Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
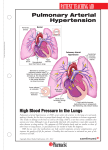
Pulmonary Arterial Hypertension (PAH) Pulmonary Arterial Hypertension (PAH) 1 Pulmonary Arterial Hypertension (PAH) Pulmonary Arterial Hypertension (PAH) Contents 2 1.Introduction 4 2. What is PAH? 5 3. Classification of PH 4. How common is PAH? 5. Why does PAH develop? 6. What are the symptoms of PAH? 6 8 8 10 7. How is PAH diagnosed? 8.Echocardiography – Value as a screening tool 9. Right heart catheterisation – The diagnostic gold standard for PAH 10 10. Screening for PAH 11. How is PAH treated? 12. Treatment guidelines – Goal-oriented therapy 16 13. The importance of early identification and intervention in PAH 14. Assessing the severity of PAH – Functional class – Exercise capacity – six minute walk test (6MWT) – Cardiopulmonary exercise testing – Haemodynamic parameters – Biochemical markers 15. PAH in patients with systemic sclerosis (SSc) – How is PAH-SSc detected? – How is PAH-SSc treated? 16.References 19 14 14 15 15 17 18 18 20 20 22 22 23 23 24 24 25 26 3 Pulmonary Arterial Hypertension (PAH) 1. Introduction 2. What is PAH? This brochure explains how pulmonary arterial hypertension (PAH) develops, describes the symptoms associated with the disease and outlines how it can be diagnosed and treated. Treatment is aimed at improving symptoms, exercise tolerance, long-term outcome and quality of life. Until the mid-1980s there were limited treatment options for patients and PAH was associated with poor prognosis. Today, treatment options have improved the prognosis for patients with this condition. Pulmonary arterial hypertension (PAH) is a progressive disease caused by narrowing or tightening (constriction) of the pulmonary arteries, which connect the right side of the heart to the lungs. By definition, PAH is characterised by an increase in mean pulmonary arterial pressure (PAP) to at least 25 mmHg at rest, and a mean pulmonary capillary wedge pressure (PCWP) of <15 mmHg.1,2 As PAH develops, blood flow through the pulmonary arteries is restricted and the right side of the heart becomes enlarged due to the increased strain of pumping blood through the lungs. It is this strain on the heart and the decrease in blood to the left heart and systemic circulation through the lungs that leads to the common symptoms of PAH, such as breathlessness, fatigue, weakness, angina, syncope, and abdominal distension.2 The increase in pulmonary vascular resistance observed in patients with PAH is related to a number of progressive changes in the pulmonary arterioles, including:2 •Vasoconstriction • Obstructive remodelling of the pulmonary blood vessel walls due to cell proliferation within the various layers of the vessel wall (smooth muscle cell and endothelial cell proliferation) •Inflammation • In situ thrombosis The most prominent histological feature of PAH is a thickening of the three cellular layers (the intima, media, and adventitia) that line the blood vessels, which is due to a process of cell enlargement termed hypertrophy. Other changes include development of plexiform lesions (focal proliferations of endothelial and smooth muscle cells that are a classic characteristic of PAH), and in situ thromboses (Figure 1). Figure 1. Histopathological features of PAH Intima Endothelium Media and smooth muscle Normal Collateral flux Plexifom lesion Adventitia Endothelial proliferation Intimal and medial thickening Intimal fibrosis Medial and smooth muscle cell hypertrophy In situ thrombosis Intimal fibrosis Intimal fibrosis and in situ thrombosis 4 Media Intimal fibrosis Direction of blood flow 5 Pulmonary Arterial Hypertension (PAH) 3. Classification of PH One of the more common forms of PAH is idiopathic PAH (IPAH), which corresponds to sporadic disease in which there is neither a family history of PAH nor an identified risk factor.3 Heritable PAH (HPAH) accounts for at least 6% of cases of PAH4 and mutations in the bone morphogenetic protein receptor 2 (BMPR2) have been identified in the majority of cases.5 PAH is also a rare side effect of certain anorexigenic agents, such as fenfluramine.2,3 However, the incidence of drug-induced PAH related to fenfluramine is decreasing as this agent is no longer available. Pulmonary arterial hypertension (PAH) represents Group 1 within the Pulmonary Hypertension World Health Organization (WHO) clinical classification system (Dana Point 2008) and is one of five such groups (Figure 2). The groups are divided based on aetiology.3 Figure 2. Classification of pulmonary hypertension Group 1 PAH can also be associated with a number of other conditions (associated PAH, APAH), which together account for most other cases. These conditions include:3 Pulmonary arterial hypertension (PAH) • Idiopathic (IPAH) PAH associated with connective tissue disease PAH is a well-recognised complication of connective tissue diseases, such as systemic sclerosis (SSc) and systemic lupus erythematosus (SLE). The prevalence of PAH has been well established only for patients with SSc.3 In recent studies, the prevalence of right heart catheterisation-confirmed PAH in patients with SSc was between 7% and 12%.6,7 PAH in patients with SSc is discussed in more detail later in this booklet. • Heritable (HPAH): – Bone morphogenetic protein receptor type 2 (BMPR2) – Activin receptor-like kinase 1 gene (ALK1), endoglin (with or without haemorrhagic telangiectasia) – Unknown • Drug- and toxin-induced • Associated with (APAH): PAH associated with HIV infection PAH is a rare but relatively well-documented complication of HIV infection with an estimated prevalence of around 0.5%.8 Highly active anti-retroviral therapy (HAART) has markedly improved survival rates in HIV patients, meaning long-term conditions such as PAH are increasingly responsible for HIV-associated morbidity and poor prognosis.9,10 – Connective tissue diseases – Human immunodeficiency virus (HIV) infection – Portal hypertension – Congenital heart disease (CHD) – Schistosomiasis – Chronic haemolytic anaemia PAH associated with portal hypertension PAH is a well-recognised complication of chronic liver diseases that develop as a result of portal hypertension (also called portopulmonary hypertension) and makes up around 10% of the PAH population.11,12 • Persistent pulmonary hypertension of the newborn (PPHN) Group 1’ Pulmonary veno-occlusive disease (PVOD) and/or pulmonary capillary haemangiomatosis (PCH) Group 2 Pulmonary hypertension due to left heart diseases • Systolic dysfunction PAH associated with congenital heart disease Congenital heart disease (CHD) is relatively common and affects around 1% of the population. Approximately 5–10% of adults with CHD will go on to develop PAH.13 The most severe form is Eisenmenger’s syndrome, which is associated with the reversal of an initial left-to-right shunt to a right-to-left shunt, causing cyanosis (a blue colouration of the skin due to low oxygen in the blood) and limited exercise capacity.3,14 Patients with PAH associated with CHD also include those with mild to moderate systemic-to-pulmonary shunts with no cyanosis at rest, patients with small defects, and those with residual PAH following corrective cardiac surgery.2,3 • Diastolic dysfunction • Valvular disease Group 3 