Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
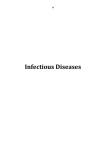
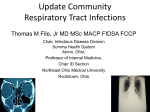
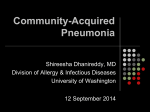
Treatment of Community-Acquired Pneumonia—IDSA Guidelines* Jack M. Bernstein, MD The Infectious Diseases Society of America (IDSA) has published guidelines for the treatment of community-acquired pneumonia (CAP). Although Streptococcus pneumoniae remains the most common etiologic agent, Chlamydia pneumoniae and Legionella pneumophila are also important causes. For all suspected CAP patients, particularly those requiring hospitalization, chest radiographs are strongly recommended to confirm the diagnosis. The IDSA guidelines, in contrast to those published by the American Thoracic Society, emphasize the use of sputum Gram’s stain and culture in all patients, whenever possible, to establish etiology. This information can be used not only to guide therapy but also to track trends in the etiologic pathogens for CAP and their antibiotic susceptibility. In light of the better outcomes with the earliest possible interventions, the IDSA recommends initial empiric antimicrobial therapy until laboratory results can be obtained to guide more specific therapy. Macrolides, doxycycline, and fluoroquinolones are suggested for primary empiric therapy, since each has activity against common bacterial pathogens and atypical agents. Detailed antibiotic recommendations are made for various pathogens. For inpatients, attempts should be made to cover Legionella and other common pathogenic bacteria. Alternative antibiotics are recommended for patients with structural diseases of the lung, penicillin allergy, or suspected aspiration pneumonia. Switch to an appropriate oral antibiotic is recommended as soon as the patient’s condition is stable and he or she can tolerate oral therapy, often within 72 h. (CHEST 1999; 115:9S–13S) Key words: American Thoracic Society guidelines; antibiotics; community-acquired pneumonia; empiric therapy; etiology; Infectious Diseases Society of America guidelines Abbreviations: ATS 5 American Thoracic Society; CAP 5 community-acquired pneumonia; IDSA 5 Infectious Diseases Society of America; SGS 5 sputum Gram’s stain understanding of community-acquired pneuO urmonia (CAP) has expanded greatly over the past several years. Epidemiologic studies show that the combined cause-of-death category of pneumonia and influenza ranks sixth as the leading cause of death in the United States.1 From 1979 to 1994, the crude rate of pneumonia and influenza has increased 59%. These increases weigh heavily on the elderly, who are more susceptible to these diseases and are more likely to die from them. The elderly accounted for 89% of all pneumonia and influenza deaths in 1992.2,3 Increasing death rates imply an increasing incidence within the community, but estimates are hard to obtain because CAP is not a reportable disease to state or federal agencies and is most often treated on *From the Department of Veterans Affairs Medical Center and the Department of Medicine/Veterans’ Affairs Campus, Wright State University, Dayton, OH. Correspondence to: Jack M. Bernstein, MD, Department of Medicine/Veterans’ Affairs Campus, Wright State University, PO Box 927, Dayton, OH 45435; e-mail: bernstein@wsu-id. dayton.oh.us an outpatient basis.4 Estimates for the incidence of CAP are 3.5 to 4 million cases per year, with up to 20% of patients requiring hospitalization.5 Those who enter the ICU suffer a 15 to 20% mortality rate. Etiologic Considerations Most CAP cases that yield an identifiable pathogen are caused by Streptococcus pneumoniae.6 Infection caused by aspiration of contents of the oropharynx may yield a variety of organisms. Although S pneumoniae accounts for a large portion of the pneumonias, culture reveals an expanding list of additional causes. Haemophilus influenzae and Chlamydia pneumoniae are generally the third or fourth most common organisms identified. Less common etiologic agents include oral anaerobes, Staphylococcus aureus, Legionella pneumophila, Moraxella catarrhalis, and Hantavirus (Table 1). However, 30 to 60% of the CAP cases do not yield an identifiable pathogen.7 When no pathogen is isolated, diagnosis rests on clinical criteria, none of which are definitive. The distribution of infective organisms varies in CHEST / 115 / 3 / MARCH, 1999 