Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
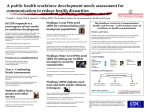
2186 Commentary Development of an Integrated Approach to Cancer Disparities: One Cancer Center’s Experience Karen M. Emmons,2 Karen Burns White,1 and Edward J. Benz3 1 Dana-Farber/Harvard Cancer Center, 2Harvard School of Public Health, and 3Harvard Medical School, Boston, Massachusetts The National Cancer Institute’s (NCI) Cancer Centers Program has provided a critical infrastructure for discovery related to the causes, prevention, and treatment of cancer. This program spends more than $200 million annually to fund 39 comprehensive cancer centers in 24 states. The substantial resources provided to cancer centers throughout the country provides the NCI with a significant opportunity to influence key areas of need. For example, the cancer center guidelines have been used to increase the emphasis on translational research which has the potential to affect patient care, to increase interdisciplinary research and inclusion of population approaches to cancer prevention and early detection, to standardize quality control and safety protections for clinical trials, and to promote cooperation among centers. The guidelines also ensure that all cancer centers continuously focus on accrual to clinical trials and take steps to increase population representativeness among clinical trial participants. Although the guidelines do not explicitly require cancer centers to address disparities, the increasing recognition of persistent cancer disparities as an urgent problem requiring extensive and systematic effort has led to increased scrutiny of the way in which cancer centers use their significant resources related to addressing disparities (1). A recent Institute of Medicine (2) review of the NIH’s role in identifying solutions to persistent disparities highlights the importance of leveraging existing resources and structures that have a potential to make an impact. An emphasis on the role of cancer centers in addressing cancer disparities beyond minority accrual to trials is much needed, given that cancer disparities among low income groups and some racial/ethnic minority groups are unrelenting and, to date, intractable. In responding to this challenge, cancer centers must determine how to use limited resources in a time of flat funding and shrinking budgets. The DanaFarber/Harvard Cancer Center (DF/HCC) has restructured flexible resources to provide an integrated Cancer Epidemiol Biomarkers Prev 2007;16(11):2186 – 92 Received 3/7/07; revised 7/17/07; accepted 8/29/07. Grant support: P30 CA06516 and U01 CA114644 from the National Cancer Institute, and U48 DP000064 from the National Cancer Institute and the Centers for Disease Control and Prevention. Requests for reprints: Karen M. Emmons, Center for Community-Based Research, Harvard School of Public Health and Dana-Farber Cancer Institute, 44 Binney Street, Boston, MA 02115. Phone: 617-632-2188; Fax: 617-632-5690. E-mail: [email protected] Copyright D 2007 American Association for Cancer Research. doi:10.1158/1055-9965.EPI-07-0211 structure within the cancer center related to disparities, and to create incentives for investigators to refocus on disparities. We offer this commentary to describe this approach, which may be useful to others. This is still a work in progress—our success will only be measured over time by our ultimate effect over time on cancer disparities in the communities we serve. An earlier NCI review of the cancer center had been critical of the low rate of accrual of minority patients to clinical trials and the Center’s limited emphasis on cancer disparities. Although there were researchers in the Harvard system who focused on disparities, they did not necessarily focus their work on cancer, and were largely uninvolved in the cancer center. Furthermore, virtually all of the limited efforts in cancer disparities resided in discipline-based programs (e.g., population science). There was little likelihood that the situation would improve without a deliberate and strategic emphasis on disparities. The leadership recognized both the challenge and opportunity of this situation, and set about to create an emphasis on cancer disparities that would permeate all aspects of the cancer center’s functioning. This was particularly challenging given that the DF/HCC includes seven separate institutions, all of whom had their own strategies for addressing disparities. These forces led to the creation of the Initiative to Eliminate Cancer Disparities (IECD), a comprehensive, integrated, Center-wide initiative designed to lower the existing barriers that were impeding the study of factors contributing to, and solutions for, cancer disparities. A primary goal of the IECD is to transform the way DF/ HCC member institutions work together on cancer disparities, in part by creating an intentional focus on cancer issues within communities of color. The Initiative was designed by first examining the structural barriers both within the cancer center and in the broader research community related to addressing disparities. Such barriers included disciplinary and funding silos that have largely relegated research in