Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
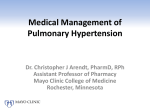
REVIEW ARTICLE Pulmonary arterial hypertension, a rare entity Jaime Eduardo Morales-Blanhir,* Andrés Eduardo Carmona-Rubio,† María de Jesús Rosas-Romero,* Gloria Silene Vergara de Márquez,‡ Guillermo Adolfo Arbo Oze de Morvil§ *Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. FEMEXER. †Universidad de Buffalo, Universidad Estatal de Nueva York. ‡ Sociedad Venezolana de Cardiología. Unidad de Hipertensión Pulmonar del Hospital Clínico. Maracaibo. Venezuela. §Sociedad Paraguaya de Neumología. Asunción, Paraguay. ABSTRACT Hipertensión arterial pulmonar, una entidad rara RESUMEN Pulmonary arterial hypertension (PAH) is a rare disease. It is characterized by the progressive remodeling of the small pulmonary arteries that lead to an elevation of the pulmonary vascular resistance and right ventricular dysfunction. Early diagnosis and prompt treatment avoid the deterioration of the patient’s quality of life. Statistics show that there are 15 cases per million people worldwide, the majority composed of young women, with an age at diagnosis of 30 to 40 years. At present, the exact processes that initiate the pathophysiologic changes observed in PAH are unknown; it is thought to be multifactorial. Diagnosis in PAH must be done in a step by step manner. Under the suspicion of pulmonary hypertension (PH), the first thing to do is confirm the diagnosis. The second step is to identify the specific etiology and lastly evaluate the severity by echocardiography, hemodynamic parameters, biomarkers and exercise capacity. PH treatment, particularly PAH, has evolved over the last 2 decades due to the advance in disease knowledge and the availability of agents that act on different pathways. Concerning surgical treatment, it is indicated in PAH when there is not an adequate response to medical treatment. In conclusion, PAH is recognized worldwide as a rare or infrequent disease. The countries that have a registry for the diagnostics, treatment, follow-up and prevalence of PH are mainly in Europe. With the exception of the United States and Canada, there are no registries in America. Recent years have shown an important advance in Latin America. La hipertensión arterial pulmonar (HAP) es una enfermedad rara que se caracteriza por un aumento progresivo de la resistencia vascular pulmonar, que conlleva a la insuficiencia cardiaca derecha y la muerte prematura. Su diagnóstico y tratamiento temprano es esencial para tener un impacto en el pronóstico a largo plazo. Las estadísticas reportan 25 casos/ millón de habitantes, principalmente en mujeres, con una edad de diagnóstico entre 30/40 años. Se conoce que algunos de los procesos que desencadenan los cambios fisiopatológicos son multifactoriales. Ante la sospecha, primero confirmar el diagnóstico, identificar la clase de hipertensión pulmonar (HP) de acuerdo con la clasificación y, por último, realizar estudios adicionales para identificar el tipo de HAP. El tratamiento de la HP, en especial de la HAP, ha permitido la aprobación de varias terapias específicas que confieren mejoras en la clínica, hemodinámica, calidad de vida y sobrevida. El tratamiento quirúrgico está indicado posterior a no obtener una respuesta adecuada en el tratamiento médico. En conclusión, la HAP se conoce como una enfermedad rara o huérfana, los países que llevan un registro en el diagnóstico, tratamiento, seguimiento y prevalencia son en su mayoría europeos; en América, exceptuando Estados Unidos y Canadá, no se cuenta con registros; sin embargo, en los últimos años existen avances importantes en Latinoamérica. Key words. Pulmonary hypertension. Pulmonary arterial hypertension. Echocardiography. Palabras clave. Hipertensión pulmonar. Hipertensión arterial pulmonar. Ecocardiografía. INTRODUCTION vation in the pulmonary vascular resistance (PVR), which leads to right ventricular failure and premature death.1 National Institute of Health (NIH) PAH patient registry in the United States reported a Pulmonary arterial hypertension (PAH) is a rare disease that has been described as a progressive ele- Rev Invest Clin2014 Morales-Blanhir JE, et al. Clínica Pulmonary arterial hypertension. 2014;/ 66 65-78 Revista de Investigación / Vol. 66, Num. 1 / January-February, pp (1): 65-78 Full text of this article available in internet: www.imbiomed.com.mx 65 mean age of 35.9 ± 12.2 years, female-male ratio of 2.4:1.2 The prevalence is 25 cases per million people in Switzerland/France,3,4 and in Scotland 26 cases per million people.5 Information available concerning PAH in Latin America is limited. PAH is defined as the rise in the mean pulmonary arterial pressure (mPAP) > 25 mmHg at rest, determined by right heart catheterization (RHC).6,7 The definition of PAH during exercise (mPAP > 30 mmHg) is no longer used due to lack of scientific evidence.7-8 Valerio, et al., observed patients with scleroderma and mPAP 21-24 mmHg, where initially they found an elevated transpulmonary gradient that ended in developing pulmonary hypertension during follow up.9 Physiopathology concerning pulmonary arterial hypertension (PAH) is currently unknown and it is thought to be multifactorial. The most important function of the pulmonary endothelium is PVR maintenance. The rise of PVR is related to different mechanisms which include vasoconstriction, pulmonary vascular wall remodeling (proliferative and obstructive), inflammation and thrombosis. Excessive vasoconstriction has been related to anomalous expression of potassium channels in smooth muscle cells and endothelial dysfunction. The latter generates a chronic deficiency of vasodilators and proliferative agents [nitric oxide (NO) and prostacyclins], along with the overexpression of vasoconstrictive and vasodilator substances (thromboxane A2 and endothelin-1).6,7 Several genetic alterations have been identified through biomolecular techniques and developing experimental models. The term hereditary PAH (HPAH) includes familial PAH (PAH present in one or two members of the family) and simple PAH (only one subject in a family) when a spontaneous mutation is identified. In 75% of reported HPAH cases a 1 2 3 66 Set treatment goals , Establish patient s mutation in the gene that codes the bone morphogenetic protein type 2 (BMPR2) was detected. Other mutations were also found (ACVRL1, BMPR1B, CAV1, ENG, SMAD9) but are less common (< 1%). HPAP presents itself with the same signs, symptoms and histologic changes as idiopathic PAH. The time from the initiation of symptoms to diagnosis can be shorter in individuals with familial PAH due to the presence of higher suspicion. Three retrospective clinical trials suggest that patients with a mutation in the BMPR2 present it self with severe disease. 