Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
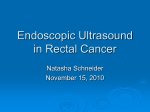
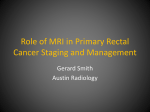
Study of endorectal ultrasonography in staging of rectal cancer Institute: Department of Ultrasound Diagnosis, Beijing Hospital of Ministry of Health, Beijing100730, China Corresponding author: GUO Fa-jin, Correspondence to: Dahua Tel: 13910813603 Fax: 01085133830 road 1, Dongdan, Beijing100730, China Email: [email protected]; Authors: REN Jun-hong, GUO Fa-jin, DAI Wei-de, HAN Xiu-jie and MA Na. Maximum # of words (4000): 3637 1 ABSTRACT Background There is no consensus regarding the performance for endorectal ultrasonography (ERUS) at every stage of rectal cancer. Thus, the purpose of our study was to further assess the value of ERUS in the preoperative staging of rectal cancer. Methods A retrospective study were performed for 44 consecutive patients (mean age: 63.3 ± 10.2 years) who underwent surgical treatment for endorectal carcinoma and preoperatively evaluated using Biplane ERUS between September 2008 and December 2010. We compared the ERUS staging with the pathology findings based on the surgical specimens. Results ERUS staging agreed with the histologic staging in 39of 44 (88.6%) patients, the agreement on the depth of transmural invasion depth was good (κappa = 0.73; 95% CI: 0.60–0.86, P=0.000). The detection sensitivities of rectal cancer with ERUS were as follows: T1 85.7%, T2 87.5%, T3 88.9%, T4 100.0% with specificity values of T1 97.3%, T2 92.9%, T3 96.2%, T4 97.6%. ERUS correctly staged patients with T1 95.5%, T2 90.9%, T3 70.5 %, T4 97.7%. The positive predictive value of ERUS was lowest for T4 (75%), but positive predictive value is highest for T3 (94.1%) as followed by T2(87.5%) and T1(85.7%); the negative predictive values of ERUS from high to low were ordered by T4(100%), T1(97.3%),T2(92.9%) and T3(92.6%) .The total overstaged cases was 4.5%, the understaged cases 6.8%. The extent of perirectal lymph node metastases was determined with sensitivity of 68.4% (13/19), specificity of 80.0% (20/25), and diagnostic accuracy of 75.0% (33/44). Conclusions Biplane ERUS has a high diagnostic accuracy for tumoral invasion of the rectal wall at every T stage, but relatively low diagnostic accuracy for lymph node metastases. Key words: Ultrasonography, endoscopic; Stage; Rectal cancer 2 In rectal cancer, the depth of tumor infiltration and metastatic involvement of lymph nodes are important prognostic factors1, 2. Accurate preoperative assessment of these prognostic factors is an important first step in assigning patients to one of the available treatment strategies. The assessment of the depth of cancer invasion (T stage) remains the primary and most important feature in the treatment of patients with rectal cancer. Endorectal ultrasonography (ERUS) as one noninvasive radiologic modalities has proved to be important and widely used diagnostic tools in the assessment of depth of cancer invasion and/or lymph node involvement. Extensive researches on the diagnostic performance of ERUS in the staging of rectal cancer have been performed 3-10 , yet a wide of variationes in study design, patient population, imaging techniques, and results exist which may be related with technical developments and different techniques employed over the years, variation in training and expertise of the investigators, patient characteristics (disease stage, age, or sex distribution).There is no consensus regarding the performance for ERUS at every stage of rectal cancer. Thus, the purpose of our study was to further assess the value of ERUS in the preoperative staging of rectal cancer at our institution. METHODS Study subjects All subjects gave their written informed consent prior to the study. This study was also approved by our Institutional Review Board. Between September 2008 and December 2010, 44 consecutive subjects with rectal cancer were admitted to our hospital. All subjects underwent biplane ERUS and colonoscopy, preoperatively. Postoperative pathological examinations were carried out in all subjects. There