Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
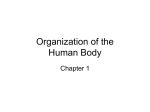
Cervical Spine Injuries in Polytrauma Patients: What the Surgeon Wants to Know. Poster No.: C-1655 Congress: ECR 2016 Type: Educational Exhibit Authors: E. Federici, C. Dell'atti, V. Martinelli, D. Beomonte Zobel, M. Bartocci, N. Magarelli, L. Bonomo; Rome/IT Keywords: Education, Diagnostic procedure, CT, Conventional radiography, Musculoskeletal spine, Emergency, Trauma DOI: 10.1594/ecr2016/C-1655 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 32 Learning objectives • • • To review the spectrum of cervical spine injuries, from the craniocervical junction through the subaxial spine. To highlight the role of multidetector computed tomography (MDCT) for diagnosis of cervical spine injuries in polytrauma patients. To identify what the surgeon needs to know about the injury to predict outcomes and plan management. Background Cervical spine injuries occur in 5%-10% of patients with polytrauma and it is a common problem with a wide range of severity from minor ligamentous injury to frank osteoligamentous instability with spinal cord injury. It is essential that radiologists recognize findings that distinguish injuries with ligamentous instability or that require surgical stabilization from those that are classically stable and can be treated with a conservative treatment. Craniocervical Junction (CCJ) and Subaxial Cervical Spine The CCJ is an anatomical region that is formed by complex articulations involving the occipital condyles and the first two vertebra. These joints are supported by several ligaments, including the anterior longitudinal ligament, the anterior atlantoaxial and atlantooccipital ligaments, the cruciform ligaments, the alar ligaments, and the tectorial membrane, which extends cranially as the cephalic extension of the posterior longitudinal ligament (Fig1) [1]. Craniocervical biomechanical continuity depends on the integrity of the skull base, atlas, and axis and their attaching ligaments. Page 2 of 32 Fig. 1: Anatomy of the craniocervical region. References: Atlas of Human Anatomy Netter. A full conventional RADIOGRAPHIC EXAMINATION of the cervical spine as a minimum includes a lateral view, antero-posterior (AP) view and an AP odontoid peg view. The lateral view should include the cervical-thoracic junction. Normal measurements have been determined for many of the bone relationships and soft-tissue contours at the craniocervical junction and are valuable for excluding upper cervical spine injury. Harris et al [2,3] have identified a practical method for evaluating the normal osseous relationships at the craniocervical junction using lateral conventional radiographs. They determined the upper limits of normal for adults and children by measuring the basiondens interval (tip of dens to basion) and the basion-posterior axial line interval (basion to posterior axial line, a vertical line drawn along the posterior aspect of the subdental body of C2). In 95% of adults, the basion-dens interval was less than 12 mm, and in 98%, the basion was situated no more than 12 mm anterior or 4 mm posterior to the posterior axial line (Fig 2). An abnormal distance between the dens or posterior axial line and the basion suggests failure or insufficiency of the alar ligaments, tectorial membrane, or both. Page 3 of 32 Fig. 2: Normal relationships within the craniocervical junction: the basion-dens interval (a), the posterior axial line (b) and the basion-posterior axial line interval (c). References: Institute of Radiology, Catholic University - Rome/IT Alignment is assessed by visually assessing the SPINAL LINES on the lateral radiograph (Fig.3). They should all appear smooth and without interruption [4]. • • • • The anterior spinal line passes along anterior borders of the vertebral bodies and the anterior aspect of the odontoid peg. The distance between the anterior arch of C1 and the odontoid peg should not exceed 3 mm in adults and 5 mm in children. The posterior spinal line passes along the posterior borders of the vertebral bodies. The junction of the laminae with the spinous processes forms the spinolaminar line. The lamina of C2 is normally up to 2 mm posterior to the spinolaminar line. The distance between the spinous processes should be roughly equal at all levels, taking into account the normal downward slope of the C7 spinous process. Page 4 of 32 Fig. 3: Lateral radiograph shows normal alignment of