10 Prenatal testing in high risk pregnancies is an excellent alternative in a family with a confirmed diagnosis of familial PAH.11 Any condition considered to predispose or facilitate PAH is considered a risk factor. Initial clinical values are important for risk assessment. However, their utility for prognosis is limited because they can change with time and intervention. The evaluation of the goals of therapy in PAH, using the criteria established in the guidelines of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS) are reflected in figure 1. Future investigations must be focused in developing a dynamic scoring system to evaluate time dependent variables over clinical results.12 Different classifications of pulmonary hypertension (PH) allow investigators to organize the data collected from patient registries and clinical trials. During the 2008 International Symposium in Dana Point it was decided to maintain the current structure with a five group classification.13,14 The same classification was kept in Nice 2013, were the main discussions involved topics in: genetics, congenital or acquired left heart diseases (e.g. outflow and inflow tract obstructions), developmental lung diseases and other uncertain multifactorial entities. Rate of progression WHO-FC Syncope 6MWD Echo findings CPET BNP/NT proBNP Haemodynamics Clinical evidence of right heart failure clinical status Stable and satisfactory Review treatment regimen No change Stable and not satisfactory Unstable and deteriorating Escalation Figure 1. Risk assessment and treat-to-target approach for pulmonary arterial hypertension. WHO-FC: World Health Organization-functional class. 6MWD: 6-min walking distance. CPET: cardiopulmonary exercise testing. Echo: echocardiography. BNP: brain natriuretic peptide. NTproBNP: N-terminal-pro-brain natriuretic peptide. Adapted from Rubin, et al. 201212, with permission from the publisher. Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 Analysis of the data involving survival from the latest cohorts of PAH is biased by patients included months or years after their diagnosis (survivors) who have a better prognosis than patients newly diagnosed during the evaluation. Critical analyses of the cohorts show an improved survival. However, idiopathic PAH is still a severe disease with poor prognosis.15 DIAGNOSTICS Upon suspecting PH the first thing is confirming the diagnosis. The second is identifying the class of PH. Lastly, performing tests to find out the type of PAH, figure 2. Idiopathic PAH is considered a diagnosis of exclusion. Symptoms/Signs/History suggestive of PH Noninvassive assessment compatible with PH? Search for other causes and/or re-check No Yes Consider common causes of PH Group 2: left heart disease? Group 3: lung diseases and/or hypoxia? History, symptoms, signs ECG, chest radiograph TTE, PFT, HRCT Group 2 or 3: diagnosis confirmed Yes PH “proportionate” to severity NO Yes “out of proportion” PH Treat underlying disease and check for progression Perform V’/Q’ scan Segmental perfusion defects Consider group 4: CTEPH Yes NO Search for other causes Consider other uncommon causes NO Perform RHC (PAH probability*) Ppa ≥ 25 mmHg Ppcw ≤ 15 mmHg Consider PVOD/PCH Specific diagnostic tests PVOD PCH Clinical signs HRCT, ANA CTD History Drugs, toxins HIV test TTE, TEE, CMR Yes Physical, US, LFT Physical, laboratory analysis Portopulmonary HIV CHD Idiopathic or heritable PAH Schistosomiasis, other group 5 Chronic haemolysis BMPR2, ALK-1, endoglin (HHT), family history Figure 2. Diagnostic algorithm. ALK-1: activin-receptor-like kinase. ANA: anti-nuclear antibodies. BMPR2: bone morphogenetic protein receptor 2. CHD: congenital heart disease. CMR: cardiac magnetic resonance. CTD: connective tissue disease. CTEPH: chronic thromboembolic pulmonary hypertension. Group: clinical group. HHT: hereditary haemorrhagic telangiectasia. HRCT: high-resolution computed tomography. LFT: liver function tests. Ppa: mean pulmonary arterial pressure. PAH: pulmonary arterial hypertension. PCH: pulmonary capillary haemangiomatosis. Ppcw: pulmonary capillary wedge pressure. PFT: pulmonary function test. PH: pulmonary hypertension. PVOD: pulmonary veno-occlusive disease. RHC: right heart catheterization. TEE: transoesophageal echocardiography. TTE: transthoracic echocardiography. US:ultrasonography. V’/Q’: ventilation/perfusion lung scan. Adapted from Galiè, et al. 20097 with permission from the publisher. Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 67 An important consideration in Latin America is the fact that some countries do not have PH qualified physicians and in some places, especially rural areas, it is hard to find hospitals with the necessary equipment to perform diagnostic tests.16 Clinical suspicion of PH is based on the symptoms, signs and the presence of risk factors.7,17-18 Detection requires studies to confirm the diagnosis: electrocardiogram, chest radiography and Doppler echocardiogram. The latter is a very useful tool in the diagnosis19-23 and screening of patients with risks of developing PAH, e.g. congenital cardiomyopathies, venous thrombosis, connective tissue disorders, human immunodeficiency virus (HIV) or the exposure to toxics associated with PAH.6-7 The identification of the type of PH requires several diagnostic tests. Pulmonary function tests (PFTs) and high resolution computerized tomography (HRCT) of the chest, to rule out left sided cardiomyopathies (group 2) or lung diseases (group 3).24-26 If there is no evidence of the mentioned pathologies or PH disproportionate to the underlying condition, pulmonary ventilation/perfusion scan (V/Q) which is more sensitive than chest HRCT for chronic thromboembolic pulmonary hypertension (CTEPH) is the next step [sensitivity (S): 90100%, specificity (E): 94-100%].27,28 If the V/Q shows multiple perfusion defects CTEPH has to be suspected, for definitive diagnosis RHC has to be performed and in some cases selective pulmonary angiography.29 Lastly, blood work is done, e.g. HIV, thyroid testing30 and immunologic workup.31 Other tests that can be performed are, abdominal ultrasound,32-34 evaluation of exercise capacity (6 min walk and cardiopulmonary exercise test), RHC with pulmonary vascular reactivity test (PVRT)7 to identify PAH.35-38 Recently, cardiovascular magnetic resonance has been used to measure and calculate hemodynamic parameters and evaluate the right ventricle (RV).39-41 In relation to the early detection of PAH there have been important advances. Although, there is still room for improvement in diagnostics, catheterization and patient management. Definitive diagnosis can be delayed for up to 2 years from the start of symptoms, which is still a challenge. Targeting high risk patients can allow early diagnosis in PAH. However, methods utilized routinely in clinical practice have limitations. A combination of tools and parameters is required to improve the sensitivity and specificity. PAH is a disease that progresses fast, even in patients with mild symptoms and appropriate therapy. This is why early detection can have a big impact in long term prognosis in PAH patients.42 68 PROGNOSTIC FACTORS Demographic factors, such as sex or time of initiation of symptoms, are not clearly related to mortality. On the other hand, age (< 14 years or > 65 years of age) and race (Afro-American and Asian) have been showed to have a worse prognosis.43 Survival between male and females is similar in studies which were done before and after initiating appropriate therapy.44 Associated PAH pathologies can influence the prognosis, e.g. multiple sclerosis alone or accompanied by interstitial lung disease, HIV45 and portal hypertension 32-34 have been shown to have a poor prognosis. Pregnancy has also been described as having a poor prognosis in patients with PAH. Functional class Clinical assessment provides valuable prognostic information that can guide patient management. Syncope, hemoptysis and signs of right ventricular failure lead to a bad prognosis, as well as, rapid progression of the latter. Although there is great variation between observers measuring World Health Organization Functional Class (WHO-FC), it still remains an important indicator of survival. Patients with WHO-FC I and II have a better prognosis than WHO-FC III or IV. In the NIH Registry, mean survival of patients with mild to moderate symptoms (WHO-FC I and II) was 58.6 months compared to 31.5 months in patients who had moderate to severe symptoms (WHO–CF III) and was 6 months in patients with severe symptoms (WHO-FC IV).46 Exercise capacity An important parameter utilized in PAH is the measurement of exercise capacity. For objective assessment we use the 6 min walk (6MW)47 and the cardiopulmonary exercise test (CPET). 