SUPPLEMENT Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21925/ on 05/04/2017 9S Table 1—Pathogens Typically Cultured From CAP Pathogen Prevalence, % S pneumoniae H influenzae Oral anaerobes S aureus Other Gram-negative bacteria Respiratory viruses L pneumophila C pneumoniae M catarrhalis 20–60 3–10 6–10 3–5 3–10 2–15 2–8 5–17 1–3 different age groups. Figure 1 shows examples of how the percentages of pathogens change with patient age. C pneumoniae is clearly an important pathogen for younger patients, whereas S pneumoniae grows in significance and Mycoplasma pneumoniae decreases for the elderly. L pneumophila, however, is most prevalent among the 35- to 49-yearold age group. Existing Guidelines for CAP The American Thoracic Society (ATS) and the Canadian Infectious Disease Society have provided guidelines to help the clinician treat CAP inpatients and outpatients.7,8 By providing criteria to stratify patients with the disease, these guidelines suggest when to hospitalize the patient and what courses of therapy may be useful. Patient stratification for outcome focuses on the severity of the disease and underlying risk factors for poor clinical outcome. The ATS guidelines stress the difficulty in acquiring specific etiologic information and emphasize instead empiric treatment of the disease. The ATS points out that the clinical presentations of patients infected with the same pathogen often differ. Furthermore, early chest radiographs may not show infiltrates or other signs of inflammation, and radiographs may not provide enough information to dif- Figure 1. Pathogens for CAP by age group.16 10S ferentiate bronchitis or chronic bronchitis from CAP.4,6 Attempts to clinch a diagnosis by culturing an organism often fail. Indeed, a study of 154 CAP patients using sputum culture, serologic tests, and bronchoscopy was able to identify the pathogen only 51% of the time.9 It is this type of result that prompted the ATS to recommend an empiric approach to CAP therapy.10 The IDSA Guidelines The Infectious Diseases Society of America (IDSA), which has recently reexamined the etiology and presentations of CAP, has proposed new guidelines that may lead to more efficient care for CAP patients.11 The guidelines seek to streamline decision making for patient care and to encourage ongoing attempts to identify the infecting organism. The objective is to rationalize antibiotic therapy so as to maximize the chance of cure and minimize the likelihood of inducing pathogen resistance. Figure 2 diagrams the recommended treatment algorithm, emphasizing inpatient management. Entry into the algorithm begins with a patient history consistent with CAP. This history could include such obvious considerations as cough, fever, and previous hospitalization for pneumonia. Additional contributing risk factors for CAP include viral infections, a compromised immune system, neutropenia, pulmonary edema, altered consciousness, airway obstruction, and congenital pulmonary abnormalities.4 At the outset, the IDSA guidelines strongly recommend a chest radiograph for all suspected CAP patients to confirm the presence of pneumonia. Radiographs are particularly valuable for CAP patients admitted to the hospital, because they provide Figure 2. Algorithm for CAP treatment. Adapted from IDSA.11 Emerging Resistance and Therapeutic Options Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21925/ on 05/04/2017 a baseline to assess the subsequent progression or regression of pulmonary inflammation. Clearly, patients with more CAP risk factors are subject to a higher risk of mortality. The IDSA algorithm helps define which patients would benefit from hospitalization. Clinical factors that are part of the decision include respiratory failure, ARDS, mechanical intervention, bilateral infiltrates or a . 50% increase in infiltrates, and a worsening chest radiograph within 48 h of hospital admission. Additional indicators of CAP severity include systolic or diastolic hypotension, profound sepsis with end-organ dysfunction, and tachypnea . 30 breaths/min. Although these factors can be part of patient assessment, the factors considered need not be this complex. Farr et al12 examined the prognostic power offered by 42 different measurable clinical factors for CAP patient outcome.12 They found that three parameters offered the clinician the best opportunity to predict patient mortality, specifically, tachypnea . 30 breaths/min, BUN . 