the subaxial spinal lines: the anterior marginal line (1), the posterior marginal line (2), the spinolaminar line (3) and the posterior spinous line (4). References: Institute of Radiology, Catholic University - Rome/IT Noting the central position of the spinous processes assesses alignment on the AP radiograph (Fig.4). The spinous processes of the cervical spine may appear bifid; this is a normal anatomical finding at many levels and in this situation the central point of the posterior elements is the point midway between the two tubercles of the spinous process. Page 5 of 32 Fig. 4: Antero-posterior radiograph shows normal alignment of spinous processes. References: Institute of Radiology, Catholic University - Rome/IT When assessing the AP through mouth odontoid peg view (Fig.5), normal alignment is demonstrated by noting that the lateral margins of the C1-C2 facet joints are symmetrically aligned with no overlap. Page 6 of 32 Fig. 5: The distance from the dens (A,3) to the lateral masses of C1 (A,2) should be equal bilaterally. B: Open-mouth or odontoid view. References: Institute of Radiology, Catholic University - Rome/IT Soft-tissue swelling is assessed on the lateral radiograph. Superior to the level of the larynx the distance between the anterior aspect of the vertebral bodies and the posterior aspect of the air in the oropharynx should be no greater than one-third of the AP diameter of a vertebral body width. Inferior to the level of the larynx (usually C3 or C4 and frequently seen due to calcification in the laryngeal cartilage) it should be no greater than the AP diameter of the vertebral body [4]. CT of the cervical spine should include the spine from the cranio-cervical junction to the level of the third thoracic vertebral body. The precise imaging parameters will depend on the CT system being used, but an appropriately thin slice thickness should be selected to allow good-quality coronal and sagittal reformats. The alignment and soft-tissue swelling is assessed on these reformats using the same basic principles as the interpretation of the conventional radiograph. The axial sections are particularly useful for diagnosing bone fractures. The presence of malalignment and soft-tissue swelling will often give an indication of ligamentous disruption in the absence of any bony injury but this is not always the case. If there is continued clinical concern following a normal CT, then MRI is warranted as CT cannot exclude a purely ligamentous disruption. Page 7 of 32 Images for this section: Fig. 1: Anatomy of the craniocervical region. © Atlas of Human Anatomy Netter. Page 8 of 32 Fig. 2: Normal relationships within the craniocervical junction: the basion-dens interval (a), the posterior axial line (b) and the basion-posterior axial line interval (c). © Institute of Radiology, Catholic University - Rome/IT Page 9 of 32 Fig. 3: Lateral radiograph shows normal alignment of the subaxial spinal lines: the anterior marginal line (1), the posterior marginal line (2), the spinolaminar line (3) and the posterior spinous line (4). © Institute of Radiology, Catholic University - Rome/IT Fig. 4: Antero-posterior radiograph shows normal alignment of spinous processes. Page 10 of 32 © Institute of Radiology, Catholic University - Rome/IT Fig. 5: The distance from the dens (A,3) to the lateral masses of C1 (A,2) should be equal bilaterally. B: Open-mouth or odontoid view. © Institute of Radiology, Catholic University - Rome/IT Page 11 of 32 Findings and procedure details MDCT is used throughout major trauma centers as the initial screening examination for high-risk patients who are suspected of having cervical spine trauma, and it is increasingly incorporated into whole-body CT protocols in the evaluation of polytrauma. MDCT is often sufficient for making the determination of whether surgery is necessary or not, but important determinants of management (disk herniations, ligament injuries or epidural hematoma) are not well evaluated with CT but are clearly depicted at MR imaging. INJURIES OF THE CRANIOCERVICAL JUNCTION Craniocervical Dissociation Craniocervical dissociation is an umbrella term that describes both • • complete dislocations, which are common in fatal motor vehicle trauma, and subluxation or distraction injuries, which may be subtle and potentially survivable. By definition, atlanto-occipital dissociation is an unstable injury with severe ligamentous disruption and is usually accompanied by severe