Pulmonary hypertension due to lung diseases and/or hypoxemia • Chronic obstructive pulmonary disease (COPD) • Interstitial lung disease (ILD) • Other pulmonary diseases with mixed restrictive and obstructive pattern • Sleep-disordered breathing PAH associated with schistosomiasis Schistosomiasis is a parasitic disease caused by trematode flatworms of the genus Schistosoma. Patients with schistosomiasis and PAH can have the required specific clinical and pathological characteristics to be included in the APAH group. The prevalence of PAH in patients with schistosomiasis is around 4.6%.15 • Alveolar hypoventilation disorders • Chronic exposure to high altitude • Developmental abnormalities Group 4 Chronic thromboembolic pulmonary hypertension (CTEPH) Group 5 PH with unclear multifactorial mechanisms PAH associated with sickle cell disease The prevalence of PAH in patients with sickle cell disease is around 2–3.75%.16,17 • Haematological disorders: myeloproliferative disorders, splenectomy • Systemic disorders: sarcoidosis, pulmonary Langerhans cell histiocytosis, lymphangioleiomyomatosis, neurofibromatosis, vasculitis • Metabolic disorders: glycogen storage disease, Gaucher disease, thyroid disorders • Others: tumoural obstruction, fibrosing mediastinitis, chronic renal failure on dialysis 6 7 Pulmonary Arterial Hypertension (PAH) 4. How common is PAH? The role of endothelin Endothelin-1 (ET-1) is a vasoconstrictive protein produced by endothelial cells lining the blood vessels. High levels of endothelin are seen in patients with PAH due to various aetiologies24–26 and correlate with disease severity,27 resulting in a number of detrimental effects, primarily in the vasculature:23 Although PAH is a rare disease, with an overall estimated prevalence of 15–50 cases per million, the prevalence of PAH in certain at-risk groups (e.g. HIV-infected patients and patients with SSc) is substantially higher as discussed previously. 18 • Fibrosis • Hypertrophy and proliferation of cells, which can lead to thickening, narrowing, and occlusion of blood vessels • Inflammation • Vasoconstriction Idiopathic PAH (IPAH) has an annual incidence of 1–2 cases per million people in the US and Europe and is 2–4 times as common in women as in men.12,19 The mean age at diagnosis is around 45 years, although it can occur at any age.20 Despite the true relative prevalence of IPAH, heritable PAH (HPAH), and associated PAH (APAH) being unknown, it is likely that IPAH accounts for at least 40% of cases of PAH, with APAH accounting for most of the remaining cases.11 PAH associated with the newborn is known as persistent pulmonary hypertension of the newborn (PPHN). Severe PPHN has been estimated to occur in 0.2% of live-born term infants, and some degree of pulmonary hypertension complicates the course of more than 10% of all neonates with respiratory failure.21 ET-1 binds to two receptors, known as ETA and ETB. Both receptors are implicated in PAH and mediate the deleterious effects of endothelin.23 Endothelin receptor antagonism can either mitigate the effects of only one (single ETA antagonist) or both (dual ETA and ETB receptor antagonist) receptor types. Therapy with orally administered endothelin receptor antagonists (ERAs) that block the binding of endothelin to one or both receptors aims to mitigate the deleterious effects of the high levels of endothelin seen in PAH.28 Due to the non-specific nature of the symptoms, PAH is unfortunately most frequently diagnosed when patients have reached an advanced stage of disease (WHO Functional Class III and IV).11 The role of prostacyclin Prostacyclin is a potent vasodilator as well as an inhibitor of platelet activation.29 Patients with PAH have low levels of prostacyclin,29 which promotes vasoconstriction in the pulmonary vasculature and a tendency for smooth muscle cell proliferation and platelet activation.23 This may also encourage the formation of thrombi, which have been found in both the small distal pulmonary arteries and the proximal elastic pulmonary arteries.2 Therapy with prostacyclin or prostacyclin analogues can help to correct this deficiency, although administering this form of treatment may be complex due to the fact that some prostacyclins are broken down rapidly within the body; in most cases prostacyclins need to be given as a continuous intravenous or subcutaneous infusion or by inhalation.30 5. Why does PAH develop? The exact causes of the development of PAH remain unknown. However, research has led to a better understanding of underlying pathological mechanisms. PAH is recognised as a complex, multi-factorial condition involving numerous biochemical pathways and different cell types.2,22 Endothelial dysfunction, an abnormality of the inner lining of blood vessels, is believed to occur early in disease pathogenesis, and this leads to endothelial and smooth muscle cell proliferation followed by structural changes or remodelling of the pulmonary vascular bed, which in turn results in an increase in pulmonary vascular resistance. The role of nitric oxide Nitric oxide (NO) is an endothelial-derived substance that, like prostacyclin, is a potent vasodilator and also possesses anti-proliferative properties.30 Patients with PAH appear to produce insufficient NO, which could result in vasoconstriction within the pulmonary vasculature and a tendency for smooth muscle cell proliferation22,23 that may contribute to the development of PAH. The vasodilatory effect of NO is mediated by cGMP, which is rapidly degraded by phosphodiesterases (PDEs).23 Orally administered PDE-5 inhibitors reduce the degradation of cGMP and so promote the accumulation of intracellular cGMP, enhancing NO-mediated vasodilatation.31 Vascular remodelling itself involves every layer of the vessel wall and is characterised by proliferative and obstructive changes involving many cell types; including endothelial cells, smooth muscle cells, and fibroblasts.2 Inflammatory cells and platelets may also play a significant role in PAH. Endothelial dysfunction results in chronically impaired production of vasoactive mediators, such as nitric oxide (NO) and prostacyclin, along with prolonged overexpression of vasoconstrictors, such as endothelin-1 (ET-1), which not only affect vascular tone but also promote vascular remodelling. These substances are important therapeutic targets for new treatment options in PAH.2,23 8 9 Pulmonary Arterial Hypertension (PAH) 6. What are the symptoms of PAH? Figure 3. ACCF/AHA diagnostic approach to PAH22 Pivotal Tests Changes to the pulmonary vasculature lead to the typical symptoms of PAH. The symptoms are caused by the high resistance to blood flow through the lungs, which results in increased stress on the heart. This can severely impact a patient’s ability to exercise or carry out normal daily activities. Common early symptoms include:2,19,32 Contingent Tests History Exam • Index of suspicion • of PH CXR • Breathlessness (dyspnoea), particularly during physical activity • Fatigue • Dizziness • Syncope, also on physical activity (rare) • Peripheral oedema • Chest pain, again particularly during physical activity Contribute to Assessment of: ECG TEE Echocardiogram Exercise Echo • RVE, RAE, RVSP, RV • Function • Left Heart Disease • VHD, CHD Pulmonary