6MW is simple, economic, reproducible and standardized. On top of the distance walked, the amount of dyspnea during exercise is measured using the Borg Scale and oxygen saturation is measured through digital pulse oximetry. The 6MW is done at the time of diagnosis and it helps assess response to treatment. Walking a distance of < 332 meters or < 250 meters and having an oxygen desaturation > 10% are indicators of bad prognosis in PAH.7 In a recent study, the evaluation of the pulmonary function during CPET demonstrated that patients with PAH have a ventilator equivalent for CO 2 (VECO2) < 48, peak Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 oxygen consumption (peak VO2) > 13.2 mL/kg/min, delta O2 > 3.3 mL/min, 6MW of 399 m and an increased accumulative survival compared to patients that lack the above (p < 0.05).48 Hypocapnia during rest and exercise is correlated with a low cardiac output, low VECO2 and as an independent maker of mortality.49 Biological markers Biological markers constitute a noninvasive tool for observation and evaluation of RV dysfunction in PAH patients. Serum quantification of brain natriuretic peptide (BNP) is of use in PAH patient prognosis,50 levels of BNP is associated with pulmonary arterial pressure (PAP) and PVR.51 PAP and PVR values correlate with the rise of BNP and have an inverse relationship with the cardiac index. Other biological markers that suggest bad prognosis: hyperbilirubinemia, hyponatremia, hyperuricemia, Von Willebrand factor elevation and high sensitivity cardiac troponin-t elevation. Takeda, et al., in a study with 37 PAH patients demonstrated that the rise in bilirubin levels is a risk factor for mortality.52 Hypeuricemia is common in patients with PAH. Recently, a study proposed investigating the possible clinical benefit of lowering high levels of uric acid.53 The elevation of high sensitivity troponin-t is associated with advanced WHO-FC and high mortality; additionally it is related to RV dysfunction and deterioration in the 6MW.54 Hemodynamic and echocardiographic parameters Multiple prognostic parameters are generated through echocardiography: RV area, left ventricle (LV) eccentricity index or Ryan index, Tei index, tricuspid annular plane systolic excursion (TAPSE) and the presence of pericardial effusions.7 Patients without pericardial effusions have been proven to have a better prognosis. Hemodynamic parameters measured at rest by RHC have prognostic values. In the NIH registry, three hemodynamic variables are associated with the rise in the risk of mortality: increase in mPAP [relative risk (RR): 1:16; 95% confidence interval (CI): 1.05 -1.28]; increase right atrial pressure (RAP) [RR:1.99; 95% CI: 1.47-2.69] and decrease cardiac index [RR: 0.62; 95% CI: 0.46-0.82].6 Patients with RAP < 8 mmHg or cardiac index ≥ 2.5 L/ min/m2 have better prognosis than those with RAP > 8 mmHg or cardiac index ≤ 2.5 L/min/m2.55 TREATMENT During the last two decades advanced comprehension of the pathogenesis of PAH led to the approval of different specific therapies bestowing improvement in clinical symptoms, hemodynamics, quality of life and survival of patients. The therapeutic algorithm is targeted at PAH (group 1) patients, it is not appropriate for group 2 and 3. At the moment there is no evidence supporting treatment for uncertain multifactorial mechanisms. Main focus after diagnosis of PAH is to adopt general measures, initiate supportive medical treatment and send a patient to PH referral centres.7,56 Class of recommendations (CR): I and level of evidence (LE): C. In Latin America there are referral centers in most countries, mainly in the more populated cities.16 General measures include daily living activity recommendations: • • • • Physical rehabilitation CR: I-LE: A. Birth control CR:I-LE: C. Psychosocial support CR:I-LE: C. Influenza and pneumococcal immunizations CR:ILE:C. Supportive medical treatment consists of: • Oral anticoagulation CR:IIa-LE:C for Idiopathic PAH and CR:IIb-LE: C for Associated PAH. • Diuretics CR:I-LE:C. • Oxygen CR:I-LE:C. • Digoxin and other inotropic drugs CR:IIb-LE:C. These treatments are commonly used; although there are no randomized, controlled clinical trials in PAH who support their use. 56 Specific medical treatment is established in referral centers using pharmacotherapy that acts through endothelin, nitric oxide and prostacyclin pathways that participate in PAH development. In concordance with the results obtained by RHC, if the PVRT has a positive response, defined as a decrease in mPAP or < 40 mmHg, maintaining the same or increased cardiac output, therapy is initiated with calcium channel blockers (CCB), CR:I-LE:C. If there is no positive response, other treatment options need to be explored. According to the WHO-FC: • WHO-FC II. Ambrisentan, bosentan, macitentan, riociguat, sildenafil, tadalafil, CR:I-LE:A o B. Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 69 • WHO-FC III. Ambrisentan, bosentan, intravenous epoprostenol (IV), inhaled iloprost, macitentan, riociguat, sildenafil, tadalafil, subcutaneous (SC) or inhaled treprostinil, CR:I-LE: A o B. IV Iloprost, IV treprostrinil CR:IIa-LE:C. Beraprost, CR:IIb-LE:B. Initial combination therapy CR:IIb-LE:C. • WHO-FC IV: IV epoprostenol CR:I-LE:A o B. Ambrisentan, bosentan, inhaled o intravenous iloprost. Macitentan, riociguat, sildenafil, tadalafil, inhaled, subcutaneous or intravenous treprostinil CR:IIa-LE:C. Initial combination therapy CR:IIb-LE:C. Because there is no well-defined comparison between medications, first line evidence based treatment can not be proposed. Choice of medication is dependent on multiple factors which include: approval status, form of administration, side effect profile and treatment physician experience/preference.56 In Latin America, knowledge is limited to the medications used as monotherapy and combination therapy illustrated in table 1 and table 2. Calcium channel blockers Only 10-15% of PAH patients have a positive PVRT by RHC, making those candidates eligible to receive long term CCB, especially nifedipine or diltiazem. The use of verapamil is not recommended due to its negative inotropic effect. In a prospective study with high dose CCB; nifedipine 90-240 mg/day or diltiazem 360-900 mg/day, significantly improved prognosis of patients with positive PERT.57 Another essay showed the utility of 20-40 mg daily doses of amlodipine. It is important to do hemodynamic and clinical evaluations on patients 3-6 months after initiating therapy.58 Prostanoids The utility of prostacyclin’s in patients with PAH has increased with the synthesis of stable analogs that possess different pharmacokinetic properties with similar effects.6,7 Epoprostenol has a short half-life ~3 min; it is administered via continuous intravenous infusion Table 1. Drugs for pulmonary hypertension in Latin America. Pharmacological Argentina Brazil Chile Colombia Costa Rica Cuba México Paraguay Perú Venezuela • Calcium channel blockers Nifedipine Diltiazem Amlodipine Verapamil • Prostanoids Epoprostenol Treprostinil Iloprost Beraprost • Endothelin receptor antagonists Bosentan Ambrisentan • 5-phosphodiesterase inhibitors Sildenafil Tadalafil Vardenafil • Non-pharmacological Balloon atrial septostomy Lung Transplant : available/approved. 