disparities to population sciences, lack of mechanisms for ensuring the faculty’s cultural competency, having a very limited number of minority faculty, and a perception among some basic and clinical scientists that cancer disparities were not relevant to them. We identified strategies to address each of these barriers, and have also identified and tried to take advantage of factors at the federal level that could facilitate our efforts (see Table 1). We believe it is critical in such an effort to engage the cancer center membership fully, including researchers in areas that typically do not consider disparities within Cancer Epidemiol Biomarkers Prev 2007;16(11). November 2007 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2007 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention Table 1. Structural barriers and strategies used to address them Structural barriers Factors facilitating adoption at federal level Disciplinary silos NIH emphasis on transdisciplinary science Funding silos Perceived lack of relevance NIH and other federal agencies emphasize the importance of research on disparities National focus on disparities NCI attention to minority accrual to trials Limited expertise in cancer disparities across DF/HCC programs Need cultural competency training mechanism for clinical research faculty Limited numbers of minority faculty Minority supplement mechanism Strategies used within DF/HCC Cost considerations DF/HCC nodal point structure requires emphasis on interdisciplinary and transdisciplinary research None DF/HCC leadership structure expanded to integrate a focus on disparities in all decision-making processes, via appointment of an Associate Director of the IECD, who reports to the Cancer Center Director 15% FTE of senior faculty Heavily publicize federal funding opportunities focus on disparities, and provide mentoring related to application development None; uses existing communication mechanisms Use cancer center pilot research mechanism to stimulate disparities Nine pilot projects funded focused on disparities (out of 30 total awards) Set disparities research as a priority for fund-raising/development efforts None Prominent national speakers provide keynote addresses on disparities None; funded with existing mechanisms Thought-leaders within basic and clinical science programs engaged in considering ways their work could address disparities None Identify potential added value of initiative to disease programs (e.g., provide assistance with increasing diversity of applicants on training grants; expand faculty recruitment opportunities with minority faculty hiring supplement None Develop more relevant algorithms for assessing progress None Conduct internal pilot projects to determine opportunities for improving accrual Some staffing costs Identify disparities researchers and engage them in cancer-related outcomes None Identify and engage basic and clinical scientists targeting topics related to disparities (e.g., genetic factors and potential treatment targets related to high breast cancer mortality in young African-American women) None Established cultural competency training initiative for clinical research faculty Subcontract with local cultural competency expert to offer initial didactic program and to develop a cancerrelevant e-tool Opportunities to use NIH minority supplement mechanisms identified None Minority faculty recruitment supplements $100,000 per faculty position; one position allocated per year from development resources Cancer Epidemiol Biomarkers Prev 2007;16(11). November 2007 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2007 American Association for Cancer Research. 2187 2188 The DF/HCC Initiative to Eliminate Cancer Disparities their domain (e.g., basic scientists). It is clear that the causes of cancer disparities are multifactorial, and that effective solutions will require involvement from a range of disciplines. For example, there are well-documented disparities in lung cancer morbidity and mortality among African-Americans. It is clear that lung cancer has specific behavioral risk factors that require the development of effective behavioral interventions (e.g., smoking prevention and cessation). However, there may be important genetic factors at play in determining both smoking cessation and lung cancer treatment outcomes (3-9). Health care services research also plays an important role, with recent studies showing that hospital factors are associated with disparate lung cancer outcomes for African-Americans (10, 11). There is increasing information across a range of disease areas showing the potential role of cell regulation and gene-environment interactions across a range of cancers. We have sought to use data such as this to emphasize to all cancer center members the potential role they could play in our efforts to reduce cancer disparities. Initiative to Eliminate Cancer Disparities: Key Components There are five key strategies that we have used to develop the IECD including (a) stimulating research in cancer disparities; (b) developing new metrics for evaluating minority accrual to trials; (c) development of a cultural competency training program for cancer center members; (d) identifying