Angiography VQ Scan Chest CT Angiogram • Chronic PE Coagulopathy Profile The symptoms may not be obvious at first and are often attributed to more common conditions. Over time, however, they can become more severe and begin to limit normal activities. As the disease progresses, some patients may experience constant dyspnoea and fatigue so that even simple tasks, such as getting dressed and walking short distances, become difficult. As the early symptoms of PAH are often mild, time from symptom onset to disease diagnosis is estimated to be more than 2 years.11,12 This means that PAH is frequently not recognised until the disease is relatively advanced.11,19 PFTs ABGs Overnight Oximetry Polysomnography Other CTD Serologies LFTs 7. How is PAH diagnosed? • Scleroderma, SLE, RA • Portopulmonary Htn Functional Test (6MWT, CPET) PAH is a challenging disease to diagnose accurately. It requires invasive investigations and significant experience to manage patients effectively. As such, current guidelines recommend that the diagnosis and management of PAH is co-ordinated by expert centres (dependent on regional variations).2,33 • Sleep Disorder • HIV Infection HIV ANA • Ventilatory Function • Gas Exchange • Establish Baseline • Prognosis Vasodilator Test RH Cath Exercise RH Cath Volume Loading • Confirmation of PAH • Haemodynamic Profile • Vasodilator Response Left Heart Cath Once a suspicion of PAH has been raised, the aim is to confirm or exclude the diagnosis of pulmonary hypertension (PH) and, if present, establish its aetiology, assess disease severity, as well as to decide on subsequent management and treatment strategies. The non-specific nature of symptoms associated with PAH means that the diagnosis cannot be made on symptoms alone. The diagnosis of PAH involves a series of investigations to determine whether there is a likelihood of PAH being present, to confirm the diagnosis based on initial non-invasive testing, to clarify the specific aetiology, to evaluate the functional and haemodynamic impairment of the individual patient, and to determine an appropriate treatment category.2,22 These diagnostic steps have been formalised into clinical practice guidelines for the diagnosis of PAH, both in the US (Figure 3)22 and Europe (Figure 4).2 6MWT, 6-minute walk test; ABGs, arterial blood gases; ANA, antinuclear antibodies; CHD, congenital heart disease; CPET, cardiopulmo6MWT, 6-minute walk test; ABGs, arterial blood gases; ANA, antinuclear antibodies; CHD, congenital heart disease; CPET, cardiopulmonary nary exercise test; CT, computerised tomography; CTD, connective tissue disease; exercise test; CT, computerised tomography; CTD, connective tissue disease;CXR, chest x-ray; ECG, electrocardiogram; HIV, human CXR, chest x-ray; ECG, electrocardiogram; HIV, human immunodeficiency virus screening; Htn, hypertension; LFT, liver function test; PE, immunodeficiency virus screening; Htn, hypertension; LFT, liver function test; PE, pulmonary embolism; PFT, pulmonary function test; PH, pulmonary embolism; PFT, pulmonary function test; PH, pulmonary hypertension; pulmonary hypertension; RA, rheumatoid arthritis; RAE, right atrial enlargement; RH Cath, right heart catheterisation; RVE, right ventricular RA, rheumatoid arthritis; RAE, right atrial enlargement; RH Cath, right heart catheterisation; RVE, right ventricular enlargement; RVSP, right enlargement; RVSP, right ventricular systolic pressure; SLE, systemic lupus erythematosus;TEE, transoesophageal echocardiography; VHD, ventricular systolic pressure; SLE, systemic lupus erythematosus; valvular heart disease; VQ Scan, ventilation-perfusion scintigram. TEE, transoesophageal echocardiography; VHD, valvular heart disease; VQ Scan, ventilation-perfusion scintigram. Adapted with permission of Wolters Kluwer Health, from ACCF/AHA. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association, McLaughlin VV, Archer SL, Badesch DB, et al. Circulation 119:2250–94 Copyright © 2009, permission conveyed through Copyright Clearance Center, Inc. Interpretation of the results of tests is complex and requires substantial experience in the management and follow-up of PAH patients. 10 11 Pulmonary Arterial Hypertension (PAH) Diagnosis of PAH Figure 4. ESC/ERS clinical guidelines for the diagnosis of PAH2 The diagnosis process can be summarised in four general stages as described below. However, the type of tests used may vary between centres, depending on the individual circumstances and the needs of the patient. Symptoms/signs/history suggestive of PH Non-invasive assessment compatible with PH? YES Search for other causes and/or re-check 1.Clinical suspicion of PAH • Exertional dyspnoea, syncope, angina, and/or progressive limitation of exercise capacity without apparent risk factors, symptoms, or signs of common cardiovascular and respiratory disorders • Patients with associated conditions and/or risk factors (e.g. family history, connective tissue diseases, HIV) NO Consider common causes of PH Group 2: Left heart disease? Group 3: Lung diseases and/or hypoxia? History, Symptoms, Signs ECG, Chest radiograph TTE, PFT, HRCT 2.Exclusion of Group 2 (left heart disease) and Group 3 (lung diseases) • Clinical history, electrocardiogram (ECG), chest radiograph, transthoracic echocardiogram, pulmonary function tests, and high-resolution computed tomography (HRCT) of the chest are requested in order to identify the presence of Group 2 (left heart disease) or Group 3 (lung diseases) Group 2 or 3: diagnosis confirmed YES PH “proportionate” to serverity NO YES “out of proportion” PH Treat underlying disease and check for progression Perform V/Q scan Search for other causes Segmental perfusion defects Consider Group 4: CTEPH 3.Exclusion of Group 4 • If PH Groups 2 or 3 are not found, less common causes of PH should be looked for. For example, ventilation/perfusion lung scan is used to exclude Group 4 chronic thromboembolic pulmonary hypertension (CTEPH) NO 4.PAH evaluation and characterisation (type, functional class, haemodynamics) • A range of other tests can be performed to refine the final diagnosis, including CT pulmonary angiography, cardiac magnetic resonance imaging, haematology, biochemistry, immunology, serology, and ultrasonography • The diagnostic gold standard for the confirmation of a diagnosis of PAH is right heart catheterisation (RHC) • The degree of limitation to the patient caused by PAH is assessed by determining functional class and by exercise tests such as the six-minute walk test (6MWT). This gives both a baseline measure against which to assess progression or response to treatment, and provides prognostic information NO Consider other uncommon causes YES Consider PVOD/PCH Perform RHC (PAH probability*) mPAP ≥ 25 mm Hg PWP ≤ 15 mm Hg YES Specific diagnostic tests Physical, Laboratory analysis Clinical signs HRCT, ANA PVOD PCH History CTD HIV Test Drugs Toxins HIV TTE, TEE, CMR Physical, US, LFT CHD Idiopathic or Heritable PAH Schistosomiasis Other group 5 Chronic Haemolysis PortoPulmonary BMPR2, ALKI, Endoglin (HHT) Family history ALK-1, activin-receptor-like kinase; ANA, antinuclear antibodies; BMPR2, bone morphogenetic protein receptor 2; CHD, congenital heart ALK-1, activin-receptor-like ANA,CTD, antinuclear antibodies; BMPR2, Group, bone