacophrenic artery (accompanies phrenic nerve down lat side heart) musculophrenic artery (in thoracic) thoracic aorta bronchial, oesophageal, sup phrenic arteries Venous: pericardiacophrenic vein brachiocephalic vein Nerve: phrenic (pain), vagus, sympathetic trunk (vasomotor); visceral layer has no nerve supply Heart and Great Vessels Endocardium: endothelium and subendothelial connective tissue Myocardium: double helical orientation of fibres; outer spiral contracts to eject blood from ventricles; anchored to fibrous skeleton of heart forming 4 fibrous rings that surround valves; acts as insulator to ensure atria and ventricles contract separately Epicardium: mesothelium, formed by visceral pericardium Relations: anterior: sternum, CC’s, ant 3rd-5th ribs TURN HEAD TO L THEN UP A BIT – that’s how heart lies Ventricles separated by ant and post IV grooves Atria and ventricles separated by coronary / AV groove Base of heart is posterior aspect facing T6-9, is mostly L atrium; bounded below by coronary sulcus, above with bifurcation of pul artery; LV not involved Ant surface is mainly RV, upper by RA, strip of LV Diaphragmatic surface is 2/3 LV 1/3 RV, rests upon central tendon and L muscular diaphragm L border: LV and L auricle R border: RA only RA: R auricle increases capacity; smooth thin-walled post area (sinus venarum) on which SVC (@levels of 3 rd CC, has no valve), IVC (@level of 5th CC, has a valve) and coronary sinus (between AV orifice and IVC, has a valve) open; muscular ant wall of pectinate muscles – 2 areas separated exteriorly by sulcus terminalis and interiorly by crista terminalis, separates SVC and R auricle; fossa ovalis on interatrial septum is remnant of oval foramen RV: tapers into conus arteriosus pulmonary trunk; separated by supraventricular crest (directs flow towards pul trunk) from irregular muscular elevations (trabeculae carneae); Septomarginal trabeculae: muscular bundle from inf IVS of RV to base of ant papillary muscle, carries R branch of AV bundle LA: R+L (2 of each) pulmonary veins are valveless and enter post wall; wall of L auricle contains pectinate muscles; smooth walled apart from the auricle; semilunar depression is on other side of fossa ovalis, surrounding ridge is valve of oval fossa LV: walls mostly covered with trabeculae carnae (finer and more than R), conical cavity is longer than R, papillary muscles are larger than R; aortic vestibule leads to aortic orifice and valve; mitral valve has 2 cusps (ant and post) @ 4th CC which are smaller and thicker than tricuspid Ventricular septum: mostly muscular, but upper post part is membranous Tricuspid valve: at 4th-5th IC space; tendinous cords attach to free and ventricular edges of 3 cusps (anterior, posterior, septal/medial), arise from papillary muscles (anterior, attached to ant and post cusps; and posterior, attached to post and medial cusps) Mitral valve: 2 triangular cusps; larger and thicker than tricuspid; larger anterior, smaller posterior Semilunar valves: do not have tendinous cords; edge of each cusp is thickened (lunule), apex is thickened further at nodule Pulmonary valve: 3 cusps: anterior, R, L Aortic valve: 3 cusps, posterior, R, L; larger, thicker and stronger than pulmonary Coronary arteries: travel just deep to epicardium; supply myocardium and epicardium R arises from R aortic sinus (beginning of aorta), L arises from L aortic sinus pass around pulmonary trunk; 90% are R dominant RCA: supplies RA, RV, some LV, some IV septum, SAN and AVN Runs in coronary (AV) groove sinoatrial nodal branch (60%): supplies SAN and pul trunk R marginal branch: supplies RV and apex Continues to post side of heart AVN branch post IV branch (branches from circumflex in 15%; in post IV groove, supplies both V’s) LCA: supplies LA, LV, some RV, most IV septum Runs in coronary groove divides into 1) Circumflex branch – follows coronary groove to post surface of heart; supplies LA and LV L marginal branch (supplies LV) 2) L ant descending IV branch – passes along IV groove to apex; anastomosis with post IV branch in post heart; supplies both ventricles and IV septum lat (diagonal) branch Coronary sinus: runs from L to R in post coronary groove; receives great, middle and small cardiac veins, L post ventricular and L marginal veins Great cardiac: ascends in IV groove; drains areas supplied by LCA Middle and small cardiac: drain areas supplied by RCA Oblique vein: remnant of fetal L SVC Small ant veins: don’t drain into coronary sinus, drain into RA Lymph: pass to subepicardial lymphatic plexus through coronary groove inf tracheobronchial LN’s (usually on R) Conducting system: SAN: located deep to epicardium at junction of SVC and RA, near sup end of sulcus terminalis; supplied by SAN artery usually from RCA AVN: in postinf interatrial septum near opening of coronary sinus; supplied by AVN artery, from RCA in 80% AV bundle: transmits through fibrous skeleton of heart along membranous part of IVS; supplied by LCA Bundles of His: divide at junction of membranous and muscular septum; proceed on each side of muscular IVS deep to endocardium Subendocardial branches (Purkinje fibres): extend to ventricles RBB: to IVS, RV wall, ant papillary muscle, goes through septomarginal trabeculae (moderator band) LBB: 6 branches; to IVS, ant and post papillary muscles, wall of LV Nerve supply: cardiac plexus (superficial beneath AofA, deep between AofA and bifurcation of trachea and to R of ligamentum arteriosum) and pul trunk; deep is larger than superficial; receives vagal input Sym: cardiopulmonary splanchnic nerves (pain fibres accompany) ParaS: vagus Surface markings: Sup border: from inf border of 2 nd L CC to sup border 3rd R CC R border: from 3rd R CC to 6th R CC Inf border: to 5th IC space near MCL Aortic: at 3rd rib L sternal border auscultate at 2nd ICS L parasternal Pulmonary: 2nd ICS R parasternal Tricuspid: at top of xiphoid process auscultate at 5th L ICS Mitral: at 4th rib L sternal border auscultate at 5th L ICS, 6-10cm from AML