a coordinated set of outreach activities; and (e) student training and recruitment/ retention of minority faculty. A summary of the activities within each of these strategies, and benchmarks developed to judge our progress, is provided in Table 2. Development of a Research Program in Cancer Disparities. We have stimulated research in disparities by creating a research program-in-development focused on cancer disparities, bringing in a leader of that program who is an expert in disparities but is relatively new to cancer, and identifying a co-leader with cancer expertise. Although it has been tempting to push this program to fully deemed status quickly, it has been given time to mature. Three years following its initiation, it is now in the process of going to full status in a position of considerable strength. Applications for NCI and Centers for Disease Control and Prevention mechanisms designed to address disparities have helped us to build an infrastructure for this work (e.g., NCI-funded Community Network Program grant and U56; Centers for Disease Control and Prevention/NCI-funded Cancer Prevention and Control Research Network). This program has 51 affiliated cancer center members, a research portfolio of $16.7 million, and active collaborations with four disease programs. We have also extensively used our Developmental Funds to seed pilot research projects in disparities. Available mechanisms include annual competitive solicitations for large pilot projects ($75,000/y for 2 years) and on-going availability of smaller developmental opportunities for new and innovative ideas ($10,000). Both types of awards have been used for stimulating collaborations in disparities. This has also been an important mechanism to help our junior minority investigators establish their research programs, thus increasing their competi- tiveness for federal funding. We have funded nine pilot projects focused on disparities (total cost, $930,000). To date, approximately half of these pilots have led to extramural funding. We have also used pilot monies available through other funding mechanisms (e.g., U56, Community Network Program, Cancer Prevention and Control Research Network) to stimulate disparities research within the Center (12 additional pilots funded). Effective engagement of the disease programs is critical to the long-term success of our disparities research efforts. As one example, we have collaborated with leaders of the Gastrointestinal Cancer Specialized Programs of Research Excellence to develop a research program focused on vitamin D as a potential mechanism in colorectal cancer disparities. This collaboration provided an opportunity for the Gastrointestinal Cancer program investigators to access a population-based cohort of 1,500 low income, racial and ethnic minority adults that had been part of a community-based colorectal cancer screening study. There was great value added for the Gastrointestinal Cancer investigators in this collaboration because it provided a significant economy of scale by allowing work with an existing cohort that had been recruited and characterized. Through the process of developing the application, we were able to increase the disease program leaders’ knowledge of and interest in disparities. Furthermore, we recently added a prostate cancer component to the vitamin D work, as proposed by one of our minority junior faculty members and his fellow. This component was funded by the DF/HCC developmental monies. Development of New Metrics for Evaluating Clinical Trials Accrual. The 2004 Cancer Center Support Grant guidelines requires Centers to account for minority patient accrual to therapeutic trials to determine whether accrual figures are proportional to the cancer patient population in the Cancer Center’s primary catchment area. However, our Center, like most others, had historically compared our accrual against the overall minority population, rather than against the subpopulation of minority group members who had developed cancer. There had been no effort to determine the racial/ethnic minority representation of the local cancer patient population, and thus it was impossible to accurately judge our success in this area. By using data from The Massachusetts Community Health Information Profile database, which is maintained by the state Department of Public Health and Tumor Registry data, we could determine the representation of different racial and ethnic minority groups among all cancer patients diagnosed in our catchment area. Furthermore, we could identify the hospitals at which those patients received their treatment, and therefore, we could characterize much more specifically the effectiveness of our participation in cancer care delivery for patients of color. We further stratified these analyses by cancer site. Thus, in addition to tracking the rate of accrual to trials among minority and non – minority patients, we could identify the percentage of minority cancer patients in our catchment area that are on trial. This is a much more relevant figure than overall accrual rates. Our goal is to provide on-going feedback to disease program leaders in order to engage them in efforts to improve accrual