morphogenetic protein receptorhaemorrhagic 2; CHD, disease; CMR, cardiac magnetickinase; resonance; connective tissue disease; clinical group; HHT, hereditary congenital heart disease; CMR, cardiac magnetic resonance; CTD, connective tissue disease; Group, clinical group; HHT,, mean telangiectasia; HIV, human immunodeficiency virus; HRCT, high resolution computed tomography; LFT, liver function test; mPAP hereditary telangiectasia; HIV, human immunodeficiency virus; capillary HRCT, high resolution computed LFT, pulmonary arteryhaemorrhagic pressure; PAH, pulmonary arterial hypertension; PCH, pulmonary haemangiomatosis; PFT, tomography; pulmonary function liverpulmonary function test; mPAP, mean pulmonary arteryveno-occlusive pressure; PAH, disease; pulmonary arterial hypertension; pulmonary capillary test; PH, hypertension; PVOD, pulmonary PWP , pulmonary wedge PCH, pressure; RHC, right heart haemangiomatosis; PFT, pulmonary function test; PH, TTE, pulmonary hypertension; PVOD, pulmonary veno-occlusive V/Q disease; catheterisation; TEE, transoesophageal echocardiography; transthoracic echocardiography; US, ultrasonography; Scan,PWP, pulmonary wedge pressure; RHC, right heart catheterisation; TEE, transoesophageal echocardiography; TTE, transthoracic ventilation/perfusion lung scan. echocardiography; US, ultrasonography; V/Q Scan, ventilation/perfusion lung scan. Adapted with permission of Oxford University Press, from Guidelines for the diagnosis and treatment of pulmonary hypertension, Galiè N, Hoeper MM, Humbert H, et al. Eur Heart J 2009;30:2493–537 Copyright © 2009, permission conveyed through Copyright Clearance Center, Inc. 12 13 Pulmonary Arterial Hypertension (PAH) 8. Echocardiography 9. Right heart catheterisation Value as a screening tool The diagnostic gold standard for PAH Transthoracic Doppler echocardiography (TTE) is a non-invasive screening test for pulmonary hypertension.34 Pulmonary arterial pressure can be estimated from the tricuspid regurgitant (TR) jet measured by TTE (Figure 5) and a range of other measurements can be obtained which provide information about the cause and consequences of PH. Right heart catheterisation (RHC) is required for a definitive diagnosis of PAH (Figures 6 and 7),2,34 to assess the severity of haemodynamic impairment, and to test the vasoreactivity of the pulmonary circulation. PAH is defined as a sustained elevation of mean pulmonary arterial pressure (mPAP) to >25 mmHg at rest, and a mean pulmonary capillary wedge pressure (PCWP) of <15 mmHg.1,2 Figure 5. Echocardiography in PAH Figure 6. Right heart catheterisation2 Internal jugular vein Right heart catheterisation is required to confirm the diagnosis of PAH. Tricuspid regurgitation (TR) Pulmonary artery Left lung PAH is defined by ● mPAP ≥25 mmHg at rest LA Right ventricle Brachial vein ● PCWP ≤15 mmHg RA RV LV Femoral vein TR jet velocity (v) Standard approaches for catheter access Galié et al. Eur Heart J 2009. Syst PAP = Right ventricular systolic pressure Right heart catheterization Figure 7. Right heart catheterisation34 (in absence of pulmonary outflow obstruction) RVSP = 4v2 + RAP* Catheter Aorta Characteristic intracardiac pressure waveforms during passage through the heart Pulmonary artery *ESC guidelines. Eur Heart J 2004. Left atrium RA RV PA PCW 40 mmHg 20 Superior vena cava Right atrium Pulmonary valve Tricuspid valve Inferior vena cava 14 Right ventricle Left ventricle 15 Pulmonary Arterial Hypertension (PAH) 10. Screening for PAH 11. How is PAH treated? Early diagnosis and therapeutic intervention may offer an improved outlook for patients with PAH. One method of improving early diagnosis is the introduction of screening programmes for high-risk patient populations. These programmes screen patients for the presence of PAH while they are not showing obvious symptoms. While there is currently no cure for the disease, modern advanced PAH therapies can markedly improve a patient’s symptoms and slow the rate of clinical deterioration.2,37 The aims of treatment in patients with PAH are several-fold and range from symptomatic relief to improvement in the physical limitations imposed by their disease (such as improving functional class; see section: Assessing the severity of PAH), and delaying disease progression.2,33 High-risk patient populations are those patients with conditions known to be associated with a high risk of developing PAH, including: The management of PAH is complex and involves the use of a range of treatment options, which can be broadly broken down into four main categories: • Family members of a patient with heritable pulmonary arterial hypertension (HPAH) • Patients with systemic sclerosis (SSc) • Patients with HIV • Patients with portopulmonary hypertension (PoPH) • Patients with congenital heart disease 1. General measures aim to limit any potentially deleterious effects of the patient’s external circumstances on their PAH disease, and include avoiding pregnancy, prevention and prompt treatment of chest infections, and awareness of the potential effects of altitude.2,22,38 2. Conventional or supportive therapy aims to provide symptomatic benefit; however, there is no evidence that it has an effect on the disease process or prognosis. Such measures include supplemental oxygen, oral anticoagulants, diuretics, and calcium channel blockers.2,22,38 For example, results from a PAH registry in France, which aimed to describe the clinical and haemodynamic characteristics of patients with PAH and which included 674 consecutive patients from 17 different centres, showed that without screening the majority of patients were diagnosed in WHO FC III or IV, and only 24% of patients were in the less severe WHO FC II (Figure 8).11 The US REVEAL registry was established to define the characteristics of patients with PAH and their management in current practice, with the aim of helping to improve diagnosis, treatment and management.12 Data from REVEAL was recently used to validate a quantitative algorithm for predicting survival and to develop a simplified calculator for everyday clinical use. In this study, of 504 patients newly diagnosed with PAH enrolled in the registry, over 60% were in functional class III.35 However, PAH was detected at an earlier stage during a national screening program in a high-risk population (Figure 8), demonstrating the potential value of a screening strategy.6 3. Advanced therapy (also termed PAH-specific therapy) PAH-specific therapies have been developed to target one of three major pathways known to be involved in the development of PAH23 and have, to varying degrees, been shown to affect the disease process: • Endothelin receptor antagonists (ERAs) are oral treatments that act by blocking the binding of endothelin, which is implicated in the pathogenesis of PAH through its actions on the pulmonary vasculature, to either one (single antagonist) or both (dual antagonist) of its receptors.23 Clinical trials have shown that treatment with ERAs has a beneficial effect on exercise capacity, WHO Functional Class (FC), haemodynamics and time to clinical worsening in patients with PAH23,28,39–42 • Prostacyclins and synthetic prostacyclins (prostacyclin analogues) act by helping to correct the deficiency of endogenous