neurologic deficit. Traumatic atlantooccipital dissociation is more common and more survivable in skeletally immature pediatric trauma patients [1]. Lateral radiographic findings in atlanto-occipital distraction injuries include soft-tissue swelling and pathologic convexity of the soft tissues anterior to C2 (generally greater than 10 mm in thickness) and a basion-dens interval greater than 12 mm in children under the age of 13 years. [5]. Occipital Condyle Fractures (OCF) Anderson and Montesano [6] introduced the most widely used radiologic classification system for occipital condyle fractures, describing three different patterns of injury: • Type I OCF is an impaction-type fracture resulting in a comminution of the occipital condyle, with or without minimal fragment displacement. The mechanism of injury is believed to be axial loading of the skull onto the atlas Page 12 of 32 • • with or without lateral bending. It is considered a stable entity because the tectorial membrane and contralateral alar ligament are intact; however, bilateral lesions may be unstable (Fig.6) [7]. Type II OCF is part of a more extensive basioccipital fracture, involving one or both occipital condyles. The mechanism of injury is a direct blow to the skull. An intact tectorial membrane and alar ligaments preserve stability [7] Type III OCF is an avulsion type of fracture near the alar ligament resulting in medial fragment displacement from the inferomedial aspect of the occipital condyle into the foramen magnum. The mechanism of injury is forced rotation, usually combined with lateral bending (Fig.7). After occipital condylar avulsion, the contralateral alar ligament and tectorial membrane may be stressed and "loaded" resulting in a partial tear or complete disruption. Thus, the type III OCF is considered a potentially unstable injury [7]. Fig. 6: Axial (a), coronal (b) and sagittal (c) CT images show a Type I OCF (yellow arrows). References: Institute of Radiology, Catholic University - Rome/IT Page 13 of 32 Fig. 7: Axial (a) and coronal (b) CT images show a Type III OCF (yellow arrows). References: Institute of Radiology, Catholic University - Rome/IT Fractures of the Atlas Jefferson introduced the first classification system for atlas fractures, which is still in use with some modifications [8,9]. • • • • • Type I: fractures of the posterior arches alone. Type II: isolated fractures of the anterior arch. Type III: bilateral posterior arch fractures with unilateral or bilateral anterior arch fracture (classic Jefferson burst). Type IV: fractures of the lateral mass. Type V: transversely oriented anterior arch fractures resulting from avulsion of the longus colli or atlantoaxial ligament. Fractures of the atlas are usually mechanically stable and rarely result in neurologic injury. For atlas fractures, associated cervical spine fractures and the integrity of the transverse ligament are the main determinants of the need for surgical intervention (Fig.8) [9]. Classic Jefferson fracture Page 14 of 32 Burst fractures of the atlas are thought to result from axial loading. This bursting fracture is the result of force transmitted from the vertex of the skull through the occipital condyles to the lateral masses of the atlas. The fracture pattern results in outward displacement of the lateral masses, a finding that indicates possible injury to the transverse ligament. To prevent atlantoaxial dissociation, Jefferson fractures may require surgical stabilization if the transverse ligament is compromised or the anterior arch is appreciably displaced. Fig. 8: Axial CT images show a Jefferson fracture with fractures of the anterior arch and the posterior arch (a, yellow arrows) of atlas and demonstrate the avulsion of a bony fragment by the transverse ligament (b, yellow arrows). References: Institute of Radiology, Catholic University - Rome/IT Odontoid Fractures. Odontoid fractures are classically divided into three groups (Fig.9), as introduced by Anderson and D'Alonzo [10]. • • Type I: fractures represent an avulsion fracture of the odontoid tip at the insertion of the alar ligament. They are rare with a limited number of case reports in the medical literature. The fracture is typically described as stable. Type II: odontoid fractures represent the most common pattern of dens injury and occur through the base of dens at the junction of the C2 vertebral body (Fig.10). The fracture is traditionally considered unstable, often requiring immediate