70 : available/not approved. Adapted from Morales-Blanhir, et al. 2011.16 Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 Table 2. Combined therapy used in Latin America. Argentina Brazil Chile Colombia Costa Rica Cuba Mexico Paraguay Perú Venezuela Bosentan+ Sildenafil Sildenafil+ Iloprost Iloprost+ Bosentan Sildenafil+ Treprostinil Treprostinil+ Bosentan Treprostinil+ Iloprost : used. Adapted from Morales-Blanhir, et al. 2011. 16 through a tunneled catheter. This drug improves symptomatology, exercise capacity and hemodynamics in PAH, it is the only treatment proven to increase survival in idiopathic PAH, associated PAH and non-surgical CTEPH in randomized clinical trials.7,59,60 Treprostinil is a tricyclic benzidine analogue of epoprostenol; it can be administered intravenously, subcutaneously, orally and inhaled. Lang, et al., performed an long term, open clinical trial where they observed an improvement in exercise capacity and symptoms employing SC trepostinil in idiopathic PAH or CTEPH, with a 26 month follow up.7,61 The use of inhaled trepostinil was evaluated in the TRIUMPH trial (Treprostinil Sodium Inhalation Used in the Management of Pulmonary Arterial Hypertension) where benefit in PAH patients was observed at 24 months of its administration.62 Another controlled, randomized trial FREEDOM-C (Oral Treprostinil for the Treatment of Pulmonary Arterial Hypertension in Patients on Background Endothelin Receptor Antagonist and/or Phosphodiesterase Type 5 Inhibitor Therapy) amplified the understanding of oral dosing and titration of trepostinil.63 Iloprost is a chemically stable prostacyclin analog that can be administered intravenously or by aerosol. The most used is the inhaled version. In a trial, 63 PAH patients treated with iloprost reported an 85% two year survival, proving that it is a well-tolerated long term therapy.64 Beraprost is a stable oral prostacyclin analog. In a randomized and controlled trial labeled ALPHABET (Arterial Pulmonary Hypertension and Beraprost European Trial) in Europe65 and a second in the United States66 with beraprost at a 80 μg dose, four times a day, showed an improvement in exercise capacity that persisted only for 3-6 months, without any evidence of hemodynamic benefits. In a multicentric trial that lasted 12 weeks with 46 patients with PAH showed that a long acting preparation of beraprost (TRK100STP) improved exercise capacity, mPAP and PVR. It also showed that this product was effective in Japanese patients with PAH.67 Selexipag is an oral, selective prostacyclin receptor agonist. It was evaluated in a double blind, controlled, randomized, phase II trial with 43 PAH patients. Approximately one third of the patients were being treated with endothelin inhibitors or sildenafil as base treatment. The dose of selexipag was 200 mg twice a day, with increase to maximum tolerated doses. Decrease in PVR was observed, when compared with placebo in the seventeenth week (-30, 3%; p = 0.0045). Additionally, improvement in the 6MW was observed, although this did not reach statistical significance. When compared with placebo, selexipag therapy is associated with an increase in CI. This medication is well-tolerated with a good safety profile at the expected pharmacological effect.68-70 Endothelin receptor antagonists Activation of the endothelin (ET) system has been demonstrated in both plasma and lung tissue of PAH patients. Bosentan is an oral active dual endothelin-A and endothelin-B receptor antagonist (ERA). It has been evaluated in PAH (idiopathic, associated with connective tissue disease and Eisenmenger’s syndrome) in randomized clinical trials BREATHE-1,2,5: (Bosentan Randomized Trial of Endothelin Antagonist Therapy-1,2,5) and EARLY (Endothelin Antagonist trial in Mildly Symptomatic PAH patients) that showed improvement in exercise capacity, functional class, hemodynamics, echocardiographic variables and time to clinical worsening.7,56 In a registry with 528 patients, distributed in 15 referral Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 71 centers in Australia, from 2004-2007, it was demonstrated that treatment with bosentan improved prognosis in idiopathic PAH and connective tissue disease-associated PAH.71. In multiple trials, there was a 10% rise in hepatic aminotransferases enzymes; this is why liver function tests must be done at least once a month.56 Ambrisentan is a non-sulfonamide, propanoic acid-class, ERA that is selective for the endothelin-A receptor. Its usage was evaluated in two randomized, controlled clinical trials ARIES 1-2: (Ambrisentan in Pulmonary Arterial Hypertension 1 and 2), which demonstrated efficacy in symptomatology, exercise capacity, hemodynamics and time to clinical worsening.72 In these patients liver function tests have to be done once a month. Macitentan is a new dual ERA in clinical development for PAH. A phase 1 clinical trial, compared pharmacokinetics and safety of macitentan in healthy Caucasian and Japanese subjects; it also compared difference between genders. The study showed no significant clinical difference with adverse effects, laboratory values, EKG and vital signs between the two groups. Additionally, they proved that it was not necessary to adjust the dose of macitentan based on gender or ethnicity.73 Pulmonary fibrosis is a progressive and fatal disease. A double-blind, randomized, placebo-controlled, multicenter, parallel group study to evaluate the efficacy, safety, and tolerability of macitentan in patients with idiopathic pulmonary fibrosis (NCT00903331) did not demonstrate that macitentan positively affects the forced vital capacity (FVC) in comparison with placebo in patients with idiopathic pulmonary fibrosis.74 In another multicenter, double blinded, randomized controlled-placebo trial called SERAPHIN (Study with an Endothelin Receptor Antagonist in Pulmonary Arterial Hypertension to Improve Clinical Outcome) showed that macitentan significantly reduced mortality in PAH. 75 Phosphodiesterase-5 inhibitors The benefit of phosphodiesterase-5 inhibitors (PDE-5) in vascular remodeling and pulmonary vasodilation is well known. Sildenafil is an orally active PDE-5 selective inhibitor. Several non-controlled trials have described favorable effects of sildenafil in idiopathic PAH, connective tissue or congenital heart disease associated PAH and CTEPH. A randomized, controlled trial SUPER-1 (The Sildenafil Use in Pulmonary Hyper- 72 tension-1), showed that 278 patients with PAH treated with sildenafil 20, 40 and 80 mg, three times a day (TID), had a favorable effect in: exercise capacity (increasing 50m in the 6MW), symptoms, hemodynamics and quality of life.76 The dose approved is 20 mg TID. Once the SUPER-1 TRIAL concluded, 259 of the 277 patients were enrolled in the SUPER2, an open, non-controlled extension. These 2 trials proved that long treatment (> 3 years) with sildenafil as a monotherapy improved WHO-FC and 6MW in patients with PAH.77 In patients with chronic to obstructive pulmonary disease (COPD) associated PH, sildenafil improved hemodynamic parameters at rest and during exercise. This effect is accompanied by the inhibition of the hypoxic vasoconstriction and deterioration of arterial oxygenation at rest; this is why in COPD associated PAH arterial blood gas monitoring is necessary.78 Tadalafil is a selective inhibitor of PDE-5, administered once a day. It was studied, in a controlled, randomized trial, called PHIRST (Tadalafil in the Treatment of Pulmonary Arterial