prostacyclin seen in patients with PAH. The clinical use of prostacyclins in patients with PAH has been extended by the synthesis of more stable analogues for intravenous infusion,43 as well as those that can be given by subcutaneous infusion,44,45 or by inhalation46 • Phosphodiesterase-5 (PDE-5) inhibitors are oral agents that act on the nitric oxide (NO) pathway to induce vasodilation and also have antiproliferative effects on vascular smooth muscle cells. Clinical trials have shown that treatment with PDE-5 inhibitors has a beneficial effect on exercise capacity, haemodynamic parameters, and symptoms in patients with PAH.31,47 WHOclass FCatatdiagnosis diagnosis, orscreening without 6,11 screening Figure 8. Functional – with orwith without 16,27 11 80 Patients (%) 63% 60 With screening 100 75% 80 Patients (%) 6 No screening 100 40 60 50% 40 31% 24% 20 0 12% 1% I II III WHO FC N=674 IV 44% 20 0 I Surgical intervention 13% 6% II III For patients with severe PAH who do not respond to treatment with advanced therapies, surgery may be the only option. Surgical options include balloon atrial septostomy, which creates a small hole between the right and left atria to reduce the pressure and therefore the stress on the right heart, and lung or heart and lung transplantation.2 IV WHO FC N=16 European and US guidelines now recommend annual screening of high-risk groups with Doppler echocardiography, which is currently the most effective method for screening.2,36 However, right heart catheterisation needs to be performed for a definitive diagnosis of PAH. 16 17 Pulmonary Arterial Hypertension (PAH) 12. Treatment guidelines 13. The importance of early identification and intervention in PAH Goal-oriented therapy Early diagnosis and therapeutic intervention may offer an improved outlook for patients. Prognosis and response to treatment have both been shown to be better for patients with less severe disease (i.e. WHO FC I/II) compared with those who do not begin targeted therapy until their PAH has reached a more severe stage (i.e. WHO FC III/IV).49 Disease progression may be delayed by recognising and treating patients as early as possible.40 Treatment guidelines recommend that patients with PAH receive initial monotherapy.2,33,48 The choice of initial therapy depends on a variety of factors, including disease severity, route of administration, side effect profiles, approval and reimbursement status and preferences of patients and clinicians. Once treatment is initiated, patients should be monitored regularly and their response to therapy assessed using a range of clinical, exercise, haemodynamic and echocardiographic parameters. Guidelines have identified factors associated with prognosis which should be used to monitor treatment response, including functional class, six-minute walk distance, the presence of pericardial effusion on echocardiography, and haemodynamic parameters such as right atrial pressure.2,22,48 Early diagnosis poses a challenge to healthcare professionals because many of the initial symptoms of PAH are mild and non-specific meaning many patients are not diagnosed until their disease is already quite severe.11 Regular screening can improve early detection in those patients with conditions known to be associated with PAH (e.g. systemic sclerosis or congenital heart disease). Given the diagnostic challenges, referral to expert centres is recommended to assist in the early identification of PAH.2,48 Management of patients in such centres also helps to ensure that suitable treatment is provided, patients are appropriately monitored and treatment adjusted when required, and the complex comorbidities often associated with PAH are managed optimally. Treatment guidelines recommend that, if the patient shows an inadequate clinical response to monotherapy, combination therapy using a combination of PAH-specific therapies from different classes (i.e. prostacyclin/prostacyclin analogues, endothelin receptor antagonists, phosphodiesterase-5 inhibitors) should be considered.2,33,48 The type of combination therapy chosen by the healthcare professional will depend on a variety of factors, including approval and reimbursement status and preferences of patients and clinicians. A goal-orientated strategy whereby treatment goals are set based on achieving or maintaining particular thresholds or values in parameters known to be prognostically relevant can be used to assess response.2,22 While this strategy is discussed in international guidelines,1 European guidelines currently give the most detailed advice as to the use of this strategy.2 According to European guidelines, predetermined goals based on parameters that have been shown to be associated with better prognosis should be set for the patient, and regular follow-up visits are recommended in order to ascertain progress towards the treatment goals. Based on these parameters, a patient’s condition can be categorised as:2 • Stable and satisfactory: A patient fulfilling the majority of goals or targets • Stable but not satisfactory: A patient who, although stable, has not achieved the status that the patient and treating physician would consider desirable and some of the treatment goals have not been met • Unstable and deteriorating: A patient not meeting goals or targets, and exhibiting a number of parameters associated with a worse prognosis Patients in the ‘stable but not satisfactory’ or ‘unstable and deteriorating’ categories require re-evaluation and consideration for escalation of treatment. The management of patients with PAH is complex. Given these complexities, referral of patients with PAH to an expert centre is recommended wherever possible.2,33,48 18 19 Pulmonary Arterial Hypertension (PAH) Survival according to functional class5 14. Assessing the severity of PAH Figure 10. Survival according to functional class37 100 Survival (%) Assessing patients with pulmonary arterial hypertension (PAH) involves evaluating the severity of their disease using a range of clinical assessments, exercise tests, biochemical markers, and echocardiographic and haemodynamic assessments. The clinical assessment of the patient has a pivotal role in the choice of the initial treatment, the evaluation of the response to therapy, and the possible escalation of therapy if needed. A number of parameters have been proven to have prognostic significance in PAH, although their value in a given patient may vary depending on the underlying aetiology of the disease. Some of the most important and widely-used parameters are discussed below. 80 WHO FC II 60 WHO FC III 40 WHO FC IV 20 0 Functional class 24 36 No. at risk 12 15 19 23 24 26 27 37 48 70 79 86 88 89 7 6 9 11 10 13 17 Reproduced with permission from: Wolters Kluwer Health. Humbert M, Sitbon O, Chaouat A, et al. