Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
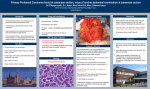
Peritoneal carcinomatosis. How to detect early signs M. Ave-Seijas V.Taboada L. Trillo R. Bouzas CHUVI-HospitalXeral-CíesVigo/ES Learning Objective To illustrate peritoneal carcinomatosis early manifestations with MDCT Special emphasis is placed on depicting the different peritoneal recesses using multiple projections through multiplanar reconstruction Background Peritoneal carcinomatosis is a challenge for MDCT, and variability in the sensitive to detect early sings is probably common between different radiologists We retrospectively reviewed MDCT findings of 33 patients with histopathological diagnosis of peritoneal carcinomatosis between 2005 and 2008, focusing this review in non ovarian tumors MDCT were interpreted by six radiologists. Only two of them were specialists in abdominal imaging Imaging Findings I- Peritoneal anatomy The peritoneal cavity is the virtual space between the visceral and parietal layers of the peritoneum The distribution of disease within the peritoneal cavity is determined by many factors, including gravity, changes in abdominal pressure with respiration and the peritoneal reflection, which may limit the spread of the disease [1,2,3] II.- Peritoneal carcinomatosis Diffuse metastatic spread within the peritoneal cavity Mestastases are usually from intra-abdominal primary neoplasms, such as ovarian carcinoma in women and stomach, colon, pancreas in both genders According to several studies the most common sites of peritoneal seeding include the pelvis, right lower quadrant, right paracolic gutter and the superior aspect of the sigmoid mesocolon [3,4] Metastases spread throughout the peritoneum in four ways: Direct tumor invasion or along peritoneal ligaments, mesenteries and omenta to non-contiguous structures Intraperitoneal seeding via ascitic fluid flow Lymphatic extension Haematogenous spread III.- Imaging techniques for the detection of peritoneal carcinomatosis There is not a completely optimal imaging technique for detecting peritoneal carcinomatosis Computed tomography(CT) is the most used tool. CT has a sensitivity less than 50% in detecting peritoneal metastases, but the specifity exceeds 85% and the sensitivity is improved in peritoneal deposits greater than 1 cm [5] Other imaging techniques: Abdominopelvic ultrasound can detect ascites and depict peritoneal implants, but it is an operatordependent technique and time consuming Magnetic Resonance Imaging(MRI) has a superior tissue contrast compared with CT, but its spatial resolution is lower. Recent studies say that comparing with singlephase helical CT, it shows an advantage in depicting tumor involving the peritoneum, omentum and bowel [6,7] Positron Emission Tomography-CT(PET-CT) has limitations in detecting mucinous tumors and can have false-positive results in cases of acute inflammation or active tissue repair NOWADAYS, CT IS THE IMAGING STANDARD TO EVALUATE PERITONEAL CARCINOMATOSIS, AND MRI AND PET-CT ARE CONSIDERED USEFUL BUT NOT FUNDAMENTAL [8,9] IV- CT findings of peritoneal carcinomatosis Ascites, usually loculated Thickening of the parietal peritoneum, either smooth or nodular Scalloping of the liver or splenic surfaces Alteration of the greater omentum Affectation of the mesentery Bowell involvement WE ALSO ASSESS EXTRAPERITONEAL ABDOMINAL DISEASE SECONDARY TO HEMATOGONOUS SPREAD, INCLUDING LIVER METASTASES Ascites usually loculated Fig. 2. Axial CT scan shows hepatic loculated fluid. Fig. 1. Coronal CT scan shows lateroconal left fascia thickening and large amounts of ascites with atypical distribution. Fig. 3. Axial CT scan shows fluid in the culde-sac. Typical place of ascites. Thickening of the parietal peritoneum Fig. 4. a) Axial and b) coronal CT scans shows bilateral thickening of lateroconal fascia and loculation of subhepatic fluid in both paracolic gutters. A a b Thickening of the parietal peritoneum Fig. 5: Bilateral thickening of lateroconal fascia “Scalloping” of the liver or splenic surfaces Implants located between the diaphagmatic peritoneum and the liver or the spleen Fig.6. Axial CT scan shows scalloping of the hepatic margin and a large amount of ascites. Alteration of the greater omentum Soft-tissue permeation of omental fat, nodules or thickened omentum with diffuse tumor infiltration (omental cake) Fig.7. Axial CT scan shows soft-tissue permeated omental fat. Fig.8. Axial CT scan shows omental nodules. Fig.9. Axial CT scan shows diffuse omental infiltration (omental cake). Alteration of the greater omentum a b Fig. 10. a) Axial CT scan shows soft-tissue permeation of omental fat. b) Axial CT scan after surgery shows bowell