were 30 men and 14 women with mean age of 63.3 ±10.2 years (range from 36 years old to 79 years old). Inclusion criteria were primary invasive rectal cancer. Exclusion criteria included multiple 3 primary colon cancer, synchronous or metachronous second primary malignancie, inflammatory bowel disease, severe arrhythmia, glaucoma, intracorporeal metal parts, severe claustrophobia, as well as pregnancy. None of the patients received neoadjuvant therapy. Surgical procedures for these patients involved right hemicolectomy, transverse colectomy, left hemicolectomy, sigmoidectomy, anterior resection for rectal cancer (Dixon’s operation) or abdominal-perineal resection (Miles’ operation). Postoperative pathological examination was consistent with adenocarcinoma in 40 cases, carcinoid tumor in 1 case, stromal tumor (low grade) in 1 case, and canceration of an adenoma in 2 cases. ERUS examination A Technos DU8 ultrasound system (Esaote, Italy) with an endoluminal biplane broad band multi-frequency probe was applied. The frequencies of the linear array ranged from 5.5 to 10 MHz, and the frequencies of the convex array ranged from 5.5 to 8.5 MHz. Two-dimensional ERUS was used to observe the location, size and morphology of the lesion, the degree of tumoral invasion of the rectal wall, the relationship between the lesion and the perirectal organs, and the extent of perirectal lymphadenopathy. High-frequency color Doppler flow imaging (CDFI) was used to observe the distribution of blood flow within the lesion, the peak velocity of the arterial blood flow, and the resistance index (RI). ERUS was performed preoperatively and interpreted by one gastrointestinal radiologist and one rectal surgeon who were blinded to the findings of the digital rectal examination. The depth of transmural tumor invasion was assessed according to the TNM classifications 11,12 for both ERUS and histopathologic examinations, and results were compared prospectively. The ultrasonographic staging of rectal cancer are as follows: uT1: tumor is limited to three layers, and the submucosa is intact (Figure1A, B, C); uT2: tumor invades the muscularis propria, but does not reach the serosa (Figure2A, B, C); uT3: tumor invades the 4 rectal serosa and peripheral tissues (Fig.3 A, B, C); uT4: tumor invades adjacent organs and tissues (Fig. 4A, B, C)13; uN0: no lymph node metastasis or obvious lymph nodes are noted around the rectum, or the lymph node diameter is less than 5 mm; uN1: lymph node metastasis and the lymph node diameter is equal to or greater than 5 mm (Figure 5). Optical colonoscopy Optical colonoscopy was performed in the standard fashion with a standard endoscope (CF-Q 140; Olympus Optical Co., Tokyo, Japan) by the same gastroenterologist with at least 10 years of experience in performing endoscopy. The gastroenterologist was blinded to the results of ERUS. Sedatives and analgesics were used intravenously when necessary. The locations, sizes and numbers of colorectal neoplasms were recorded. Routine pathological examination Immediately after surgery, resected specimens were opened on the side opposite the tumor and fixed in 10% formalin. After fixation, we obtained serial slices through the whole tumor in Tis–T2 cases or through more than two sections of the deepest part of the tumor in T3 or T4 cases. The slices were embedded in paraffin, sectioned, and examined histologically after H and E staining. The resected specimens were histopathologically examined by pathologists who were blinded to the findings of the preoperative evaluation of tumor extent. Pathological T stage was identified according to the AJCC TNM (tumor-node-metastasis) Rectal Cancer Staging System14. Statistical Methods The data were represented as mean ± standard deviation ( x s ), and the count data were presented as percent proportion. The diagnostic accuracy, sensitivity, and specificity of biplane ERUS in the uT staging of rectal cancer were calculated in accordance with the postoperative pathological results (the latter were considered the gold standard). SPSS 11.0 5 was used to evaluate all data. Kappa