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation 2010;122:156–63. Figure 9. WHO functional classification of pulmonary hypertension (modified from the New York Heart Association functional classification for heart failure) I 12 Time (months) The clinical severity of PAH is classified according to a system originally developed for heart failure by the New York Heart Association (NYHA) and then modified by the World Health Organization (WHO) for patients with PAH.2 This system grades PAH severity according to the functional status of the patient, linking symptoms with activity limitations, and allows clinicians to quickly and accurately predict disease progression and prognosis, as well as the need for specific treatment regimens, irrespective of the underlying aetiology of PAH (Figure 9). Functional class 0 Given this link with prognosis, improvement from WHO FC III/IV to WHO FC II and improvement or maintenance of patients with early signs at WHO FC I/II are very important goals of therapy.33 Symptomatic profile Patients with pulmonary hypertension but without resulting limitation of physical activity. Ordinary physical activity does not cause dyspnoea or fatigue, chest pain, or near syncope II Patients with pulmonary hypertension resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity causes undue dyspnoea or fatigue, chest pain, or near syncope III Patients with pulmonary hypertension resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary activity causes undue dyspnoea or fatigue, chest pain, or near syncope IV Patients with pulmonary hypertension with inability to carry out any physical activity without symptoms. These patients manifest signs of right heart failure. Dyspnoea and/or fatigue may even be present at rest. Discomfort is increased by any physical activity Functional class is a powerful predictor of outcomes in patients with PAH.2 Even with advanced medical treatment (see section: How is PAH treated?), patients in WHO FC IV continue to have extremely poor outcomes relative to those patients in lower functional classes. In a recent French study, lower functional class (I/II) was found to be positively and significantly associated with survival (Figure 10),37 while data from the US REVEAL registry showed that functional class IV was independently associated with increased mortality in patients with PAH (HR, 3.1; 95% CI, 2.2 to 4.4).50 20 21 Pulmonary Arterial Hypertension (PAH) Exercise capacity: six-minute walk test (6MWT) CPET with measuring of the VO2 max offers some advantages over the 6MWT, for example in terms of sensitivity, but these tests are more difficult to perform and require specialist equipment. As they are a maximal stress test, they are not suitable for more severe patients who may not be able to tolerate the exercise and may be exposed to risk of syncope and discomfort. The six-minute walk test (6MWT) is a key test in PAH management because it is a measure of the patient’s functional limitation and correlates with peak aerobic capacity.51 It is also a simple test to perform, which is inexpensive and convenient. In addition to distance walked, dyspnoea on exertion, and O2 saturation can also be recorded, which can provide further information regarding the patient’s condition. Haemodynamic parameters Results of the 6MWT have been shown to correlate with functional class and the distance walked significantly decreases in proportion to the severity of NYHA FC (Figure 11).52 Haemodynamic parameters are measured by right heart catheterisation (RHC) and are important diagnostic and prognostic markers in the assessment of PAH; correlating with clinical status, WHO FC, exercise capacity, and prognosis. They are also used to assess treatment effect. Prognosis is significantly correlated with markers of right ventricular function, including mean right atrial pressure (mRAP)37,50 and mean cardiac index (CI).55 Normalisation of haemodynamics may therefore be considered a suitable goal or treatment measure. Figure 11. 6MWD compared with functional class52 800 * p<0.05 vs. control subjects † p<0.05 vs. NYHA FC II 700 Serum levels of a protein known as N-terminal prohormone brain-type natriuretic peptide (NT-proBNP) have been shown to be associated with prognosis in PAH.2 A level of serum NT-proBNP below 1400 pg/mL seems to identify patients with good prognosis and who are unlikely to need escalation of treatment in the immediate future.56 However, cut-off levels still need to be verified in controlled trials, and our understanding of the role of this marker is still emerging. * 600 6MWD (m) Biochemical markers ‡ p<0.05 vs. NYHA FC III 500 *† 400 300 *†‡ 200 100 0 Control NYHA FC II NYHA FC III NYHA FC IV Reprinted with permission of the American Thoracic Society. Copyright © American Thoracic Society. Miyamoto S, Nagaya N, Satoh T, et al. Clinical correlates and prognostic significance of six-minute walk test in patients with primary pulmonary hypertension. Comparison with cardiopulmonary exercise testing. American Journal of Critical Care Medicine 2000;161(2 Pt 1):487–92. Official Journal of the American Thoracic Society It should be noted that, despite these advantages, the 6MWT is only properly validated for patients with IPAH. It is not yet clear whether it is appropriate for the assessment of treatment success in patients with, for example, PAH-SSc where accompanying conditions can make the 6MWT difficult. It also has not been standardised for all populations, and it is important that the test is performed under supervision according to a standardised protocol in order to allow meaningful comparisons.53 Cardiopulmonary exercise testing Cardiopulmonary exercise testing (CPET) assesses lung gas exchange and gives a more sensitive and comprehensive measure of exercise capacity than the 6MWT.51 It is a maximal stress test – the patient exercises at a workload that progressively increases to their symptom tolerance (i.e. the maximum workload the patient can tolerate). As such, it is difficult to perform in patients with severe disease. One important measure assessed using CPET is peak O2 consumption (VO2 max), which is a measure of the ability of the cardiovascular system to transport oxygen to the tissues and the ability of the cells to use oxygen. It has become the gold standard for assessing a patient’s exercise capacity and maximal cardiovascular response. PAH patients show reduced peak VO2 and this measurement correlates with a patient’s prognosis.54 22 23 Pulmonary Arterial Hypertension (PAH) Suggested screening protocol for the detection of PAH in SSc patients53 Figure 12. Suggested screening protocol for the detection of PAH in SSc patients61 15. PAH in patients with systemic sclerosis (SSc) SSc patients without severe pulmonary function abnormalities or severe cardiac disease Around 15% of all cases of pulmonary arterial hypertension (PAH) in a recent French PAH registry11 and 25% in a US PAH registry12 were associated with connective tissue disease, and particularly with SSc (also known as scleroderma). Doppler echocardiography Patients with SSc who develop PAH have poorer prognosis than those who do not,57,58 and PAH has become one of the leading causes of mortality in SSc patients, accounting for more than 25% of all SSc-related deaths.59 VTR <2.8 m/s NO DYSPNOEA (or dyspnoea explained by another cause) Given the significant incidence of PAH in patients with SSc and the high mortality associated with this complication if untreated, there is a clear need for early detection and timely treatment before patients show marked clinical and haemodynamic deterioration.6 VTR ≥3.0 m/s VTR 2.8–3.0 m/s DYSPNOEA (not explained by another cause) Suspected PAH NO PAH How is PAH-SSc detected? The diagnosis of