dillatation( )with nodular thickened wall( )due to extensive carcinomatosis. Initial changes (a) were interpreted as postsurgery changes. Affectation of the mesentery Soft-tissue permeation of mesenteric fat, nodules or masses and lymph nodes increased in number or size Fig.11. Axial CT scan shows soft-tissue permeation of mesenteric fat Combination of signs Fig. 12. Coronal CT scan shows mesenteric masses and loculated ascites Fig.13. Axial CT scan shows bilateral lateroconal fascia ( ) thickening, loculated fluid ( )and mesenteric masses ( ). Fig. 12. Axial CT scan shows complex cystic mass in lesser sac ( ) and peritoneal tumour implant ( ). Fig. 13. Coronal MIP CT scan shows small mesenteric lymph nodes. Bowell involvement Thickening and nodularity of the bowel wall Fig.14. Axial CT scan shows thickening of the bowel wall and loculated fluid. V.- Data: These 33 patients were divided into two groups. In one group (A) peritoneal carcinomatosis was diagnosed on the first MDCT, and in the other group (B) we included those who had at least one MDCT performed 3 to 6 months before the establishment of the diagnosis of carcinomatosis. In this last group we actively searched for conclusive signs of carcinomatosis and possible causes of delayed diagnosis, especially due to misperceptions, and therefore false negatives. We illustrate the differences between those groups. We use 10 abdominal MDCT obtained in patients with no cancer history as control group for comparison We settle a search pattern in the abdomen dividing it into quadrants (right upper quadrant:RUQ, left upper quadrant:LUQ, right lower quadrant:RLQ and left lower quadrant:LLQ) We analyzed a change in the fascia morphology, the liver surface, mesentery, omentum, bowel wall and the presence of ascites, lymph nodes, and liver metastasis, and illustrate evolution between both MDCT PRIMARY TUMOR Group A: unknown (5), gastric (5), colon (2), pancreas (2), neuroendocrine (1), lung (1) endometrium (1) Grupo B: gastric (4), colon (4), unknoum(3), carcinoid (2) pancreas (1) hypernephroma (1), gallbladder(1) Percentages of CT findings in two groups Group A Group B Ascites 88,2 % 43,8% Parietal Peritoneum 47% 75% “scallopig” 11,8% 6,2% Greater Omentum 35,3% 25% Merentery 47% 12,5% Mesentery lymph nodes 47% 62,5% liver MTS 23,53% 12,5% Only one of the patients in the control group showed peritoneal involvement, as free fluid secondary to adherences, which was detected in all quadrants CT findings in group A (peritoneal carcinomatosis diagnosed on the first MDCT) N:17 patients RUQ LUQ RLQ LLQ Ascites: 15 12 9 11 14 1 9 7 4 3 Parietal Peritoneum: 8 Perihepatic Paracolic gutter “scallopig”:2 8 patients had mesenteric lymph nodes, and 4 had liver metastasis 1 Greater Omentum:6 Soft-tissue Nodules Omental Cake 0 5 1 0 5 1 0 3 1 0 3 1 Merentery:8 Soft-tissue Nodules 5 2 3 1 2 0 2 0 CT findings in group B (MDCT performed 3 to 6 months before the establishment of the diagnosis of carcinomatosis) 10 patients had mesenteric lymph nodes, and 2 had liver metastasis N:16 patients RUQ LUQ RLQ LLQ Ascites:7 3 3 5 3 8 9 1 7 1 - 1 - - - Parietal Peritoneum 12 Perihepatic Paracolic gutter “scallopig”1 Greater Omentum:4 Soft-tissue Nodules Omental Cake 2 0 0 2 - 1 - 1 - Merentery:2 So nodules 2 0 1 - 1 - - CASE 1 a b Fig. 1. A 67 year-old man with colon carcinoma. a) Axial CT scan shows a small parietal peritoneal implant in the right hepatic lobe ( ). b) Coronal CT scan shows the parietal peritoneal implant. We observe an ondulation of the hepatic surface ( ) caused by muscular slip of the diaphragm that can mimic the appearance of peritoneal thickening. Fig. 2. Axial and coronal consecutives CT scans show a small parietal peritoneal implant in the right hepatic lobe, larger in last CT. The diagnosis of peritoneal carcinomatosis was established on the last CT a b Fig. 3. a) Coronal and b) coronal MIP CT scans show mesenteric small lymph nodes. Small lymph nodes are associated with early signs of peritoneal carcinomatosis. CASE 2 a Fig. 1. A 65 year-old man with T4 N1 M1 gastric cancer that was understaged as T4 N1 M0. a) Coronal CT scan shows gastric wall thickening and small local lymph nodes. b) Axial CT scan shows discrete permeation of omental fat with separation of a small bowell loop from the abdominal wall (early sign of omental disease) b b a Fig. 2. Images obtained in 65 year-old man with T4 N1 M1 gastric cancer after surgery. a) Coronal CT scan shows gastric wall thickening and mesenteric small lymph nodes. b) Axial CT scan shows nodular thickened omentum. CASE 3 b a Fig. 1. A 69 year-old man with colon carcinoma. a) Coronal CT scan shows thickening of the parietal peritoneum ( ) in the right hepatic lobe