rates and to increase their program’s interest in disparities research. Cancer Epidemiol Biomarkers Prev 2007;16(11). November 2007 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2007 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention Table 2. IECD components and benchmarks used to assess progress IECD Component Establish robust research program in cancer disparities Benchmark Status Articulate disparities research agenda Completed; 51 cancer center members affiliated with program Engage leaders of two to three disease programs Have actively engaged gastrointestinal, gynecologic, lung, and breast programs; other efforts under way Assist investigators who are developing grants in disparities Program leadership has mentored investigators submitting more than 20 grant applications Use DF/HCC developmental funds to seed disparities research Nine pilot grants on disparities funded to date through DF/HCC; 12 pilots funded leveraging other resources (two additional under review) Establish junior faculty seminar series focused on research in cancer disparities Monthly seminars for 2 y; attract 15 to 20 participants regularly Increase disparities-focused extramural funding Identifying opportunities to embed cancer disparities into disease-based programs. Create new research theme in gene expression with explicit focus on health disparities Develop new metrics for evaluating minority accrual to trials Metrics developed representing accrual relative to the Boston minority cancer patient population Completed Develop a cultural competency training program for cancer center members Conduct a didactic cultural competency program Completed initial program; annual activities in all care-giving institutions Implement and evaluate a cancer-relevant cultural competency e-learning tool Initial pilot with faculty completed; pilot and evaluation with fellows under way Establish a Community Engagement Committee across all seven DF/HCC institutions Has met monthly for 6 y; draws on Community Benefits resources of each institution Develop strategic partnerships with key community groups related to cancer and clinical trials education Faith-based initiative under way Faith-based cancer education toolkit developed and being implemented in participating churches Identify a coordinated set of outreach activities Annual emphasis on National Minority Cancer Awareness Week Student training Recruitment/retention of minority faculty Develop a patient navigator network to provide support and share resources across navigators in the DF/HCC care-giving institutions Patient navigator network developed and meeting quarterly for 3 y Develop robust training mechanism CURE program in place for 6 y Develop tracking system for present/past student progress Completed At least 70% of CURE students will pursue further education/careers in science and cancer More than 90% of CURE students are meeting this goal Secure funding for minority postdoctoral fellowships Completed; funding in place for 3 y; from shared institutional funds Establish mechanism and funding for minority faculty recruitment supplements Completed; four awarded during the first 5 y; anticipating five additional positions in current funding cycle Develop mechanism to collect data and regularly report on race/ethnicity of DF/HCC faculty Completed Cancer Epidemiol Biomarkers Prev 2007;16(11). November 2007 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2007 American Association for Cancer Research. 2189 2190 The DF/HCC Initiative to Eliminate Cancer Disparities Implementation and Evaluation of a Cultural Competency Training Program. The goal of the emerging field of cultural competence in health care is to improve the providers’ ability to understand, communicate with, and care for patients from diverse backgrounds. Following a needs assessment, we determined that an explicit effort in cultural competency was needed, and thus, contracted with a local expert to develop a cultural competency training curriculum consisting of group sessions in the context of regular program meetings. We contracted with Quality Interactions, an e-learning tool for crosscultural care, to add cancer cases to this tool, which expanded its appropriateness for our membership. We conducted a pilot of the tool with selected disease programs, and are now rolling it out on a broader basis. An evaluation plan has been developed in order to determine the effect of the program on patient-related outcomes. Identify a Coordinated Set of Outreach Activities. Recognizing the importance and role of the community, we have prioritized building linkages with the community and creating a community voice within the cancer center. Our initial aim was to bring together the cancer-related resources and activities of the seven individual institutional offices charged with addressing disparities and/or community relations. Our approach to engaging the community is 3-fold: (a) increase community access to research through clinical trials education; (b) implement and support innovative programs that will reduce the barriers to care; and (c) develop a mechanism that will provide a standing forum to solicit the viewpoints of the community. Our clinical