surgical stabilization. Page 15 of 32 • Type III: fractures extend into the C2 vertebral body (Fig.11). Fracture displacement is common; however, fewer than 8% of patients with Type III fractures develop nonunion after non-surgical immobilization alone. Thus, Class III data support halo immobilization for 6-8 weeks as a first-line management [11]. Fig. 9: Odontoid fracture classification by Anderson and D'Alonzo. References: Institute of Radiology, Catholic University - Rome/IT Page 16 of 32 Fig. 10: Sagittal (a) and coronal (b) CT reformats show a Type II odontoid peg fracture (yellow arrows). References: Institute of Radiology, Catholic University - Rome/IT Fig. 11: Sagittal (a) and coronal (b) CT reformats show a Type III odontoid peg fracture (yellow arrows). Page 17 of 32 References: Institute of Radiology, Catholic University - Rome/IT Hangman Fractures. A hangman's fracture is a traumatic spondylolisthesis of C2 where a fracture occurs through both pedicles, separating the posterior elements from the vertebral body (Fig.12). The C2 vertebral body subluxes anteriorly relative to C3 but the posterior elements remain normally aligned. Because the spinal canal effectively widens in AP diameter at the level of slip there is often little or no neurological injury despite sometimes marked spondylolisthesis.[4] These fractures can occur as the result of either compressive hyperextension or distractive hyperflexion and can involve any part of the axis ring, including laminae, pedicles, or part of the posterior wall of the axis body. Page 18 of 32 Fig. 12: Axial (a), coronal (b) and sagittal CT images show a hangman fracture (yellow arrows). References: Institute of Radiology, Catholic University - Rome/IT Atlantoaxial Rotatory Subluxation and Fixation Traumatic rotatory subluxation and fixation are well documented in children but are rare in adults [12]. Higher degrees of rotatory subluxation have a greater propensity to develop into rotatory fixation and have a greater need for surgical reduction. Fielding and Hawkins [13] have described a number of configurations of atlantoaxial rotatory fixation. • • • • Type I: atlantoaxial rotatory fixation occurs within the normal physiologic range, with intact alar and transverse ligaments.The dens acts as the pivot, and there is no anterior displacement of the atlas. In type II: atlanto-axial rotatory fixation, the transverse ligament is injured. Anterior displacement of the atlas should not exceed 5 mm because of restraint from the alar ligament. In type III: atlantoaxial rotatory fixation, both the transverse and alar ligaments are deficient. The configuration is similar to type II, but anterior displacement of the atlas exceeds 5 mm. Type IV: describes the rare circumstance in which a deficient odontoid is present, resulting in posterior displacement of the atlas. The spinal canal may be compromised in types II to IV. INJURIES OF THE SUBAXIAL CERVICAL SPINE Hyperflexion Injuries Flexion forces to the spine can cause rupture of the posterior elements. Typically there may be little in the way of anterior soft-tissue swelling since all the soft-tissue injury occurs posteriorly. There may be a fracture of the anterior aspect of the vertebral body, the flexion teardrop fracture. The bony fragment is typically relatively large and elongated in the cranio-caudal direction of the spine, which distinguishes it from the hyperextension tear drop, which is usually a small fragment. There is a strong association with severe neurological injury [4]. Bilateral subluxation of the facet joints can occur with little in the way of bony injury. The facet joints can lock in a displaced position, the so-called perched facet joints. Page 19 of 32 A hyperflexion force with resistance of the posterior paraspinal muscles can produce a 'clay-shoveler's' fracture (Fig.13). This is a fracture of the lower cervical or upper thoracic spinous process and is one of the few cervical fractures that can be considered stable [4]. Page 20 of 32 Fig. 13: Sagittal CT reformat shows a 'clay-shoveler's' fracture (yellow arrow). References: Institute of Radiology, Catholic University - Rome/IT Page 21 of 32 Hyperflexion Rotation Injury A rotational force applied along with flexion can result in a unilateral dislocation of a facet joint. Malalignment in the sagittal plane may be very minimal. CT demonstrates the 'reverse hamburger' sign on the axial sections through the facet dislocation [4]. Hyperextension