identity test was applied and a P value less than 0.05 was considered to be statistically significant. RESULTS Detection of rectal cancer with ERUS The morphology of most tumors on ERUS was irregular with uneven hypoechoic signals inside the tumor and multiple microcalcifications observed in some areas. Tumoral invasion of various layers of the rectal wall was observed. Since malignant tumors characteristically invade along blood vessels, CDFI blood flow distribution can identify the depth of infiltration of tumor within the rectal wall. Hypervascularity was noted within each tumor and the arterial blood flow was high-impedance (RI = 0.75 ± 0.08). Enlarged perirectal lymph nodes were found in 19 cases with diameters ranging from 3.6 to 11.5 mm (mean size: 8.4 ± 0.7 mm). Staging of rectal cancer with ERUS Detailed results of the ERUS staging were listed in Table 1. Findings from histopathological examinations were served as the reference standards. Using ERUS, uT1 was found in 6 cases, uT2 in 14 cases, uT3 in 16 cases, and uT4 in 3 cases. ERUS staging agreed with the histologic staging in 39 of 44 (88.6%) patients, the agreement on the depth of transmural invasion depth was good (κappa = 0.73; 95% CI: 0.60–0.86, P=0.000). Accuracy rate, sensitivity, specificity, positive predictive value, and negative predictive value for detection of T2 to T4 stage were shown in Table 2. Among 5 cases in which staging errors were encountered at T1,1 case (14.3%) were overstaged; at T2, 1 case (6.3%)overstaged and 1 case (6.3%) understaged; at T3, 1 case (5.9%) understaged ; at T4, 1 case (25%) understaged. Histologic review of the specimens revealed that total overstaged cases( 4.5%), the tumor invaded close to the deeper uninvolved layer and reactive changes were present in 6 the connective tissue around the tumor including inflammatory. Histologic review of understaged cases (6.8%) indicated that they had only microscopic invasion beyond the estimated layers and that reactive changes of the connective tissue around the tumor were slight or absent. The extent of perirectal lymph node metastases was determined with sensitivity of 68.4% (13/19), specificity of 80.0% (20/25), and diagnostic accuracy of 75.0% (33/44). DISCUSSION For a patient with rectal cancer to achieve a better prognosis and quality of life, the extent of surgery should accurately reflect the disease status. Treatment options should be selected according to the extent of the tumor. The evaluation of the tumor infiltration depth (T staging) and the lymph node metastasis (N staging) is a very important part of preoperative staging. In general, T1 tumors invading the superficial submucosa can be effectively treated by local excision, T2 tumors invading the muscularis propria, or T3 tumors invading the perirectal fat slightly but remaining within the mesorectal fascia can be treated by mesorectal excision. Patients with T3 tumors invading the mesorectal fascia or T4 tumors invading the neighboring organs require more radical surgery15. To select patients for optimal management, it is crucial to staging of cancer before surgery, because overstaging would increase patients’ sufferings arising from the adverse effects while understaging would deprive patients from the desired benefits 16. In a meta-analysis, Bipat, et al.17obtained summary estimates and ROC curves for the diagnostic accuracy of ERUS, CT, and MR imaging in the staging of patients with rectal cancer. ERUS was found to be the most accurate modality when compared with CT and MR imaging for evaluation of local invasion of rectal cancer. For lymph node involvement, the results were comparable, with low sensitivity values. However, So far, the accuracy of ERUS 7 examination is far from satisfactory, especially for N stage. A systematic review of showed that ultrasound had an overall accuracy of 82% and was particularly useful for early localized rectal cancers. ERUS had accuracy of 73% in the assessment of nodal metastases18.And the accuracy was closely related with the experience of examiners. It is therefore possible that