Hypertension), which included 405 patients with PAH treated with tadalafil doses of 5, 10, 20 or 40 mg, once a day. They observed positive results in: exercise capacity, symptoms, hemodynamics and time to clinical deterioration with the highest dose. This trial concluded that monotherapy with tadalafil 40 mg, favors clinical improvement in these patients.79 Vardenafil is a selective inhibitor of PDE-5. Jing, et al., in an open, multicentric trial with 45 patients with PAH, treated with vardenafil 5 mg, once a day, during 4 weeks and then 5 mg twice a day, showed that therapy was well tolerated, it improved 6MW, WHO-FC and hemodynamic parameters.80 Riociguat is a soluble guanylate cyclase activator that produces vasodilation and stimulates endogenous nitric oxide mediated vasodilation. Two clinical trials have studied riociguat, PATENT-1 (Pulmonary Arterial Hypertension Soluble Guanilate Cyclase-Stimulater trial 1)81 and CHEST-1 (Chronic Thromboembolic Pulmonary Hypertension Guanilate Cyclase-Stimulater trial 1).82 In the first trial, 443 patients with PAH were treated with riociguat during 12 weeks, it showed improvement in the 6MW distance covered and PVR. The second trial, with 261 patients with CTEPH observed improvement in the same parameters though 16 weeks. Riociguat would be the first non-surgical therapy approved for CTEPH and an additional option in PAH, where it seems to be safe and well tolerated. Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 Hoeper, et al., administered riociguat, in a nonrandomized, open trial with 13 cases of idiopathic pulmonary fibrosis (IPF) associated PAH, 5 cases of unspecific interstitial pneumonia, 3 cases of sarcoidosis and 1 case of scleroderma, observing hemodynamic improvement at 12 weeks and an increase in the 6MW, but no change in WHO-FC or clinical improvement. Adverse effects were lower extremity edema, dyspepsia and headaches.83 In another double blinded, randomized trial, the effect of riociguat was evaluated in 201 patients with PH due to LV systolic dysfunction; although the primary endpoint of the study was not met, riociguat was well tolerated and improved the cardiac index, and systemic and PVR.84,85 COMBINATION THERAPY This is an attractive and logic alternative in PAH patients. It is directed to those patients who have a poor response to initial monotherapy CR:I-LE:A and WHO-FC III and IV CR:IIb-LE:C. The severity of disease and increase in the number of available medications, invite the exploration of combining different mechanisms of action with the purpose of optimizing clinical benefit and decreasing adverse effects. The two proposals are: • Start with combination therapy, or • Add a new medication to the patients existing treatment regimen (sequential combination).86 Multiple studies suggest that combination therapy is effective.87-92 Humbert, et al., evaluated the administration of bosentan and epoprostenol in 33 patients with PAH WHO-FC III and IV and observed hemodynamic improvement but had no statistical significance. 87 McLaughlin, et al., showed in a study with 67 patients with PAH the benefits of adding inhaled iloprost in patients who were using bosentan, observing an improvement in WHO-FC and 6MW. 88 The addition of bosentan to patients who were using sildenafil (or vice versa) has also been studied. 89,90 The addition of sildenafil to epoprostenol was described in a 267 PAH patient study that observed improvement in: exercise capacity, hemodynamics and quality of life; but not in the dyspnea Borg scale. 91 Another drug added to bosentan and sildenafil is inhaled trepostinil. In a study with 235 PAH patients, WHO-FC III and IV showed an improvement in quality of life and exercise capacity with trepostinil and bosentan or sildenafil combination. 92 Lastly, the addition of tadalafil in patients who were receiving bosentan did not show conclusive results or benefits.79,93 FUTURE MEDICAL THERAPIES New therapeutic agents are aimed at reversing sustained or abnormal vasoconstriction and/or at stopping or reversing abnormal cell growth and abnormal extracellular matrix protein deposition. Some of these promising therapies include: vasodilator peptides (vasoactive intestinal peptide), gene therapy, tyrosine kinase inhibitors and growth factor inhibitors (imatinib, gefitinib, erlotinib y patinib).94-96 Vasoactive intestinal peptide (VIP) is a potent pulmonary and systemic vasodilator. It is administered via inhalation in PAH. Rhodes, et al., in a case series of 8 idiopathic PAH patients, treated with inhaled VIP at a dose of 200 μg for 3 months, observed significant changes in mPAP < 13 mmHg, cardiac index > 1.7 L/min, PVR < ~50% and 6MW > 113 m. VIP should be considered as a future alternative in PAH pharmacotherapy.94 Hereditary PAH is associated to BMPR2 mutation. This has raised the idea of utilizing gene therapy to replace the missing gene and possibly serve as a permanent cure of the disease. No clinical trials have shown positive results on this therapeutic modalito.97 Tyrosine kinase inhibitors, specifically platelet derived growth factors (PDGF) have shown to be potent vasodilators, decreasing excessive vasoconstriction and smooth muscle proliferation. Several case reports suggest that terminal phase PAH patients can benefit from PDGF inhibitors, e.g. imatinib.96 Other pathways currently being investigated: Rho kinase (ROCK) inhibitors (fasudil), endothelial nitric oxide synthase coupling agents (cicletanine), multikinase inhibitors (sorafenib), elastase inhibitors, metabolic modulators (dichloroacetate), survivin inhibitors, peroxisome proliferatoractivated receptor gamma Inhibitors. (PPAR γ) and 3-hydroxy-3-methyl-glutaryl-CoA (HMG-CoA) reductase inhibitors. The majority of these medications are in the initial phases of investigation in PAH.98 SURGICAL TREATMENTS Indicated in PAH when the response to medical therapy in not adequate. It is constituted by two Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 73 Table 3. Medical and patient societies in Latin America. Society Location (city, country) Hipertensión Pulmonar Argentina Asociación Civil (HIPUA) Asociación Brasileña de amigos y Familiares de portadores de Hipertensión Pulmonar Federación Boliviana de Hipertensión Pulmonar Organización de Hipertensión Pulmonar en Chile Fundación Colombiana de Hipertensión Pulmonar (FCHP) Asociación de Afectados de Hipertensión Pulmonar Asociación Nacional de Hipertensión Pulmonar (ANHP) Fundación Contra la Hipertensión Pulmonar Grupo de Apoyo Hispano para Pacientes de Hipertensión Pulmonar de Nueva York Sociedad Latina de Hipertensión Pulmonar Pulmonary Hypertension Association Grupo de Apoyo para Pacientes de Hipertensión Pulmonar en Español Asociación Mexicana de Hipertensión Pulmonar Grupo de Pacientes con Hipertensión Pulmonar A.C Fundación de Apoyo para la Hipertensión Pulmonar del Sureste Fundación de Pacientes con Hipertensión Pulmonar de Panamá Asociación Paraguaya de Escleroderma y Enfermedades Autoinmunes Federación Paraguaya de Hipertensión Pulmonar Asociación Médica Peruana de Hipertensión Pulmonar Grupo de apoyo para pacientes con Hipertensión Pulmonar en Puerto Rico Grupo de apoyo para pacientes con Hipertensión Pulmonar en República Dominicana Grupo de Apoyo para Pacientes con Hipertensión Pulmonar en Uruguay Fundación Venezolana de Hipertensión Pulmonar Buenos Aires, Argentina Sao Paulo, Brazil La Paz, Bolivia Santiago, Chile Santa Fé de Antioquía, Colombia Barcelona, Spain Madrid, Spain Madrid, Spain New York, USA Pembroke Pines, FL, USA Silver Spring, MD, USA South Florida, FL, USA Mexico