Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
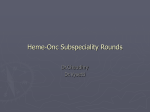
ANTIBODY MEDIATED ANEMIAS Shejal Patel DO Mr X is a 60 year old male with no past medical history and comes into the ER with complaints of fatigue and shortness of breath x 5 days. He takes no medications. He is noted on exam to be jaundiced and tachycardiac. He has no peripheral adenopathy or hepatosplenomegaly. What labs do you want? WBC 5 nml differential, Hgb 7, Plts 300 MCV 110 Retic 10% LDH elevated, hapto low TB 8, DB 2, AST/ALT/ALK phos nml Creatnine nml What will peripheral blood smear look like? Peripheral blood smear What other lab test do you want to make the diagnosis and explain how it is done? http://dxline.info/diseases/coombs-test/ DAT is + and reactive to IgG and non reactive to C3 (complement) What is the diagnosis? Reaction components Type of AIHA IgG alone warm antibody AIHA drug immune hemolytic anemia Complement alone warm antibody AIHA with subthreshold IgG deposition cold agglutinin disease paroxysmal cold hemoglobinuria drug-immune hemolytic anemia IgG plus complement warm-antibody AIHA mixed warm and cold antibody AIHA drug-immune hemolytic anemia Transfus Med Hemother. 2015 Sep; 42(5): 317–324. Published online 2015 Sep 11. You diagnose Mr. X with warm AIHA. Do you want any other workup? How will you treat Mr. X? 50% of AIHA is idiopathic. Other causes are lymphoproliferative disorders, autoimmune diseases, infections and tumors. Consider workup if anything by history or exam is concerning. Things to ask are about history of infections, recent transfusions, recent medications changes, any autoimmune disease symptoms or malignancy symptoms. First line treatment with corticosteroids Prednisone 1mg/kg/day given for a goal hemoglobin >10. Response generally occurs in 2nd week. If goal hgb of 10 not reached by 3rd week then second line treatment indicated. If hgb goal is obtained then steroid taper begins. It is suggested that prednisone taper should be reduced by 10-15 mg weekly to a daily dose of 20-30mg. Then decrease by 5mg every 1-2 weeks until dose of 15mg. Then subsequently by 2.5 mg every 2 week with aim of eventually no prednisone. Goal is for 3-4 months of <10mg of prednisone to help decrease incidence of relapse. Since patients will be on prolonged steroids, it is recommended that patients should get bisphosphonates, vitamin d, calcium. Patients often are also on folic acid. If rapid treatment needed then IV steroids can be used instead of oral. Blood, 16 Sept 2010, vol 116, number 11.. How I treat autoimmune hemolytic anemia s in adults. Haematologica, 2014; 99(10). Treatment of autoimmune hemolytic anemias Second line treatment Should consider workup at this point Can consider abdominal imaging to look at spleen and to look for adenopathy. Can check lupus anticoagulant and immunoglobulins. Splenectomy as 2nd line treatment Short term CR and PR can be seen in 2/3rd of the patients . 20% will be cured. Patients with hemolysis after splenectomy tend to require lower doses of corticosteroids than before splenectomy. Complications after splenectomy: infections, thromboembolism and pulmonary hypertension. Blood, 16 Sept 2010, vol 116, number 11.. How I treat autoimmune hemolytic anemia s in adults. Haematologica, 2014; 99(10). Treatment of autoimmune hemolytic anemias Second line treatment Rituxan 375mg IV on days 1, 8, 15, 22. Overall response rate is 70-80%(half CR and half PR) with a median duration of 1-2 years. Median time to response is 4-6 weeks although responses in first week or 3 months later is not uncommon. Often rituxan has to be repeated every 1-3 years. Of note there is a phase 3 randomized trial comparing 64 total patients on prednisone vs prednisone and rituxan in first line treatment. Blood, 21 May 2015, vol 125, number 21. The role of rituximab in adults with warm antibody autoimmune hemolytic anemia. Blood, 16 Sept 2010, vol 116, number 11.. How I treat autoimmune hemolytic anemia s in adults. Haematologica, 2014; 99(10). Treatment of autoimmune hemolytic anemias British Journal of Haematology Volume 163, Issue 3, pages 393-399, 23 AUG 2013 DOI: 10.1111/bjh.12541 http://onlinelibrary.wiley.com/doi/10.1111/bjh.12541/full#bjh12541-fig-0002 British Journal of Haematology Volume 163, Issue 3, pages 393-399, 23 AUG 2013 DOI: 10.1111/bjh.12541 http://onlinelibrary.wiley.com/doi/10.1111/bjh.12541/full#bjh12541-fig-0003 Further line treatments Azathioprine 100-150mg/day good responses in 40-60% of cases. Cyclophosphamide 100mg/day good responses in 40-60% of cases. Cyclosporine Danazol +/- prednisone can have success rate of 60-77% by reports. Cellcept ? IVIG-controversial, can use for CLL associated AIHA. ? Plasma exchange-as temporizing measure very controversial Blood, 16 Sept 2010, vol 116, number 11.. How I treat autoimmune hemolytic anemia s in adults. Haematologica, 2014; 99(10). Treatment of autoimmune hemolytic anemias Mr. X was started on prednisone 1mg/kg. His hemoglobin initially dropped to 5 range and he was symptomatic. You told the team it was okay to give the least