trials education efforts included producing an educational video and brochure, which has received numerous awards. The video is distributed to all patients considering enrollment in a clinical trial. In addition, we are actively partnering with two community coalitions to provide clinical trials education across the city of Boston. The Center must fill another central role in the development of community-based initiatives to reduce barriers to care, i.e., the implementation of support programs. We conduct a number of activities to inform the community about research and resources available within the Center, including Public Health Grand Rounds at community health centers, special events in recognition of National Minority Cancer Awareness Week, and community health fairs. We have a partnership with the faith-based community, and regularly participate in meetings of the ministerial leaders and in health events sponsored by the various churches. With our faith-based partners, we have developed a toolkit that includes a number of ‘‘plug and play’’ resources (e.g., bulletin inserts, informational materials, material to support health-oriented sermons and health ministries, and resource material). We are also connecting the health ministries to cancer screening resources (e.g., our mobile mammography van), and leveraging other resources within the DF/HCC institutions. For each of our activities, we develop a community-based advisory board to ensure that community needs and perspectives are considered. Train the Next Generation of Cancer Researchers, and Recruit and Retain Minority Faculty Our training efforts target postdoctoral fellows, as well as high school juniors and seniors and undergraduate students with demonstrated aptitude in the sciences. The centerpiece of our training effort for the latter group is a Continuing Umbrella of Research Experiences (CURE) supplement to our cancer center grant. The program has two tracks, (a) a 2-year program, and (b) a summer-only internship. Both opportunities include an intensive 9-week summer experience. Two-year students continue in a part-time capacity during the academic year. Based on their areas of research interest, students are paired with appropriate DF/HCC faculty mentors for a full-time, hands-on research experience. Students attend scientific research seminars, journal review sessions, and prepare an article on their research. They are also encouraged and supported to present at scientific meetings/science fairs and to participate in opportunities for publications. Although based on interest, most students are placed in basic science research environments, some of the participants also gain experience in clinical and population sciences. Several of our CURE students have gone on to work in their mentors’ laboratories following graduation, which has positioned them quite competitively for graduate and medical school. Many of our faculty have predoctoral and postdoctoral training grants, and having access to a cadre of outstanding minority students who are receiving mentoring in career development has been of great interest to them. We are currently developing better linkages between our student training programs and our postdoctoral training programs. To date, 90% of our CURE students have continued their education in science upon completion of our program. Ninety percent of the high school students have gone on to science-focused undergraduate majors, and 84% of the college students are either working in the science field or pursuing advanced degrees. As noted in a recent National Academies report, there is little national data available on the success of these programs to benchmark our success against (12). Our internal benchmarks are for 70% of students to continue their work and/or education in science. We also actively participate in local efforts to improve science education and training for minority students. Through a U56 cancer center/minority-serving institution partnership grant, we work with our minority-serving institution partner, the University of MassachusettsBoston, to develop their minority training programs. Increasing the rigor of scientific training of their minority students will have a direct effect on DF/HCC’s opportunities for training and hiring minority students interested in cancer. This partnership has played an instrumental role in the University of MassachusettsBoston’s applications for three major grant programs targeting training of minority students that have recently been funded (‘‘Bridges to Baccalaureate’’, ‘‘Graduate Assistance in Areas of National Need’’, and ‘‘Urban Massachusetts Louis Stokes Alliance for Minority Participation Project’’; total costs: $3,546,426). At the postdoctoral level, we have partnered with the Harvard School of Public Health to support candidates interested in cancer research through the Yerby Postdoctoral Fellowship Program. The Yerby Program is a bridge between academic training in health-related disciplines and entry-level faculty positions in public health, particularly for trainees from under-represented backgrounds. The Program engages fellows in extensive professional development opportunities, with a strong Cancer