City, México Mexico City, México Mérida, Yucatán, México Panamá City, Panamá Paraguay Asunción, Paraguay Lima, Perú San Juan, Puerto Rico, USA Santo Domingo, Dominican Republic Montevideo, Uruguay Caracas, Venezuela Adapted from Morales-Blanhir, et al. 2011.16 techniques: balloon atrial septostomy and lung or heart-lung transplantation. Ballon atrial septostomy is a palliative treatment in PAH patients. CR: IIa-LE: C in the majority of cases, this intervention is practiced in patients where there is therapeutic failure to the available medical treatments or as a palliative bridge towards lung transplantation. Which explains the high mortality rates 5-15% 56. Law, et al., in a study with 43 PAH patients, showed that septostomy provides improvement in symptomatology and hemodynamics (cardiac index and RAP).99 Heart-lung or lung transplantation in PAH has been evaluated only in prospective, non-controlled trials, due to the fact that formal controlled and randomized trials are not considered ethical in the absence of alternative treatment options. Survival rates in transplanted patients are similar in heartlung and unilateral or bilateral lung transplantation in PAH CR:I-LE:C.56 However, multiple transplant centers prefer to do bilateral lung transplantation. In a retrospective study with 219 patients divided according to their PH classification group (147 group I, 24 group III, 20 group IV and 20 group V); 67 patients received lung transplantation and 152 74 heart-lung transplantation. This study proved that there is good long term survival rate in terminal phase PH patients who receive a lung or heart-lung transplant. The results show preference in performing a heart-lung transplant in patients with RV failure or congenital shunts (pulmonary or systemic). Death due to bronchiolitis obliterans was less common in lung-heart than lung transplantations.100 CURRENT SITUATION In Latin America, there is a better organization of medical and patient PH societies (Table 3). Taking México as an example, there are several institutions: Rare Disease Mexican Federation (FEMEXER), Project “Pide un deseo” México and others, who took as their main objective to prioritize and raise awareness of rare diseases. Together they convinced the Mexican government to publish a decree in the Official Paper of the Mexican Federation, dated 01/30/2012, where the Health Secretary had to promote the availability of orphan drugs and broadcast recommendations to all health institutions to investigate and develop medications with effective potential. Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. Chin KM, Rubin LJ. Pulmonary arterial hypertension. J Am Coll Cardiol 2008; 51(16): 1527-38. Thenappan T, Shah SJ, Rich S, Gomberg-Maitland M. A USAbased registry for pulmonary arterial hypertension: 19822006. Eur Respir J 2007; 30(6): 1103-10. Tueller C, Stricker H, Soccal P, Tamm M, Aubert JD, Maggiorini M, et al. Epidemiology of pulmonary hypertension: new data from the Swiss registry. Swiss Med Wkly 2008; 138(2526): 379-84. Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med 2006; 173(9): 1023-30. Peacock AJ, Murphy NF, McMurray JJ, Caballero L, Stewart S. An epidemiological study of pulmonary arterial hypertension. Eur Respir J 2007; 30(1): 104-09. McLaughlin VV, Archer SL, Badesch DB, Barst RJ, Farber HW, Lindner JR, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension a report of the American College of Cardiology Foundation. Task force on expert consensus documents and the American Heart Association developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension Association. J Am Coll Cardiol 2009; 53(17): 1573-619. Galiè N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: The Task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Respir J 2009; 34: 1219-63. Kovacs G, Beghold A, Scheidl S, Olschewski H. Pulmonary arterial pressure during rest and exercise in healthy control subjects: a systematic review. Eur Respir J 2009; 34(4): 888-94. Valerio CJ, Schreiber BE, Handler CE, Denton CP, Coghlan JG. Borderline mean pulmonary artery pressure in patients with systemic sclerosis: Transpulmonary gradient predicts risk of developing pulmonary hypertension. Arthritis and Rheumatism 2013; 65(4): 1074-84. Pfarr N, Szamalek-Hoegel J, Fischer C, Hinderhofer K, Nagel C, Ehlken N, et al. Hemodynamic and clinical onset in patients with hereditary pulmonary arterial hypertension and BMPR2 mutations. Respiratory Research 2011; 12: 99. Loyd JE, Phillips JA III. Heritable pulmonary arterial hypertension. 2002 [Updated 2012 Dec 20]. In: Pagon RA, Adam MP, Bird TD, et al. (eds.). GeneReviews™ [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2013. Available from: http://www.ncbi.nlm.nih.gov/books/NBK1485 Rubin LJ, Simonneau G, Badesch D, Galie N, Humbert M, Keogh A, et al. The study of risk in pulmonary arterial hypertension. Eur Respir Rev 2012; 21(125): 234-8. Rosas-Romero MJ, Campos-Cerda R, Morales-Blanhir JE. Clasificación clínica de la hipertensión arterial pulmonar. Neumol Cir Torax 2006; 65(S4): S19-S27. Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 2009; 54(1 Suppl.): S43-S45. O’Callaghan DS, Humbert M. A critical analysis of survival in pulmonary arterial hypertension. Eur Respir Rev 2012; 21(125): 218-22. 16. Morales-Blanhir JE, Carmona-Rubio AE, Rosas-Romero MJ, Vergara GS, Dennis M, Ota AJS. Hipertensión pulmonar, perspectiva en Latinoamérica. Revista Española de Hipertensión Pulmonar 2011; 1(3): 65-8. 17. Londoño A. Aproximación al diagnóstico clínico de hipertensión pulmonar: signos y síntomas. Rev Col Neum 2010; 22(1 Suppl.): 11-13. 18. Morales-Blanhir JE, Campos-Cerda R, Rosas-Romero MJ. Proceso diagnóstico en la hipertensión arterial pulmonar. Neumol Cir Torax 2006; 65(S4): S28-S42. 19. Fisher MR, Forfia PR, Chamera E, Housten-Harris T, Champion HC, Girgis RE. Accuracy of Doppler echocardiography in the hemodynamic assessment of pulmonary hypertension. Am J Respir Crit Care Med 2009; 179(7): 615-21. 20. Vonk MC, Sander MH, van den Hoogen FH, van Riel PL, Verheugt FW, van Dijk AP. Right ventricle Tei-index: a tool to increase the accuracy of non-invasive detection of pulmonary arterial hypertension in connective tissue diseases. Eur J Echocardiogr 2007; 8(5): 317-21. 21. Bleeker GB, Steendijk P, Holman ER, Yu CM, Breithardt OA, Kaandorp TA, et al. Acquired right ventricular dysfunction. Heart 2006; 92(1 Suppl.): 14-8. 22. Forfia PR, Fisher MR, Mathai SC, Housten-Harris T, Hemnes AR, Borlaug BA, et al. Tricuspid annular displacement predicts survival in pulmonary hypertension. Am J of Respir Crit Care Med 2006; 174(9): 1034-41. 23. Freed BH, Patel AR, Lang RM. Redefining the role of cardiovascular imaging in patients with pulmonary arterial hypertension. Curr Cardiol Rep 2012; 14(3): 366-73. 2 4 . Resten A, Maitre S, Humbert M, Rabiller A, Sitbon O, Capron F, et al. Pulmonary hypertension: CT of the chest in pulmonary venoocclusive disease. Am J Roentgenol 2004; 183(1): 65-70. 25. Kadowaki T, Yano S, Kobayashi K, Araki K, Tokushima T, Yamadori I. Pulmonary capillary hemangiomatosis-like foci detected by high resolution computed tomography. Intern Med 2010; 49(2): 175-8. 26. Nistal MA, Martín MT. Imaging tests in chronic thromboembolic pulmonary hypertension. Arch Bronconeumol 2009; 45(6 Suppl.): 21-9. 27. Sanz J, Fernández-Friera L, Moral S. Imaging techniques and the evaluation of the right heart and the pulmonary circulation. Rev Esp Cardiol 2010; 63(2): 209-23. 