the overall accuracy of the examinations in routine clinical practices is even worse than was reported. In the current study, the T-stage on ERUS correlated with histopathology in 39 of 44 patients (88.6%). The N-stage on ERUS correlated with histopathology in 33 of 44 patients (75.0%). Our finding was in concordance with the previous report which determining the depth of infiltration of the tumor, the mean total accuracy of US for 2718 patients was reported to be 63%-96% with a mean value of 81.8%19, 20. Our results demonstrated that, with the reference standards of outcomes from histopathology, detection sensitivities of rectal cancer with ERUS were as follows: T1 85.7%, T2, 87.5%, T3 88.9%, T4 100.0% with specificity values of T1 97.3%,T2 92.9%, T3 96.2%, T497.6%. Patients with T1 tumors were overstaged more often compared with T2 (14.3% vs. 6.3%), and more T4 disease was understaged than T3 (25 % vs.5.9%). ERUS correctly staged patients with T1 or T2 and T4 rectal cancers more often than T3 (95.5% or 90.9% and 97.7% v s. 70.5 %). The total overstaged cases was 4.5%, the understaged cases 6.8%. Specifity of ERUS staged T1 to T4 almost equally, a great proportion of T4 was more sensitively to stage than T1 to T3.The positive predictive value of ERUS was lowest for T4 (75%), but positive predictive value was highest for T3 (94.1% ), and all most negative could be predicted at T1 to T4. The above results revealed that ERUS enabled distinction between early and advanced rectal lesion and this technique seemed to be more precise in distinguishing between T1 and T2, differentiation between T3 and T4 lesions remains challenging. Massari, et al21 found overall accuracy in staging depth of infiltration by ERUS was 90.7%. Overstaging occurred in 4% of patients, whereas understaging occurred in 5.3%. In staging lymph nodal involvement, 8 overall accuracy was 76%, sensitivity was 69.8%, specifity was 84.4%. These findings were comparable to our results. ERUS is not able to discriminate between lymph nodes inside or outside the mesorectal fascia, since the fascia is not identified at ERUS. The latter is also of importance in determining the spread of stage T3 tumors considered for total mesorectal excision. In another systematic review on the diagnostic performance of the imaging modality in the staging of rectal cancer, Kwok and colleagues22 reported summary sensitivity values of 93% with specificity values of 78% for ERUS imaging in the determination of wall penetration (stage T3). Sensitivity of this study was higher, and specificity was lower than ours, it might be related to ideal conditions in experimental study. ERUS has certain advantages in the diagnosis of rectal cancer. Biplane endorectal ultrasonography can clearly identify the rectal wall structures and perirectal lymph nodes;the ultrasound beam is vertical to the rectal wall and lesion, the biplane probe can reduce artifacts, improve image resolution, and accurately locate the tumor. Biplane endorectal ultrasonography, however, has several limitations. Tumor identification may be too deep or too shallow on ERUS. In addition, when the degree of tumor infiltration induces only a mild change in the rectal wall layers (as in superficial tumors) it can be misdiagnosed on ERUS as inflammation. Tumor and lymph nodes can also be obscured by intestinal contents on ERUS. These limitations may result in overstage or understage. Additionally, ERUS is not applicable for stenosing tumors; further improvements are necessary for optimum tailoring of treatment for the individual patient. Tumor and lymph nodes can also be obscured by intestinal contents on ERUS. We defined lymph node metastasis as lymph nodes equal to or greater than 5 mm in diameter. The size of perirectal normal lymph nodes are normally about 2-3 mm in diameter. Pathological studies show that 20% of lymph nodes less than 3-4 mm in diameter contain metastasis. The identification of lymph nodes with ERUS imaging remains a major point of 9 concern23. Ongoing research technology may be helpful in improving detection accuracy of