and nodular thickening of the paracolic gutter ( ). Also b) axial CT scan shows nodular thickening of the perihepatic parietal peritoneum. c) Coronal CT shows a mesenteric mass( c A radiologist with experience in abdominal imaging interpreted the images ) Fig. 2. Images obtained 6 months before . a) Coronal CT scan shows subtle thickening of the parietal peritoneum ( ) in the right hepatic lobe and nodular thickening of the paracolic gutter ( ). b) Axial CT scan shows subtle nodular thickening of the perihepatic parietal peritoneum. c) Coronal CT demonstrates small mesenteric masses( ). These subtle findings were not described by the radiologist CASE 4 a Fig. 1. A 60 year-old man with metastatic adenocarcinoma. a) Axial CT scan shows a minimum detectable amount of free perihepatic fluid and hepatic metastases. In b) Axial CT scan, free intraperitoneal fluid is not detected in other peritoneal spaces b a b Fig. 2. Images obtained 3 months later. a) Axial CT scan shows increase of amount of free perihepatic fluid. b) Coronal CT scan shows free intraperitoneal fluid in perihepatic space, periesplenic space, both paracolic gutters and pelvis. b a Fig. 3. Images obtained 6 months later in the same patient. a) Coronal, b) axial, and c) axial CT scan show large amounts of ascites in all compartments: perihepatic space, periesplenic space, mesentery, both paracolic gutters and pelvis. c VI.-Discussion In group A (peritoneal carcinomatosis diagnosed on the first MDCT), the most common CT finding of peritoneal carcinomatosis was ascites, present in 88,2 % of patients, without predilection for any abdominal quadrant In group B (who had at least one MDCT performed 3 to 6 months before the establishment of the diagnosis of carcinomatosis ), the most common CT finding (75% of patients) was thickening of the parietal peritoneum, predominating in the right upper quadrant Soft-tissue permeation of omental fat is most frequent in group A, and nodules or omental cake in group B Multiple and small lymphadenopathy, in conjunction with other signs, should warn of the presence of peritoneal dissemination We must pay special attention to the search for subtle signs of peritoneal carcinomatosis in stomach and colon carcinomas (non ovarian tumors) Moreover, in patients with minor volume ascites, it allows a better evaluation of the parietal or visceral peritoneum The use of multiple projections through multiplanar reconstruction aids to the detection of a subtle thickening of the peritoneal recesses Interpretation of MDCT by abdominal imaging radiologists may reduce the false negative of peritoneal carcinomatosis Conclusions The diagnosis of peritoneal carcinomatosis is a real challenge for the radiologist. Natural history can teach us how to integrate signs into a standard report Our study is retrospective and its validity must be confirmed by prospective studies. But this study shows the most common anatomical sites where you could find subtle signs of peritoneal carcinomatosis To increase the sensitivity for the detection of peritoneal carcinomatosis, allowing better surgical or medical oncology treatment, the radiologist should focus in the upper right quadrant and the greater omentum Bibliography 1.-Coakley FV, Hricak H. Imaging of peritoneal and mesenteric disease: key concepts for the clinical radiologist. Clin Radiol 1999;54:563-74. 2.- Healy JC,Reznek RH.The peritoneaum,mesenterias and pathological processes. Eur Radiol 1998;8:886-900. 3.-K Gordon, WK Lee and O Hennessy.Computed tomography manifestations of peritoneal diseases .Australasian Radiology 2005; 49: 269-27. 4.-Raptopoulos V, Gourtsoyiannis N. Peritoneal carcinomatosis. Eur Radiol 2001;11:2195-206 5.- Imaging in oncology.2004. 6.-Low RN, Semelka RC, Worawattanakul S et al. Extrahepatic abdominal imaging in patients with malignancy: comparison of MR imaging and helical CT in 164 patients. Magn Reson Imaging. 2000 Aug;12(2):269-77. 7.- de Bree E, Koops W,Kröger R, MD 2, et al. Peritoneal carcinomatosis from colorectal or appendiceal origin: Correlation of preoperative CT with intraoperative findings and evaluation of interobserver agreement. J Surg Oncol.2004;86:6473 8.- Yan TD,Morris DL,Kusamura S,et al.Preoperative investigations in the management of peritoneal surface malignancy with citoreductive surgery and perioperative intraperitoneal chemoterapy:expert consensus statement. J Surg Oncol .2008;98:227-227. 9.-Santiago González-Moreno,Luis Gonzalez-Bayón,Gloria Ortega-Pérez and Concepción González-Hernand.Imaging of Peritoneal Carcinomatosis. Cancer J. 2009 May-Jun;15(3):184-9 . 10.-Walkey MM, Friedman AC,Sorotra P, Radecki PD.CT manifestations of peritoneal carcinomatosis.AJR 1988;150: 1035-41.