28. Tunariu N, Gibbs SJ, Win Z, Gin-Sing W, Graham A, Gishen P, et al. Ventilation-perfusion scintigraphy is more sensitive than multidetector CTPA in detecting chronic thromboembolic pulmonary disease as a treatable cause of pulmonary hypertension. J Nucl Med 2007; 48(5): 680-4. 29. Blanco I, Barberá JA. Clinical and hemodynamic diagnosis in chronic thromboembolic pulmonary hypertension. Arch Bronconeumol 2009; 45(6 Suppl.): 15-20. 30. Armigliato M, Paolini R, Aggio S, Zamboni S, Galasso MP, Zonzin P, et al. Hyperthyroidism as a cause of pulmonary arterial hypertension: a prospective study. Angiology 2006; 57(5): 600-06. 31. Condliffe R, Kiely DG, Peacock AJ, Corris PA, Gibbs JS, Vrapi F, et al. Connective tissue disease-associated pulmonary arterial hypertension in the modern treatment era. Am J Respir Crit Care Med 2009; 179(2): 151-7. 32. Uribe M, Morales-Blanhir JE, Rosas-Romero MJ, Campos-Cerda R, Poo JL. Epidemiología, fisiopatología y diagnóstico de la hipertensión arterial pulmonar (HAP) en el cirrótico. Gaceta Médica de México 2012; 148: 153-61. Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 75 33. Porres-Aguilar M, Gallegos-Orozco JF, Garcia H, Aguirre J, Macías-Rodriguez RU, Torre-Delgadillo A. Pulmonary vascular complications in portal hypertension and liver disease: A concise review. Revista de Gastroenterología de México 2013; 78(1): 35-44. 34. Kawut SM, Krowka MJ, Trotter JF, Roberts KE, Benza RL, Badesch DB, et al. Clinical risk factors for portopulmonary hypertension. Hepatology 2008; 48(1): 196-203. 35. Escribano SP, Barberà JA, Suberviola V. Current diagnostic and prognostic assessment of pulmonary Hypertension. Rev Esp Cardiol 2010; 63(5): 583-96. 36. Hoeper MM, Lee SH, Voswinckel R, Palazzini M, Jais X, Marinelli A, et al. Complications of right heart catheterization procedures in patients with pulmonary hypertension in experienced centers. J Am Coll Cardiol 2006; 48(12): 2546-52. 3 7 . Morales-Blanhir J, Chaires LG, Rosas-Romero MJ. Cateterismo cardiaco derecho y test de reactividad vascular pulmonar. Revista Española de Hipertensión Pulmonar 2013; 3(2): 112-21. 38. Morales-Blanhir JE, Santos S, de Jover L, Sala E, Pare C, Roca J, Rodríguez-Roisin R, et al. Clinical value of vasodilator test with inhaled nitric oxide for predicting long-term response to oral vasodilators in pulmonary hypertension. Respir Med 2004; 98: 225-34. 3 9 . Marcus JT, Gan CT, Zwanenburg JJ, Boonstra A, Allaart CP, Götte MJ, et al. Interventricular mechanical asynchrony in pulmonary arterial hypertension: left-to-right delay in peak shortening is related to right ventricular overload and left ventricular underfilling. J Am Coll Cardiol 2008; 51(7): 750-7. 40. Van Wolferen SA, Marcus JT, Boonstra A, Marques KM, Bronzwaer JG, Spreeuwenberg MD, et al. Prognostic value of right ventricular mass, volume, and function in idiopathic pulmonary arterial hypertension. Eur Heart J 2007; 28(10): 1250-7. 41. Badano LP, Ginghina C, Easaw J, Muraru D, Grillo MT, Lancellotti P, et al. Right ventricle in pulmonary arterial hypertension: haemodynamics, structural changes, imaging, and proposal of a study protocol aimed to assess remodelling and treatment effects. Eur J Echocardiogr 2010; 11(1): 27-37. 42. Humbert M, Coghlan JG, Khanna D. Early detection and management of pulmonary arterial hypertension. Eur Respir Rev 2012; 21(126): 306-12. 43. Taichman DB, Mandel J. Epidemiology of pulmonary arterial hypertension. Clin Chest Med 2007; 28(1): 1-22. 44. McLaughlin VV, Shillington A, Rich S. Survival in primary pulmonary hypertension: the impact of epoprostenol therapy. Circulation 2002; 106(12): 1477-82. 45. Opravil M, Sereni D. Natural history of HIV-associated pulmonary arterial hypertension: trends in the HAART era. AIDS 2008; 22(3 Suppl.): S35-S40. 46. Humbert M, Sitbon O, Yaïci A, Montani D, O’Callaghan DS, Jaïs X, et al. Survival in incident and prevalent cohorts of patients with pulmonary arterial hypertension. Eur Respir J 2010; 36(3): 549-55. 47. Rasekaba T, Lee AL, Naughton MT, Williams TJ, Holland AE. The six-minute walk test: a useful metric for the cardiopulmonary patient. Intern Med J 2009; 39(8): 495-501. 48. Groepenhoff H, Vonk-Noordegraaf A, Boonstra A, Spreeuwenberg MD, Postmus PE, Bogaard HJ. Exercise testing to estimate survival in pulmonary hypertension. Med Sci Sports Exerc 2008; 40(10): 1725-32. 76 49. Hoeper MM, Pletz MW, Golpon H, Welte T. Prognostic value of blood gas analyses in patients with idiopathic pulmonary arterial hypertension. Eur Respir J 2007; 29(5): 944-50. 50. Sztrymf B, Souza R, Bertoletti L, Jaïs X, Sitbon O, Price LC, et al. Prognostic factors of acute heart failure in patients with pulmonary arterial hypertension. Eur Respir J 2010; 35(6): 1286-93. 51. Leuchte HH, Holzapfel M, Baumgartner RA, Ding I, Neurohr C, Vogeser M, et al. Clinical significance of brain natriuretic peptide in primary pulmonary hypertension. J Am Coll Cardiol 2004; 43(5): 764-70. 52. Takeda Y, Takeda Y, Tomimoto S, Tani T, Narita H, Kimura G. Bilirubin as a prognostic marker in patients with pulmonary arterial hypertension. BMC Pulm Med 2010; 22; 10:22. 53. Bendayan D, Shitrit D, Ygla M, Huerta M, Fink G, Kramer MR. Hyperuricemia as a prognostic factor in pulmonary arterial hypertension. Respir Med 2003; 97(2): 130-3. 54. Tang WH, Aytekin M, Hammel J, Hazen SL, Dweik RA. Sensitive cardiac troponin I predicts poor outcomes in pulmonary arterial hypertension. Eur Respir J 2012; 39(4): 939-44. 5 5 . Miura Y, Fukumoto Y, Sugimura K, Oikawa M, Nakano M, Tatebe S, et al. Identification of new prognostic factors of pulmonary hypertension. Circ J 2010; 74(9): 1965-71 56. Galié N, Palazzini M, Leci E, Manes A. Current therapeutic approaches to pulmonary arterial hypertension. Rev Esp Cardiol 2010; 63(6): 708-24. 57. Rich S, Kaufmann E, Levy PS. The effect of high doses of calcium-channel blockers on survival in primary pulmonary hypertension. N Engl J Med 1992; 327(2): 76-81. 58. Ortega H. Tratamiento con bloqueadores de los canales de calcio. Rev Col Neum 2010; 22(1 Suppl.): 50-2. 59. Cabrol S, Souza R, Jais X, Fadel E, Ali RH, Humbert M, et al. Intravenous epoprostenol in inoperable chronic thromboembolic pulmonary hypertension. J Heart Lung Transplant 2007; 26(4): 357-62. 60. McLaughlin VV, Shillington A, Rich S. Survival in primary pulmonary hypertension: the impact of epoprostenol therapy. Circulation 2002; 106(12): 1477-82. 61. Lang I, Gómez-Sánchez M, Kneussl M, Naeije R, Escribano P, Skoro-Sajer N, et al. Efficacy of long-term subcutaneous treprostinil sodium therapy in pulmonary hypertension. Chest 2006; 129(6): 1636-43. 6 2 . Benza RL, Seeger W, McLaughlin VV, Channick RN, Voswinckel R, Tapson VF, et al. Long-term effects of inhaled treprostinil in patients with pulmonary arterial hypertension: the treprostinil sodium inhalation used in the management of pulmonary arterial hypertension (TRIUMPH) study openlabel extension. J Heart Lung Transplant 2011; 30(12): 1327-33. 63. Tapson VF, Torres F, Kermeen F, Keogh AM, Allen RP, Frantz RP, Badesch DB, et al. Oral treprostinil for the treatment of pulmonary arterial hypertension in patients on background endothelin receptor antagonist and/or phosphodiesterase type 5 inhibitor therapy (The FREEDOM-C Study): A randomized controlled trial. Chest 2012; 142(6): 1383-90. 6 4 . Olschewski H, Hoeper MM, Behr J, Ewert R, Meyer A, Borst MM, et al. Long-term therapy with inhaled iloprost in patients with pulmonary hypertension. Respir Med 2010; 104(5): 731-40. 