19.6 mg/dL, and diastolic BP , 60 mm Hg. Diagnostic studies available for evaluating the CAP patient are summarized in Table 2. Baseline measurements include a chest radiograph, sputum Gram’s stain (SGS), and optionally, a sputum culture for conventional bacteria. Laboratory testing for inpatients should include a CBC count with differential and a chemistry panel including glucose, se- Table 2—Useful Diagnostic Studies for CAP Evaluation11 Studies Baseline assessment Chest radiograph to substantiate diagnosis of pneumonia, detect associated lung disease, provide a baseline to assess therapeutic response, predict pathogen, and assess severity Outpatients SGS is desired Culturing for conventional bacteria is optional Inpatients CBC count with differential Chemistry panel, including glucose, serum sodium, liver function tests, renal function tests, and electrolytes HIV serologic test with informed consent for persons age 15 to 54 years in hospitals with more than one newly diagnosed patient with HIV infection per 1,000 discharges Blood gases Blood cultures 3 2 (pretreatment) Gram’s stain and culture of sputum Test for M tuberculosis with acid-fast bacilli stain and culture in selected patients Test for Legionella in selected patients, including all seriously ill patients without an alternative diagnosis, especially if . 40 years old, immunocompromised, nonresponsive to b-lactam antibiotics, with clinical features suggesting this diagnosis, or in outbreak setting rum sodium, liver function, renal function, and electrolytes. In a hospital that sees more than one HIV-positive patient per 1,000 hospital discharges, an HIV serologic test should be run (with permission) for patients between the ages of 15 and 54 years. Seriously ill patients who lack an alternative diagnosis or have suggestive findings should also be tested for Mycobacterium tuberculosis and L pneumophila. The main difference between current ATS and IDSA guidelines lies in a greater emphasis by the IDSA on establishing the etiology for each case of pneumonia. The ATS views the relatively low information return from SGS and culture as a reason to forgo these tests. The IDSA, however, believes these etiologic tests not only help guide treatment in individual patients, but also provide an essential sampling of the community’s CAP patterns. Data from such tests allow detection of changes in the source of infection and resistance patterns among pathogens within the community. These samplings are not enough, however, to quickly detect newly emerging or resurgent infective organisms. The “Emerging Infections Network” on the IDSA Internet site (http://www.idsociety.org) provides a forum for the dissemination of information about the latest trends recognized by clinicians specializing in adult or pediatric infectious diseases.13 The Emerging Infections Network provides an early warning system for the Centers for Disease Control and Prevention and other public health agencies. The overall management goals of the IDSA guidelines pivot on the rational use of the microbiology laboratory for both inpatient and outpatient therapy. For outpatients, SGS is desirable, and culture for conventional bacteria is optional. Hospitalized patients should have an SGS and culture of both sputum and blood.11 Recommendations for therapy are pathogen directed. Hospitalization is based on the available prognostic criteria, and antibiotic therapy should begin as early as possible. Approximately 80% of CAP patients will be treated as outpatients. The IDSA guidelines call for a pathogen-directed therapy for these individuals as well. Diagnostic studies should include a chest radiograph and SGS. When the pathogen is unknown, empiric therapy should include considerations of disease severity, the patient’s age, clinical features, comorbidity, previous antibiotic therapy, and epidemiology. Options in Antimicrobial Therapy Options for antimicrobial therapy are continually evolving (Table 3). For empiric therapy, the IDSA CHEST / 115 / 3 / MARCH, 1999 SUPPLEMENT Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21925/ on 05/04/2017 11S Table 3—IDSA Therapeutic Alternatives for CAP11 Patient Category Outpatients Immunocompetent adults With suspected penicillin-resistant S pneumoniae With suspected aspiration Young adults (18 to 40 years) Hospitalized patients General medical ward ICU/serious pneumonia With structural