ERUS. Recently, some newly developed techniques, such as ERUS-guided fine needle aspiration, 3D-MRI and endorectal coil MRI16 24 have been applied to improve the diagnostic accuracy of nodal metastasis in clinical practice. Although these techniques are promising in improving staging accuracy, they need further evaluation. In addition, they are not widely available.Because of the limitations in the use of both MRI and ERUS for rectal cancer staging, comprehensive evaluation should be carried out using colonoscopy, MRI, CT, and ERUS.25-29 In summary, our findings are useful for predicting histologic diagnosis and may contribute to treatment selection. The limitation of our preliminary study on ERUS in detection of rectal cancer is that only 44 symptomatic patients scheduled for ERUS were recruited. These results need to be further evaluated in a large-scale study for the population. 10 REFERENCES 1. Lindmark G, Gerdin B, Pahlman L, Bergström R, Glimelius B. Prognostic predictors in colorectal cancer. Dis Colon Rectum, 1994; 37: 1219–1227. 2. Moriya Y, Sugihara K, Akasu T, Fujita S. Patterns of recurrence after nerve-sparing surgery for rectal adenocarcinoma with special reference to loco-regional recurrence. Dis Colon Rectum 1995; 38: 1162–1168. 3. Zhou ZG, Wu XJ, Li LR, Peng ZH, Ding PR, Wang RJ, et al. A multivariate analysis of prognostic determinants for stages II and III colorectal cancer in 141 patients. Chin Med J 2011; 124: 2132-2135. 4. Du WH, Wang X, Li T, Yang WX, Xiong XQ, Wang H. Correlation between tumor VEGF expression and local blood flow features of rectal carcinoma detected by color Doppler flow imaging of transrectal ultrasound. Chin J Ultrasonography 2006; 15: 816-819. 5. Xia L, Dai X, Liu HL. The value of endoscopic ultrasonography with combination of miniature probe and radial scanning in preoperative staging for rectal cancer. Chin J of Digestive Endoscopy 2009; 26: 175-179. 6. Shi GH, Wang XM, Yu YJ, Dong XQ. Transrectal ultrasonography in preoperative staging of rectal carcinoma: diagnostic value and relationship with TNM staging. World Chin J Digestology 2009; 17: 3465-3468. 7. Beer-Gabel M, Assouline Y, Zmora O, Venturero M, Bar-Meir S, Avidan B. A new rectal ultrasonographic method for the staging of rectal cancer. Dis Colon Rectum 2009; 52: 1475-1480. 8. Stepansky A, Halevy A, Ziv Y. Preoperative staging using transrectal ultrasound in high and low rectal cancer.Isr Med Assoc J 2010; 12: 270-272. 9. Goertz RS, Fein M, Sailer M. Impact of biopsy on the accuracy of endorectal ultrasound staging of rectal tumors. Dis Colon Rectum 2008; 51: 1125-1129. 10. Halefoglu AM, Yildirim S, Avlanmis O, Sakiz D, Baykan A. Endorectal ultrasonography versus 11 phased-array magnetic resonance imaging for preoperative staging of rectal cancer. World J Gastroenterol 2008; 14: 3504-3510. 11. Sobin LH, Wittekind CH (International Union Against Cancer), eds. TNM classification of malignant tumours, 5th ed. Baltimore, MD: Wiley-Liss, 1997. 12. Hidebrand U, Feifel G. Preoperative staging of rectal cancer by intrarectal ultrasound. Dis Colon Rectaum 1985; 28: 42. 13. Massari M, De Simone M, Cioffi U, Rosso L, Chiarelli M, Gabrielli F. Value and limits of endorectal ultrasonography for preoperative staging of rectal carcinoma. Surg Laparosc Endosc 1998; 8: 438–444. 14. American Joint Committee on Cancer. Colon and rectum. In: American Joint Committee on Cancer, eds. The AJCC Cancer Staging Manual, 7th ed. New York: Springer Science+Business Media LLC; 2010: 143-159. 15. Minsky BD. Adjuvant radiation therapy for rectal cancer: is there finally an answer? Lancet 2001; 358:1285–1286. 16. Parc Y, Zutshi M, Zalinski S, Ruppert R, Fürst A, Fazio VW. Preoperative radiotherapy is associated with worse functional results after coloanal anastomosis for rectal cancer. Dis Colon Rectum 2009; 52: 2004-2014. 17. Bipat S, Glas AS, Slors FJM, Zwinderman AH, Bossuyt PMM, Stoker J. Rectal cancer: local staging and assessment of lymph node involvement with endoluminal US, CT, and MR imaging—a meta-analysis. Radiology 2004; 232:773–783. 