Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
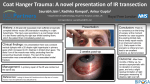
Case Report Synergistic Divergence: A Distinct Ocular Motility Dysinnervation Pattern Dr.Vishnu Suryaprakash, Dr.Shashikant Shetty, Aravind Eye Hospital Case Report A 6 year old female child came for review to our hospital with complaints of squinting in the left eye which was first noted by her parents when she was 3 months of age. She was the 3rd child of a non consanguineous marriage. Prenatal history was uneventful except for pregnancy induced hypertension. The baby was born after a full term by a normal delivery. Birth weight was normal. The baby had been immunized to date and developmental milestones were attained normally. On examination, she had a pronounced head turn to the right. Squinting of the left eye was noticed and it was about 30 degrees of exotropia and 15 degrees of hypertropia. On cover test the left eye did not take up central fixation. Visual acuity measured by Snellens chart was 6/6 in the right eye and 6/18 in the left eye. The child had been advised patching in the right eye 5 years back but had discontinued the practice for the past 2 years. Extraocular movements in the left eye were restricted in all directions of gaze, more so in adduction. Figure 1 shows pictures in all directions of gaze shows a LE exotropia and hypertropia in primary position. In attempted dextroversion the left eye shows an exaggeration of the exotropia along with Figure 1. Montage of extraocular movements an upshoot of that eye thus giving the appearance of both eyes diverging simultaneously. Discussion Synergistic divergence (SD) is a congenital ocular motility pattern characterized by paradoxical abduction during attempted horizontal gaze to the contralateral side1. This rare condition is generally unilateral and is always associated with limited adduction of the affected eye. The pathophysiology of anomalous abduction remains unclear but has been variously attributed to mechanical factors, anomalous innervation of the ipsilateral medial and lateral recti muscles2, and even anomalous cross innervation between the two lateral recti3. SD is usually an isolated ocular motility abnormality, but it has been described several times in conjunction with ocular motility phenotypes consistent with congenital fibrosis of the extraocular muscles types 1 (CFEOM1) and 3 (CFEOM3). Patients reported previously 1 had small medial recti on the affected side, perhaps due to maldevelopment of the medial rectus muscle. However, hypoplasia of the affected medial rectus alone would not explain abduction of the affected eye on attempted contralateral gaze. Figure 2 : Montage of brain imaging. Images of patient 1. (A) Axial CT image of orbit showing smaller medial rectus muscle on right. (✱) Right optic nerve; arrows: medial recti. (B) Coronal T2W MRI image of orbits again showing smaller medial rectus muscle on right. Arrows: medial recti. (C) Axial CISS MRI image showing normalappearing oculomotor nerves (arrows) bilaterally. A likely scenario is that a developmental anomaly in SD prevents the inferior branch of Vol. XIII, No.4, October - December 2013 22 Figure 2 : Montage of brain imaging. the oculomotor nerve from correctly innervating the medial rectus. The presence of synergistic divergence of the affected globe suggests that oculomotor fibers that should innervate the medial rectus actually innervate the lateral rectus, causing anomalous abduction on attempted contralateral gaze. Medial rectus denervation would explain a small medial rectus and absence of adduction on the affected side, and electromyographic studies in SD have documented reduced or absent firing in the medial rectus compatible with denervation1. Congenital cranial dysinnevation disorders, under which synergistic divergence falls result from the congenital absence or misdirection of specific brain stem lower motor neurons, leading to the loss of correct innervations of certain extraocular and/or cranial muscles, often with subsequent anomalous innervation (dysinnervation) by other nerves. SD has certain similarities to Duanes retraction syndrome, the most common CCDD ocular motility pattern. Both SD and DRS affect predominantly horizontal ocular muscles, they both occur unilaterally or bilaterally, and they sometimes coexist. However, the SD clinical phenotype differs from DRS in several ways. It involves a different motility pattern from all three DRS types; the muscle most involved is the medial rectus rather than the lateral rectus; and it does not include the DRS clinical hallmarks of globe retraction and lid fissure narrowing. DRS is more common in females for unclear reasons, whereas SD is more common in males in currently reported patients. SD deserves recognition as a distinct ocular motility pattern of CCDD, comparable to DRS but much less common. It is possibly caused by congenital denervation of the medial rectus with dysinnervation of the ipsilateral rectus, resulting in the characteristic anomalous abduction bilaterally on attempted contralateral gaze. References 1. Wilcox LM Jr, Gittinger JW Jr, Breinin GM. Congenital adduction palsy and synergistic divergence. Am J Ophthalmol. 1981;91:1–7. 2. Znajda JP, Krill AE. Congenital medial rectus muscle palsy with simultaneous abduction of the two eyes. Am J Ophthalmol. 1969; 68:1050 – 1052. 3. Freedman HL, Kushner BJ. Congenital ocular aberrant innervation: new concepts. J Pediatr Ophthalmol Strabismus. 1997;34:10-16.