Injuries Extension force to the spine can result in rupture of the anterior longitudinal ligament and posterior displacement and angulation. There is typically soft-tissue swelling anterior to the spine at the site of the ligamentous disruption. There may be an associated hyperextension teardrop fracture (Fig.14), which is usually a small fragment. Neurological abnormality implies that a hyperextension dislocation occurred at the time of injury though the spine may be relatively normally aligned subsequently [4]. Page 22 of 32 Fig. 14: Lateral radiograph shows a hyperextension teardrop fracture of C2 (yellow arrow). References: Institute of Radiology, Catholic University - Rome/IT Page 23 of 32 Images for this section: Fig. 6: Axial (a), coronal (b) and sagittal (c) CT images show a Type I OCF (yellow arrows). © Institute of Radiology, Catholic University - Rome/IT Page 24 of 32 Fig. 7: Axial (a) and coronal (b) CT images show a Type III OCF (yellow arrows). © Institute of Radiology, Catholic University - Rome/IT Fig. 8: Axial CT images show a Jefferson fracture with fractures of the anterior arch and the posterior arch (a, yellow arrows) of atlas and demonstrate the avulsion of a bony fragment by the transverse ligament (b, yellow arrows). Page 25 of 32 © Institute of Radiology, Catholic University - Rome/IT Fig. 9: Odontoid fracture classification by Anderson and D'Alonzo. © Institute of Radiology, Catholic University - Rome/IT Page 26 of 32 Fig. 10: Sagittal (a) and coronal (b) CT reformats show a Type II odontoid peg fracture (yellow arrows). © Institute of Radiology, Catholic University - Rome/IT Page 27 of 32 Fig. 11: Sagittal (a) and coronal (b) CT reformats show a Type III odontoid peg fracture (yellow arrows). © Institute of Radiology, Catholic University - Rome/IT Fig. 12: Axial (a), coronal (b) and sagittal CT images show a hangman fracture (yellow arrows). © Institute of Radiology, Catholic University - Rome/IT Page 28 of 32 Fig. 13: Sagittal CT reformat shows a 'clay-shoveler's' fracture (yellow arrow). © Institute of Radiology, Catholic University - Rome/IT Page 29 of 32 Fig. 14: Lateral radiograph shows a hyperextension teardrop fracture of C2 (yellow arrow). © Institute of Radiology, Catholic University - Rome/IT Page 30 of 32 Conclusion In the emergency department, accurate diagnosis of cervical spine fractures by the radiologist working closely with the orthopaedic is crucial for ensuring prompt and effective treatment and preventing neurologic deficits in polytrauma patients. Personal information References 1. Dreizin D, Letzing M, Sliker CW, Chokshi FH, Bodanapally U, Mirvis SE, et al.: Multidetector CT of blunt cervical spine trauma in adults. Radiographics 34:1842-1865,2014 2. Harris JH, Carson GC, Wagner LK. Radiologic diagnosis of traumatic occipitovertebral dissocia- tion. 1. Normal occipitovertebral relationships on lateral radiographs of supine subjects. AJR Am J Roentgenol 1994; 162:881-886. 3. Harris JH, Carson GC, Wagner LK, Kerr N. Ra- diologic diagnosis of traumatic occipitovertebral dissociation. 2. Comparison of three methods of detecting occipitovertebral relationships on lateral radiographs of supine subjects. AJR Am J Roent- genol 1994; 162:887-892. 4. Grainger & Allison's Diagnostic Radiology, 6th edition, Churchill Livingstone, 2015. 5. Deliganis AV, Baxter AB, Hanson JA, et al. Radiologic spectrum of craniocervical distraction injuries. RadioGraphics 2000;20:S237-S250. 6. Anderson PA, Montesano PX. Morphology and treatment of occipital condyle fractures. Spine (Phila Pa 1976) 1988;13(7):731-736. 7. Leone A, Cerase A, Colosimo C et al. Occipital condylar fractures: a review. Radiology 2000; 216: 635-644. 8. Anderson LD, D'Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg Am 1974;56:1663-74. 9. KakarlaUK,ChangSW,TheodoreN,Sonntag VK. Atlas fractures. Neurosurgery 2010;66(suppl 3):60-67. 10. Anderson LD, D'Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg Am 1974;56:1663-74. 11. Julien TD, Frankel B, Traynelis VC, Ryken TC. Evidence-based analysis of odontoid fracture management. Neurosurg Focus 2000;8:e1. 12. Roche CJ, O'Malley M, Dorgan JC, Carty HM. A pictorial review of atlanto-axial rotatory fixa- tion: key points for the radiologist. Clin Radiol 2001;56(12):947-958. Page 31 of 32 13. Fielding JW, Hawkins RJ. Atlanto-axial rotatory fixation (fixed rotatory subluxation of the atlanto- axial joint). J Bone Joint Surg Am 1977;59(1): 37-44. Page 32 of 32