18. Skandarajah AR, Tjandra JJ. Preoperative loco-regional imaging in rectal cancer. ANZ J Surg 2006; 76: 497-504. 19. Kumar A, Scholefield JH. Endosonography of the anal canal and rectum. World J Surg 2000; 24: 208–215. 20. Zorcolo L, Fantola G, Cabras F, Marongiu L, D’Alia G, Casula G. Preoperative staging of patients 12 with rectal tumors suitable for transanal endoscopic microsurgery (TEM): comparison of endorectal ultrasound and histopathologic findings. Surg Endosc 2009; 23: 1384-1389. 21. Massari M, De Simone M, Cioffi U, Rosso L, Chiarelli M, Gabrielli F. Value and limits of endorectal ultrasonography for preoperative staging of rectal carcinoma. Surg Laparosc Endosc, 1998, 8: 438–444. 22. Kwok H, Bissett IP, Hill GL. Preoperative staging of rectal cancer. Int J Colorectal Dis 2000; 15: 9–20. 23. Rafaelsen SR, Srensen T, Jakobsen A, Bisgaard C, Lindebjerg J.Transrectal ultrasonography and magnetic resonance imaging in the staging of rectal cancer. Effect of experience. Scand J Gastroenterol, 2008, 43: 440-446. 24. Lin XD, Lin LW, Wu LZ. The applications of transrectal ultrasound with head scanning probe in diagnosing rectal tumors. Chin J Med Ultrasound 2008; 5: 47-52. 25. Kim H, Lim JS, Choi JY, Park J, Chung YE, Kim MJ, et al. Rectal cancer: comparison of accuracy of local-regional staging with two- and three-dimensional preoperative 3-T MR imaging. Radiology 2010; 254: 485-492. 26. Zlobec I, Minoo P, Karamitopoulou E, Peros G, Patsouris ES, Lehmann F, et al. Role of tumor size in the pre-operative management of rectal cancer patients. BMC Gastroenterol 2010; 10: 61. 27. Luo MY, Liu L, Yan FH, Shen JZ, Yao LQ, Zhou KR. Preliminary study on MR colonography with air enema in detection of colorectal neoplasms Chin Med J 2010;123: 2527-2531. 28. Mathur P, Smith JJ, Ramsey C, Owen M, Thorpe A, Karim S, et al. Comparison of CT and MRI in the pre-operative staging of rectal adenocarcinoma and prediction of circumferential resection margin involvement by MRI. Colorectal Dis 2003; 5: 396–401. 29. Akasu T, Iinuma G, Fujita T, Muramatsu Y, Tateishi U, Miyakawa K, et al.Thin-section MRI with a phased-array coil for preoperative evaluation of pelvic anatomy and tumor extent in patients with rectal cancer. AJR Am J Roentgenol 2005; 184: 531–538. 13 TABLES Table 1. Comparison of T staging between US and postoperative pathological examination (cases) Ultrasonographic staging Postoperative pathological staging pT1 pT2 pT3 pT4 Total overstage understage uT1 6 1 0 0 7 14.3% uT2 1 14 1 0 16 6.3% uT3 0 1 16 0 17 5.9% uT4 0 0 1 3 4 25.0% Total 7 16 18 3 44 4.5% 6.3% 6.8% Table 2. Summary estimates for US in the staging of rectal cancer (%) pT1 pT2 pT3 pT4 Diagnostic accuracy 95.5(42/44) 90.9(40/44) 70.5(31/44) Sensitivity 85.7(6/7) 87.5(14/16) 88.9(16/18) 100.0(3/3) Specificity 97.3(36/37) 92.9(26/28) 96.2(25/26) Positive predictive value 85.7 (6/7) 87.5 (14/16) 94.1 (16/17) 75.0 (3/4) Negative predictive value 97.3(36/37) 92.9(26/28) 97.7(43/44) 97.6(40/41) 92.6(25/27) 100.0(40/40) 14 FIGURES A B C Figure 1. uT1 tumor. The tumor is limited to the former three layers, and the submucosa is intact, discontinuous mucosal echo can be observed, and the muscularis propria and serosa are intact. A: Ultrasonographic cross sectional image of the rectal wall. B: Ultrasonographic vertical section of the rectal wall. C: Pathological section (H&E staining, ×40)). A B C Figure 2. uT2 tumor. The tumor has invaded the muscularis propria, but the serosa is intact. A: Ultrasonographic cross sectional image of the rectal wall. B: Ultrasonographic vertical section of the rectal wall. C: Pathological section (H&E staining, ×40)). A B C Figure 3. uT3 tumor. The tumor has invaded the rectal serosa and peripheral tissues. A: Ultrasonographic cross sectional image of the rectal wall. B: Ultrasonographic vertical section of the rectal wall. C: Pathological section (HE staining, ×40)). 15 Figure 4. uT4 tumor. The tumor has penetrated the serosa and invaded the uterus (The arrow shows the uterus). Figure 5. Pathological image of lymph node metastasis around the rectal cancer (H&E staining, ×40). 16