lung disease With penicillin allergy With suspected aspiration Antimicrobial Recommendation Preferred: macrolide,* fluoroquinolone,† or doxycycline Alternatives: amoxicillin/clavulanate or second-generation cephalosporin (note: this regimen will not be active against atypical organisms) Fluoroquinolone† Amoxicillin/clavulanate Doxycycline Preferred: b-lactam‡ with or without macrolide,* or fluoroquinolone† Alternatives: cefuroxime with or without macrolide,* or azithromycin b-Lactam‡ with macrolide (erythromycin or azithromycin) or fluoroquinolone† Antipseudomonal penicillin, carbapenem, or cefepime with macrolide* or fluoroquinolone† with aminoglycoside Fluoroquinolone† with or without clindamycin Fluoroquinolone† with either clindamycin or metronidazole, or penicillin/b-lactamase inhibitor§ *Azithromycin, clarithromycin, or erythromycin. †Levofloxacin, sparfloxacin, grepafloxacin, trovafloxacin, or other fluoroquinolone with enhanced activity against S pneumoniae. ‡Cefotaxime, ceftriaxone, or a penicillin/b-lactamase inhibitor. §Ampicillin/sulbactam, ticarcillin/clavulanate, or piperacillin/tazobactam. recommends macrolides, doxycycline, and fluoroquinolones as suitable alternatives for primary therapy because each has activity against common pathogens as well as many atypical organisms. In serious cases of pneumonia (eg, in the ICU), the fluoroquinolones, erythromycin, or azithromycin should be supplemented with cefotaxime, ceftriaxone, or a b-lactam/b-lactamase inhibitor to provide extended Gram-negative coverage.11 Inpatient empiric therapy for particularly severe CAP should consider Legionella and other pathogenic bacteria as possible sources of the infection. The therapeutic program should be modified further for patients with structural disease of the lung, penicillin allergy, or suspected aspiration pneumonia. Recent studies have shown that patients can usually be switched from IV to oral therapy within 3 days, provided a good oral antibiotic is available and that the patient is in clinically stable condition and can tolerate the drug.14 Treatment for S pneumoniae should generally continue for 7 to 14 days or until the patient is afebrile for 72 h.11 Patients with atypical pathogens should be treated for 10 to 21 days. Azithromycin is a good choice for treatment of atypical pathogens, but its utility against S pneumoniae depends on community susceptibility. their conditions begin to deteriorate (Fig 3). When this happens, one must first question whether the initial diagnosis was correct.6 If the diagnosis was correct, then host issues, drug issues, or pathogen issues may be preventing a successful response. Host issues include obstruction, foreign bodies, inadequate immune response, or superinfection. Drug issues can include choosing the wrong drug, errors in dosage or administration routes, or an adverse drug reaction. Pathogen issues pivot on a correct identification of the pathogen, which may not be bacterial. Conclusions The recently published IDSA guidelines for the treatment of CAP cover essentially all aspects of When Patients Fail to Respond The expected response to antibiotic therapy is an amelioration of symptoms over the first 72 h. Some patients fail to respond to initial empiric therapy or 12S Figure 3. Causes for therapeutic failures.11 CHF 5 congestive heart failure. Emerging Resistance and Therapeutic Options Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21925/ on 05/04/2017 patient management. They begin with a strong recommendation for chest radiographs and utilize the hospitalization decision algorithm developed by Fine et al.15 Diagnostic studies are strongly encouraged, even for outpatients, to determine the etiology and allow pathogen-specific therapy. Antibiotic recommendations for initial empiric treatment are based on severity of illness and presence of risk factors. In addition, specific antibiotics are recommended for a wide range of pathogens, to assist in the switch from relatively broad-spectrum empiric therapy to specific therapy. Guidelines are presented to assist in the decision of when to switch from IV to oral therapy (often within 72 h), to determine the overall length of therapy, and to assess patient progress. Recommendations are made for the assessment of patients who fail to respond to initial treatment. Pneumococcal and influenza vaccines are recommended for those at high risk for CAP (ie, . 