PAH in patients with SSc can be particularly challenging, especially in its early stages. SSc affects a number of organs, including the lungs, and can be associated with symptoms such as fatigue and dyspnoea, which are also symptoms of PAH. As a result, detection of PAH in SSc is often delayed and patients are only diagnosed when they have advanced disease with severe clinical and haemodynamic impairment.60 Right heart catheterisation mPAP at rest <25 mmHg mPAP during exercise <30 mmHg and mPCWP <15 mmHg However, given the known high incidence of PAH in SSc, echocardiography screening is recommended in all symptomatic patients and screening by echocardiography may also be considered in all SSc patients according to the treatment guidelines.2,22 Recent studies have also shown that screening for PAH in asymptomatic SSc patients is associated with improved outcomes.60 NO PAH mPAP at rest ≥25 mmHg and mPCWP <15 mmHg mPAP during exercise ≥30 mmHg Confirmed PAH VTR, peak velocity of tricuspid regurgitation; mPAP, mean pulmonary artery pressure; mPCWP, mean pulmonary capillary wedge pressure. Figure adapted from: The three-year incidence of pulmonary arterial hypertension associated with systemic sclerosis in a multicenter nationwide longitudinal study in France. Hachulla E, de Groote P, Gressin V, et al. Copyright © 2009, John Wiley and Sons, Inc. Reproduced with permission of John Wiley and Sons, Inc. In this example of a screening algorithm,61 it is recommended that patients with SSc are regularly assessed using Doppler echocardiography (Figure 12). The parameter assessed is peak velocity of tricuspid regurgitation (VTR); patients with low VTR (<2.8 m/s) do not have PAH, whereas a high VTR (>3.0 m/s), or moderate VTR (2.8–3.0 m/s) together with dyspnoea, raises the suspicion of PAH. To confirm the diagnosis, patients must then undergo right heart catheterisation (RHC). How is PAH-SSc treated? PAH-SSc is associated with poor outcome if untreated. Data suggest that available therapies may improve quality of life and exercise capacity, and slow disease progression.62–66 Overall, patients with PAH-SSc should be treated, followed and assessed in the same way as patients with IPAH, taking into account some additional considerations.2 For example, the six-minute walk test (6MWT) used routinely to evaluate exercise capacity is not validated in patients with PAH-SSc, and complications of SSc, such as other cardiopulmonary disorders, musculoskeletal pain, fatigue, arthritis/tendonitis, and muscle weakness and contractures, can interfere with a patient’s ability to perform the test and therefore affect results.67 Treatment of patients with PAH-SSc is particularly complicated by the need to manage other problems associated with SSc, such as skin, renal, and gastrointestinal complications.68 As with other forms of PAH, patients should therefore be referred to an expert centre for PAH diagnosis and management. 24 25 Pulmonary Arterial Hypertension (PAH) 16. References 22. McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation 2009;119:2250–94. 23. Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med 2004;351:1425–36. 24. Stewart DJ, Levy RD, Cernacek P, et al. Increased plasma endothelin-1 in pulmonary hypertension: marker or mediator of disease? Ann Inter Med 1991;114:464–9. 25. Vancheeswaran R, Magoulas T, Efrat G, et al. Circulating endothelin-1 levels in systemic sclerosis subsets—a marker of fibrosis or vascular dysfunction? J Rheum 1994;21:1838–44. 26. Yoshibayashi M, Nishioka K, Nakao K, et al. Plasma endothelin concentrations in patients with pulmonary hypertension associated with congenital heart defects. Evidence for increased production of endothelin in pulmonary circulation. Circulation 1991;84:2280–5. 27. Galiè N, Grigioni F, Bacchi-Reggiani L, et al. Relation of endothelin-1 to survival in patients with primary pulmonary hypertension. Eur J Clin Inves 1996;26:A48. 28. Channick RN, Simonneau G, Sitbon O, et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet 2001;358:119–23. 29. McGoon MD, Kane GC. Pulmonary hypertension: diagnosis and management. Mayo Clin Proc 2009;84:191–207. Erratum in Mayo Clin Proc 2009;84:386. 30. Galiè N, Manes A, Branzi A. Emerging medical therapies for pulmonary arterial hypertension. Prog Cardiov Dis 2003:45:213–24. 31. Galiè N, Ghofrani HA, Torbicki A, et al. Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med 2005;353:2148–57. 32. Barst RJ, McGoon M, Torbicki A, et al. Diagnosis and differential assessment of pulmonary arterial hypertension. J Am Coll Cardiol 2004;43(Suppl S):40S–47S. 33. Barst RJ, Gibbs JS, Ghofrani HA, et al. Updated evidence-based treatment algorithm in pulmonary arterial hypertension. J Am Coll Cardiol 2009;54:S78–84. 34. Habib G, Torbicki A. The role of echocardiography in the diagnosis and management of patients with pulmonary hypertension. Eur Respir Rev 2010;19(118):1–12. 35. Benza RL, Gomberg-Maitland M, Miller DP, et al. The REVEAL risk score calculator in newly diagnosed patients with pulmonary arterial hypertension. Chest 2011 Jun 16. [Epub ahead of print] 36. McGoon M, Gutterman D, Steen V, et al. Screening, early detection, and diagnosis of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest 2004;126:14S–34S. 37. Humbert M, Sitbon O, Chaouat A, et al. Survival in patients with idiopathic, familial, and anorexigenassociated pulmonary arterial hypertension in the modern management era. Circulation 2010;122:156–63. 38. Badesch DB, Abman SH, Ahearn GS, et al. Medical therapy for pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest 2004 Jul;126(1 Suppl):35S–62S. 39. Rubin LJ, Badesch DB, Barst RJ, et al. Bosentan therapy for pulmonary arterial hypertension. N Engl J Med 2002;346:896–903. 40. Galiè N, Rubin LJ, Hoeper M, et al. Treatment of patients with mildly symptomatic pulmonary arterial hypertension with bosentan (EARLY study): a double-blind, randomised controlled trial. Lancet 2008;371:2093–100. 1. Badesch DB, Champion HC, Sanchez MA, et al. Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol 2009;54:S55–66. 2. Galiè N, Hoeper M, Humbert M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J 2009;30:2493–537. 3. Simonneau G, Robbins I, Beghetti M, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 2009;54:S43–S54. 4. Lane KB, Machado RD, Pauciulo MW, et al. Heterozygous germline mutations in BMPR2, encoding a TGF-beta receptor, cause familial primary pulmonary hypertension. The International PPH Consortium. Nat Genet 2000;26:81–4. 5. Morrell NW. Genetics of pulmonary arterial hypertension: do the molecular findings have translational value? F1000 Biol Rep 2010;2.pii:22. 6. Hachulla E, Gressin V, Guillevin L, et al. Early detection of pulmonary arterial hypertension in systemic sclerosis: a French nationwide prospective multicenter study. Arthritis Rheum 2005;52:3792–800. 7. Mukerjee D, St George D, Coleiro B, et al. Prevalence and outcome in systemic sclerosis associated pulmonary arterial hypertension: application of a registry approach. Ann Rheum Dis 2003;62:1088–93. 8. Sitbon O, Lascoux-Combe C, Delfraissy JF, et al. Prevalence of HIV-related pulmonary arterial hypertension in the current antiretroviral therapy era. Am J Respir Crit Care Med 2008;177:108–13. 