Epidemiol Biomarkers Prev 2007;16(11). November 2007 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2007 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention emphasis on the development of research and teaching skills. We support up to two Yerby fellows per year in the cancer center. To date, we have funded three students on this mechanism, and the two that have completed their training are now junior faculty at strong institutions. Current efforts are focused on increasing the rate at which these fellows are retained within the Harvard system. We also support the recruitment efforts of DF/ HCC training grants by providing resources to develop and implement minority recruitment plans through the monitoring of DF/HCC-wide success, and development of center-wide strategies when needed. To diversify our faculty, we have actively used cancer center resources for the recruitment of minority faculty. Developmental funds are used to provide supplements of $100,000 on a competitive basis to institutional recruitment packages for searches in which minority faculty are identified as leading candidates. In our previous funding cycle, four very strong researchers from under-represented minority backgrounds were recruited on this mechanism. We are currently evaluating the effect of this strategy, but anticipate extending the use of developmental resources for minority faculty recruitment in the current funding period. We have also conducted a number of activities related to the career development of our minority faculty, trainees, and those interested in cancer disparities. We initiated a seminar series for junior researchers interested in disparities to come together to meet senior faculty, learn about research resources, obtain feedback on research in progress, and forge new collaborations. The series is organized by one of our minority post-docs, which provides an excellent leadership opportunity. In partnership with the Office for Diversity and Community Partnership at Harvard Medical School, we sponsor an Annual Junior Investigators’ Health Disparities Research Poster Session, which provides an opportunity to showcase our trainees’ and junior faculty’s research in disparities. This event typically includes a talk by a very high-profile national leader, which draws significant numbers of faculty and encourages active interactions with poster presenters. Finally, across all levels, we engage in significant mentoring activities. All minority faculty hired under the DF/HCC supplemental mechanism have an identified mentor and twice-yearly evaluations of progress and the quality of the mentoring relationship. We particularly focus on providing junior faculty and postdoctoral fellows from under-represented backgrounds opportunities to become involved in article preparation and grantwriting. This is a highly effective strategy, which, although involving significant time from the IECD leadership, has great potential for long-term pay-off. Some of our senior faculty have obtained K05 grants, which has provided important support to enable high levels of engagement in mentoring. In the past year, the leadership has provided active mentoring related to more than 20 grant applications, including K-awards, R03s, R01s, and U56 pilot projects. A large percentage of these have been funded or have received competitive scores. Organizational Structure The IECD operates through a subcommittee structure, which is supported by Senior Leadership and Adminis- tration. It is led by the Associate Director of the IECD, a full Professor who serves as a voting member on the senior leadership group for the DF/HCC. Having a seat on the leadership team insures that key issues related to cancer disparities are addressed in all DF/HCC activities and budgetary decisions. Furthermore, it provides an opportunity to consider each program’s efforts related to disparities during program review, and to consider the potential effects on disparities when new requests for funding with DF/HCC resources are made. The IECD is co-led by a Deputy Associate Director, a senior administrator with substantial community-based experience. Together, the IECD leadership staffs subcommittees, engages in substantial outreach across the cancer center membership and to the local communities, and oversees collaborative endeavors and student training. Each of the key components of the IECD is led by a senior leader within the cancer center, representing basic, clinical, and population sciences. These leaders have significant institutional knowledge, as well as influence within the cancer center and their own institutions. This has been a very effective strategy for securing high-level support of the Initiative. Evaluation of Impact We have two primary strategies for evaluating the effects of the IECD over the long-term. First, the DF/HCC leadership supports an External Advisory Board (EAB) for this effort, separate from the overall DF/HCC EAB. We felt that having an EAB specific to the IECD was critical in order to have the initiatives guided by investigators with more extensive expertise in disparities, and to have a more extensive review of each IECD component. The primary responsibility of the IECD’s