64 years of age and those with underlying systemic illness), consistent with current Centers for Disease Control and Prevention guidelines. The IDSA guidelines are presented with rankings to indicate the strength of each recommendation and the quality of the evidence supporting that recommendation. These guidelines are currently being integrated with the recently revised guidelines from the ATS to create a single set of recommendations for the treatment of CAP. Appendix/Discussion Dr. Bernstein: With regard to prompt initiation of therapy, there are data that show that the longer you delay the initiation of anti-infective therapy, the longer the hospital stay. This is the origin of the guideline for trying to initiate therapy in the emergency department. Dr. Segreti: One of the problems is what you consider “prompt” initiation of therapy. This obviously has medicolegal connotations. Dr. File: We actually suggested that anywhere from 2 to 8 h was “prompt” in an early draft of the guidelines, but the data to support the earlier number just were not there, so we took it out. The point was we wanted to make sure that prompt initiation occurred rather than waiting for the culture results. You should give the antibiotics as soon as possible. Dr. Bernstein: One quandary we face in empiric therapy is the increasing macrolide resistance in the community. Doxycycline still seems to be a reasonable drug, and the newer fluoroquinolones seem to be active against the majority of pathogens. I am reluctant to prescribe macrolides since with the increasing resistance we might start seeing failures. Dr. File: The issue here is that you need to have good local susceptibility data. If you use a macrolide empirically for a hospitalized patient, and the patient ends up with a pneumococcal bacteremia, you should be able to determine macrolide susceptibility in your laboratory if you are going to continue to use that drug. It really depends on good microbiology, and a lot of hospitals do not do that. References 1 US Dept of Commerce Bureau of the Census. Monthly vital statistics report. 1997; 45:21–24 2 CDC. Pneumonia and influenza death rates—United States, 1979 –1994. MMWR 1994; 44:535–537 3 Ely EW. Pneumonia in the elderly: diagnostic and therapeutic challenges. Infect Med 1997; 14:643– 654 4 Segreti J. Community-acquired pneumonia: new pathogens, new resistance patterns. Infect Med 1996; 13(suppl A):9 –14 5 Garibaldi RA. Epidemiology of community-acquired respiratory tract infections in adults. Am J Med 1985; 78(suppl 6B):32–37 6 Marrie TJ. Community-acquired pneumonia. Clin Infect Dis 1994; 18:501–515 7 Niederman MS, Bass JB Jr. Guidelines for the initial management of adults with community-acquired pneumonia: diagnosis, assessment of severity, and initial antimicrobial therapy: American Thoracic Society: Medical Section of the American Lung Association. Am Rev Respir Dis 1993; 148: 1418 –1426 8 Mandell LA, Niederman M. The Canadian communityacquired pneumonia consensus conference group. Can J Infect Dis 1993; 4:25–28 9 Bates JH, Campbell GD, Barron AL, et al. Microbial etiology of acute pneumonia in hospitalized patients. Chest 1992; 101:1005–1012 10 Gotfried M. CAP guidelines of the American Thoracic Society. Infect Med 1996; 13(suppl A):15–21 11 Bartlett JG, Breiman RF, Mandell LA, et al. Communityacquired pneumonia in adults: guidelines for management. Clin Infect Dis 1998; 26:811– 838 12 Farr BM, Sloman AJ, Fisch MJ. Predicting death in patients hospitalized for community-acquired pneumonia. Ann Intern Med 1991; 115:428 – 436 13 Executive Committee of the Infectious Diseases Society of America Emerging Infections Network. The emerging infections network: a new venture for the Infectious Diseases Society of America. Clin Infect Dis 1997; 25:34 –36 14 Ramirez JA, Srinath L, Ahkee S, et al. Early switch from intravenous to oral cephalosporins in the treatment of hospitalized patients with community-acquired pneumonia. Arch Intern Med 1995; 155:1273–1276 15 Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med 1997; 336:243–250 16 Marston BJ, Plouffe JF, File TM Jr. et al. Incidence of community-acquired pneumonia requiring hospitalization: results of a population-based active surveillance study in Ohio. Arch Intern Med 1997; 157:1709 –1718 CHEST / 115 / 3 / MARCH, 1999 SUPPLEMENT Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21925/ on 05/04/2017 13S