9. Sitbon O. HIV-related pulmonary arterial hypertension: clinical presentation and management. AIDS 2008;22 Suppl 3:S55–62. 10. Kanmogne GD. Noninfectious pulmonary complications of HIV/AIDS. Curr Opin Pulm Med 2005;11:208–12. 11. Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med 2006;173:1023–30. 12. Badesch DB, Raskob GE, Elliott CG, et al. Pulmonary arterial hypertension: baseline characteristics from the REVEAL Registry. Chest 2010;137:376–87. 13. Diller GP, Gatzoulis MA. Pulmonary vascular disease in adults with congenital heart disease. Circulation 2007;115:1039–50. 14. Diller GP, Dimopoulos K, Okonko D, et al. Model of chronic adaptation: right ventricular function in Eisenmenger syndrome. European Heart Journal Supplements 2007;9(Suppl H):H54–H60. 15. Lapa M, Dias B, Jardim C, et al. Cardiopulmonary manifestations of hepatosplenic schistosomiasis. Circulation 2009;119:1518–23. 16. Machado RF, Gladwin MT. Pulmonary hypertension in hemolytic disorders: pulmonary vascular disease: the global perspective. Chest 2010;137:30S–38S. 17. Fonseca GH, Souza R, Salemi VM, et al. Pulmonary hypertension diagnosed by right heart catheterization in sickle cell disease. Eur Respir J 2011 Sep 8. [Epub ahead of print]. 18. Peacock AJ, Murphy NF, McMurray JJV, et al. An epidemiological study of pulmonary arterial hypertension. Eur Respir J 2007;30:104–9. 19. Gaine SP, Rubin LJ. Primary pulmonary hypertension. Lancet 1998;352:719–25. 20. Frost AE, Badesch DB, Barst RJ, et al. The changing picture of patients with pulmonary arterial hypertension in the United States: how REVEAL differs from historic and non-US Contemporary Registries. Chest 2011;139:128–137. 21. Steinhorn RH. Neonatal pulmonary hypertension. Pediatr Crit Care Med 2010;11:S79–S84. 26 27 Pulmonary Arterial Hypertension (PAH) 61. Hachulla E, de Groote P, Gressin V, et al. The three-year incidence of pulmonary arterial hypertension associated with systemic sclerosis in a multicenter nationwide longitudinal study in France. Arthritis Rheum 2009;60:1831–9. 62. Denton CP, Humbert M, Rubin L, Black CM. Bosentan treatment for pulmonary arterial hypertension related to connective tissue disease: a subgroup analysis of the pivotal clinical trials and their open-label extensions. Ann Rheum Dis 2006;65:1336–40. 63. Launay D, Sitbon O, Le Pavec J, et al. Long-term outcome of systemic sclerosis-associated pulmonary arterial hypertension treated with bosentan as first-line monotherapy followed or not by the addition of prostanoids or sildenafil. Rheumatology (Oxford) 2010;49:490–500. 64. Badesch DB, Hill NS, Burgess G, et al. Sildenafil for pulmonary arterial hypertension associated with connective tissue disease. J Rheumatol 2007;34:2417–22. 65. Badesch DB, McGoon MD, Barst RJ, et al. Long-term survival among patients with scleroderma-associated pulmonary arterial hypertension treated with intravenous epoprostenol. J Rheumatol 2009;36:2244–9. 66. Oudiz RJ, Schilz RJ, Barst RJ, et al. Treprostinil, a prostacyclin analogue, in pulmonary arterial hypertension associated with connective tissue disease. Chest 2004;126:420–7. 67. Garin MC, Highland KB, Silver RM, Strange C. Limitations to the six-minute walk test in interstitial lung disease and pulmonary hypertension in scleroderma. J Rheumatol 2009;36:330–6. 68. Kowal-Bielecka O, Landewé R, Avouac J, et al. EULAR recommendations for the treatment of systemic sclerosis: a report from the EULAR Scleroderma Trials and Research group (EUSTAR). Ann Rheum Dis 2009;68:620–8. 41. Galiè N, Beghetti M, Gatzoulis MA, et al. Bosentan therapy in patients with Eisenmenger syndrome: a multicenter, double-blind, randomized, placebo-controlled study. Circulation 2006;114:48–54. 42. Galiè N, Olschewski H, Oudiz RJ, et al. Ambrisentan for the treatment of pulmonary arterial hypertension: results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, efficacy (ARIES) study 1 and 2. Circulation 2008;117:3010–9. 43. Nicolas LB, Gutierrez MM, Galitz L, Dingemanse J. Epoprostenol with expanded stability has the same pharmacokinetic and pharmacodynamic profiles as epoprostenol in healthy subjects. Am J Respir Crit Care Med 2011;183:A5902. 44. Simonneau G, Barst RJ, Galiè N, et al. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension. A double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med 2002;165:800–4. 45. Barst RJ, Galiè N, Naeije R, et al. Long-term outcome in pulmonary arterial hypertension patients treated with subcutaneous treprostinil. Eur Respir J 2006;28:1195–203. 46. Olschewski H, Simonneau G, Galiè N, et al. Inhaled iloprost in severe pulmonary hypertension. N Engl J Med 2002;347:322–9. 47. Galiè N, Brundage BH, Ghofrani HA, et al. Pulmonary Arterial Hypertension and Response to Tadalafil (PHIRST) Study Group. Tadalafil therapy for pulmonary arterial hypertension. Circulation 2009;119:2894–903. 48. Badesch DB, Abman SH, Simonneau G, et al. Medical therapy for pulmonary arterial hypertension: updated ACCP evidence-based clinical practice guidelines. Chest 2007;131:1917–28. 49. Sitbon O, Humbert M, Nunes H, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol 2002;40:780–8. 50. Benza RL, Miller DP, Gomberg-Maitland M, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation 2010;122:164–72. 51. Ross RM, Murthy JN, Wollak ID, Jackson AS. The six minute walk test accurately estimates mean peak oxygen uptake. BMC Pulm Med 2010;10:31. 52. Miyamoto S, Nagaya N, Satoh T, et al. Clinical correlates and prognostic significance of six-minute walk test in patients with primary pulmonary hypertension. Comparison with cardiopulmonary exercise testing. Am J Respir Crit Care Med 2000;161(2 Pt 1):487–92. 53. ATS statement: guidelines for the 6-minute walk test. Am J Crit Care Med 2002;166:111–7. 54. Wensel R, Opitz CF, Anker SD, et al. Assessment of survival in patients with primary pulmonary hypertension: importance of cardiopulmonary exercise testing. Circulation 2002;106:319–24. 55. McLaughlin VV, Shillington A, Rich S. Survival in primary pulmonary hypertension: the impact of epoprostenol therapy. Circulation 2002;106:1477–82. 56. Fijalkowska A, Kurzyna M, Torbicki A, et al. Serum N-terminal brain natriuretic peptide as a prognostic parameter in patients with pulmonary hypertension. Chest 2006;129:1313–21. 57. Hachulla E, Carpentier P, Gressin V, et al. Risk factors for death and the 3-year survival of patients with systemic sclerosis: the French ItinérAIR-Sclérodermie study. Rheumatology (Oxford) 2009;48:304–8. 58. Steen V, Medsger TA Jr. Predictors of isolated pulmonary hypertension in patients with systemic sclerosis and limited cutaneous involvement. Arthritis Rheum 2003;48:516–22. 59. Steen VD, Medsger TA. Changes in causes of death in systemic sclerosis, 1972–2002. Ann Rheum Dis 2007;66:940–4. 60. Humbert M, Yaici A, de Groote P, et al. Screening for pulmonary arterial hypertension in patients with systemic sclerosis: clinical characteristics at diagnosis and long-term survival. Arthritis Rheum 2011;63:3522–30. 28 29 Pulmonary Arterial Hypertension (PAH) Notes 30 31 Pulmonary Arterial Hypertension (PAH) For further information visit www.pah-info.com © 2012 Actelion Pharmaceuticals Ltd. Gewerbestrasse 16 – CH-4123 Allschwil – Switzerland – www.actelion.com 32 Pulmonary Arterial Hypertension (PAH)