65. Galié N, Humbert M, Vachiéry JL, Vizza CD, Kneussl M, Manes A, et al. Effects of beraprost sodium, an oral prostacyclin analogue, in patients with pulmonary arterial hypertension: a Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. randomized, double-blind, placebo-controlled trial. J Am Coll Cardiol 2002; 39(9): 1496-502. Barst RJ, McGoon M, McLaughlin V, Tapson V, Rich S, Rubin L, et al. Beraprost therapy for pulmonary arterial hypertension. J Am Coll Cardiol 2003; 41(12): 2119-25. Kunieda T, Nakanishi N, Matsubara H, Ohe T, Okano Y, Kondo H, et al. Effects of long-acting beraprost sodium (TRK100STP) in Japanese patients with pulmonary arterial hypertension. Int Heart J 2009; 50(4): 513-29. Simonneau G, Torbicki A, Hoeper MM, Delcroix M, Karlócai K, Galié N, et al. Selexipag: an oral, selective prostacyclin receptor agonist for the treatment of pulmonary arterial hypertension. Eur Respir J 2012; 40(4): 874-80. Morrison K, Studer R, Ernst R, Haag F, Kauser K, Clozel M. Differential effects of Selexipag [corrected] and prostacyclin analogs in rat pulmonary artery. J Pharmacol Exp Ther 2012; 343(3): 547-55. Sitbon O, Morrell NW. Pathways in pulmonary arterial hypertension: the future is here. Eur Respir Rev 2012; 21(126): 321-7. Keogh A, McNeil K, Williams TJ, Gabbay E, Proudman S, Weintraub RG, et al. The bosentan patient registry: Long-term survival in pulmonary arterial hypertension. Intern Med J 2011; 41(3): 227-34. McGoon MD, Frost AE, Oudiz RJ, Badesch DB, Galie N, Olschewski H, et al. Ambrisentan therapy in patients with pulmonary arterial hypertension who discontinued bosentan or sitaxsentan due to liver function test abnormalities. Chest 2009; 135(1): 122-9. Bruderer S, Marjason J, Sidharta PN, Dingemanse J. Pharmacokinetics of macitentan in caucasian and japanese subjects: The influence of ethnicity and sex. Pharmacology 2013; 91(5-6): 331-8. Raghu G, Million-Rousseau R, Morganti A, Perchenet L, Behr J. MUSIC study group. Macitentan for the treatment of idiopathic pulmonary fibrosis: the randomised controlled MUSIC trial. Eur Respir J 2013; 42 (6): 1022-32. Pulido T, Adzerikho I, Channick RN, Delcroix M, Galié N, Ghofrani HA, et al. Macicentan and morbity and mortality in pulmonary arterial hypertension. N Engl J Med 2013; 369(6): 809-918. Galié N, Ghofrani HA, Torbicki A, Barst RJ, Rubin LJ, Badesch D, et al. Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med 2005; 353(20): 2148-57. Rubin LJ, Badesch DB, Fleming TR, Galiè N, Simonneau G, Ghofrani HA, et al. Long-term treatment with sildenafil citrate in pulmonary arterial hypertension: the SUPER-2 study. Chest 2011; 140(5): 1274-83. Blanco I, Gimeno E, Munoz PA, Pizarro S, Gistau C, Rodriguez-Roisin R, et al. Hemodynamic and gas exchange effects of sildenafil in patients with chronic obstructive pulmonary disease and pulmonary hypertension. Am J Respir Crit Care Med 2010; 181(3): 270-8. Barst RJ, Oudiz RJ, Beardsworth A, Brundage BH, Simonneau G, Ghofrani HA, et al. Tadalafil monotherapy and as add-on to background bosentan in patients with pulmonary arterial hypertension. J Heart Lung Transplant 2011; 30(6): 632-43. Jing ZC, Yu ZX, Shen JY, Wu BX, Xu KF, Zhu XY, et al. Vardenafil in pulmonary arterial hypertension: a randomized, double-blind, placebo-controlled study. Am J Respir Crit Care Med 2011; 183(12): 1723-9. Ghofrani HA, Galiè N, Grimminger F, Grünig E, Humbert M, Zhi-Cheng J, Keogh AM, et al. Riociguat for the treatment of 82. 83. 84. 85. 86. 87. 88. 89. 90. 91. 92. 93. 94. 95. 96. 97. pulmonary arterial hypertension. N Engl J Med 2013; 369: 330-40. Ghofrani HA, D’Armini AM, Grimminger F, Hoeper MM, Jansa P, Kim NH, et al. Riociguat for the treatment of chronic thromboembolic pulmonary hypertension. N Engl J Med 2013; 369: 319-29. Hoeper MM, Halank M, Wilkens H, et al. Riociguat for interstitial lung disease and pulmonary hypertension a pilot trial. Eur Respir J 2013; 41: 853-60. Bonderman D, Ghio S, Felix SB, Ghofrani HA, Michelakis ED, Mitrovic V, et al. On behalf of the left ventricular systolic dysfunction associated with pulmonary hypertension riociguat Trial (LEPHT) study group. Riociguat for patients with pulmonary hypertension due to systolic left ventricular dysfunction: A phase IIb double-blind, randomized, placebocontrolled, dose-ranging hemodynamic study. Circulation 2013; 128(5): 502-11. Rubin LJ. Treatment of pulmonary hypertension due to left heart failure with PAH-specific therapies: lessons from the right and LEPHT. Circulation 2013; 128(5): 475-6. Provencher S, Jais X, Yaici A, Sitbon O, Humbert M, Simonneau G. Clinical challenges in pulmonary hypertension: Roger S. Mitchell lecture. Chest 2005; 128(6 Suppl.): 622S-628S. Humbert M, Barst RJ, Robbins IM, Channick RN, Galiè N, Boonstra A, et al. Combination of bosentan with epoprostenol in pulmonary arterial hypertension: BREATHE-2. Eur Respir J 2004; 24(3): 353-9. McLaughlin VV, Oudiz RJ, Frost A, Tapson VF, Murali S, Channick RN, et al. Randomized study of adding inhaled iloprost to existing bosentan in pulmonary arterial hypertension. Am J Respir Crit Care Med 2006; 174(11): 1257-63. Porhownik NR, Al-Sharif H, Bshouty Z. Addition of sildenafil in patients with pulmonary arterial hypertension with inadequate response to bosentan monotherapy. Can Respir J 2008; 15(8): 427-30. Galiè N, Rubin LJ, Hoeper M, Jansa P, Al-Hiti H, Meyer G, et al. Treatment of patients with mildly symptomatic pulmonary arterial hypertension with bosentan (EARLY study): a double-blind, randomised controlled trial. Lancet 2008; 371(9630): 2093-100. Simonneau G, Rubin LJ, Galiè N, Barst RJ, Fleming TR, Frost AE, et al. Addition of sildenafil to long-term intravenous epoprostenol therapy in patients with pulmonary arterial hypertension: a randomized trial. Ann Intern Med 2008; 149(8): 521-30. McLaughlin VV, Benza RL, Rubin LJ, Channick RN, Voswinckel R, Tapson VF, et al. Addition of inhaled treprostinil to oral therapy for pulmonary arterial hypertension: a randomized controlled clinical trial. J Am Coll Cardiol 2010; 55(18): 1915-22. Abraham T, Wu G, Vastey F, Rapp J, Saad N, Balmir E. Role of combination therapy in the treatment of pulmonary arterial hypertension. Pharmacotherapy 2010; 30(4): 390-404. Rhodes CJ, Davidson A, Gibbs JS, Wharton J, Wilkins MR. Therapeutic targets in pulmonary arterial hypertension. Pharmacol Ther 2009; 121(1): 69-88. Rubin LJ, Santana LA. Treatment of pulmonary arterial hypertension: A look to the future. Avances Cardiol 2009; 29(2): 124-9. Souza R, Sitbon O, Parent F, Simonneau G, Humbert M. Long term imatinib treatment in pulmonary arterial hypertension. Thorax 2006; 61(8): 736. Reynolds PN. Gene therapy for pulmonary hypertension: prospects and challenges. Expert Opin Biol Ther 2011; 11: 133-43. Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78 77 98. Carmona-Rubio AE, Vergara GS, Morales-Blanhir JE. Hipertensión arterial pulmonar, ¿hacia dónde vamos en el tratamiento? Revista Española de Hipertensión Pulmonar 2013; 1(3): 10-3. 99. Law MA, Grifka RG, Mullins CE, Nihill MR. Atrial septostomy improves survival in select patients with pulmonary hypertension. Am Heart J 2007; 153(5): 779-84. 100. Fadel E, Mercier O, Mussot S, Leroy-Ladurie F, Cerrina J, Chapelier A, et al. Long-term outcome of double-lung and heart-lung transplantation for pulmonary hypertension: a comparative retrospective study of 219 patients. Eur J Cardiothorac Surg 2010; 38(3): 277-84. 78 Correspondence and reprint request: Dr. Jaime Eduardo Morales-Blanhir Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán Vasco de Quiroga, Núm. 15 Col. Sección XVI 14080, México, D.F. E-mail: [email protected] Received: September 26, 2013. Accepted: December 17, 2013. Morales-Blanhir JE, et al. Pulmonary arterial hypertension. Rev Invest Clin 2014; 66 (1): 65-78