incompatible blood, but just one unit at a time. Mr. X responded to steroids and was discharged home with followup as outpatient with you. Can there be DAT negative AIHA? IgA autoantibodies(won’t be detected by routine reagent)-can use mono-specific antisera against IgA to overcome DAT negativity. Low affinity IgG –low ionic strength solutions an be used to overcome DAT negativity. RBC bound IgG below the threshold of the test-can use other techniques that are more sensitive such as microcolumn, solid-phase, enzyme-linked and flow cytometry. Rare cases of IgM warm autoantibodies(severe hemolysis and more fatalities)- requires special tests dual DAT and Super coombs test. Still 10% AIHA remain DAT negative. Blood, 16 Sept 2010, vol 116, number 11.. How I treat autoimmune hemolytic anemia s in adults. Haematologica, 2014; 99(10). Treatment of autoimmune hemolytic anemias Generally a poor prognosis. Doesn’t respond to conventional therapies that work for IgG warm AIHA. Some case reports have shown effectiveness of treatment with rituxan, velcade, interferon and eculizumab. Why would splenectomy work for IgG warm AIHA but not IgM warm AIHA? AJH Vol 90,No1, Jan 2015. Refractory warm IgM-mediated autoimmune hemolytic anemia associated with Churg-Strauss syndrome responsive to eculizumab and rituximab. RBCs bound by IgG are recognized and cleared by macrophages in the spleen; therefore, splenectomy removes the site of RBC clearance and active hemolysis. However, RBCs in IgM-mediated AIHA undergo activation of complement and are not primarily cleared by macrophages in the spleen, but rather likely through ligation of complement receptors expressed on Kupffer cells in the liver. Thus, the liver rather than the spleen is thought to be the site of RBC clearance in IgM AIHA. Transfus Med Hemother 2015;42:303–310 Mrs Y is a 70 yo female with no past medical history who comes to see you for hemolytic anemia. DAT is + and reactive to C3 and non reactive to IgG. You are concerned for a cold autoimmune hemolytic anemia. Your differential is cold agglutin disease versus paroxysmal cold hemoglobinuria. How will you distinguish between them? Would a peripheral smear be of any help? Cold agglutinins are autoantibodies(typically IgM) that agglutinate red blood cells at 4 degree Celcius but may also act at warmer temperatures. Clinical manifestations: cold induced circulatory symptoms( livedo reticularis, raynaud disease, acrocyanosis, cutaneous necrosis). If suspect CAD then check cold agglutin titer(titer should be 1:256 or greater). Literature also suggests to check thermal amplitude however it is time consuming and often not needed for clinical practice. The thermal amplitude test is performed to determine the reactivity of a cold autoantibody at varying temperatures: 4° C, 22° C, 30° C, and 37° C. Cold autoantibodies that continue to agglutinate at temperatures greater than 30° C have the potential to be clinically significant regardless of the antibody titer. So if one has a low titer and low thermal amplitude then they don’t have CAD. ASH education program 2015. p385 Blood Aug 15 2013, vol 122, no 7. Cold Agglutin Disease Workup that should be done: spep, SIFE, immunoglobulins, c3 and c4, bone marrow biopsy and aspirate(looking for lymphoproliferative disorder). Treatment: supportive avoid cold temperatures, keep hands, feet and ears protected in cold environments. Any blood or fluids that patient gets through IV needs to be warm. Secondary to infection or malignancy: treat underlying cause. Symptomatic patients will need pharmacologic therapy. Rituxan-RR of 44-58%, 50% of patients will have a remission for a year. Is used first line. Reports of velcade, fludarabine(70% rr with rituxan even if mono rituxan didn’t work), bendamustine and eculizumab used. Plasmapheresis as a temporizing measure. Splenectomy not useful because hemolysis takes place in liver. Corticosteroids don’t work well RR 14% and if work needs high doses. ASH education program 2015. p385 Blood Aug 15 2013, vol 122, no 7. Cold Agglutin Disease Polyclonal cold reactive IgG antibodies bind to RBC surface protein ag termed P but do not agglutinate the erythrocytes. Hemolysis is entirely complementdependent and the temperature optimum for complement activation is at 37 degree Celsius. Donath-Landsteiner’s test is done, one sample of patient’s blood is incubated at 4 degree Celsius and then at 37 degree Celsius, while another sample is incubated at 37 degree Celsius without having been preincubated in the cold. If biphasic autoantibodies are present, hemolysis will be observed only in the sample preincubated at 4 degree Celsius. Often follows a viral infection. PCH is transient, so supportive care is treatment. BioMed Research Inernational. Volume 2015, Article ID 363278, Red Blood Cell Destruction in Autoimmune Hemolytic Anemia: Role of Complement and Potential New Targets for Therapy Mrs. Y workup shows that she has waldenstroms macroglobulinemia. Her cold agglutins titer is high. She got 4 doses or rituxan and her hemoglobin has improved and is stable. Questions?