EAB is to provide recommendations to the leadership for establishing priorities and identifying new areas of opportunity for the initiative. The report from the IECD EAB is provided to the DF/HCC’s overall leadership, and is included as part of the annual report to the overall cancer center EAB. Second, within each of the key components of the initiative, we have identified benchmarks that serve as metrics for evaluating progress within that area (see Table 2). These are reviewed on a regular basis, and corrective action is taken when needed. We are making significant progress towards meeting our benchmarks. Our research program is small but thriving, and is in the process of going to full program status. It will be critical that in the next phase of its development, we continue to seek out ways to keep our members fully engaged, and to extend our interactions with additional disease programs that represent areas of persistent disparities. We have successfully developed a new metric for evaluating our clinical trials accrual. It is somewhat complex to evaluate these data on an annual basis because we are dependent on sources outside of the cancer center for the benchmarking data. The ultimate test of this strategy will be whether we can use this data to address changes in accrual patterns on an on-going basis. Our cultural competency training program has been moving more slowly than we would like, in part because of the difficulties with developing a meaningful evaluation plan that will affect not only changes in our knowledge, but also on changes in our practice. We have recently engaged Cancer Epidemiol Biomarkers Prev 2007;16(11). November 2007 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2007 American Association for Cancer Research. 2191 2192 The DF/HCC Initiative to Eliminate Cancer Disparities a cultural competency and quality of care expert as a member of our team, which should greatly facilitate our movement in this area. Our Community Engagement Committee has developed a strong relationship with a large faith-based network and, with their significant input, has developed resources to support this effort. The challenge for this committee is to fully engage the community in a lasting, meaningful way with very limited staffing resources. We believe that provision of materials that can be used by well-established community channels and providing technical assistance on an ongoing basis will be an effective strategy. Our student training program is robust and thriving. We are not far enough out yet to fully know the effects, but early indicators suggest that we will meet or exceed our longterm goals. Although minority faculty recruitment is a top priority, our progress here has been slower than hoped. Our mechanism for providing supplements does not always synch well with the timing of recruitments, and the cancer center is not an appointment-granting body— this is a function of the seven individual institutions. Although substantial resources have been allocated to this strategy ($400,000 in the previous funding cycle; $500,000 in the current cycle), it is clear that hiring one minority faculty member per year will not make an impact in the context of a 900-member cancer center. We are committed to this approach as one step towards stimulating progress and emphasizing the commitment of cancer center leadership, but are currently developing other strategies to stimulate more progress in this area. Summary Recognizing the need to address the complex problems associated with cancer disparities, the DF/HCC leadership has made a commitment of considerable faculty, staff, and financial resources to tackling this issue. Senior faculty participation in this effort has been generous, with long-term commitments of time and effort. The IECD was developed as a comprehensive, integrated, Center-wide initiative to bring the intellectual and organizational resources of the Center to bear on the persistent problem of cancer disparities, and to heighten the awareness of these problems throughout the leadership structure. In this regard, the IECD is emerging as both a centralized research activity and a major resource of the Center. The ultimate goal is to contribute significantly to the elimination of racial, ethnic, and socioeconomic disparities in both prevention and treatment of cancer. This is still a work in progress—its success will only be measured in time by its effect on cancer disparities in the communities we serve. References Institute of Medicine. Unequal treatment: confronting racial and ethnic disparities in health care. Washington (DC): National Academic Press; 2003. 2. Institute of Medicine. Examining the health disparities research plan of the National Institutes of Health: unfinished business. Washington (DC): National Academies Press; 2006. 3. Zheng YL, Loffredo CA, Alberg AJ, et al. Less efficient g2-m checkpoint is associated with an increased risk of lung cancer in African Americans. Cancer Res 2005;65:9566 – 73. 4. Heist RS, Zhou W, Chirieac LR, et al. MDM2 polymorphism, survival, and histology in early-stage non-small-cell lung cancer. J Clin Oncol 2007;25:2243 – 7. 5. Liu G, Gurubhagavatula S, Zhou W, et al. Epidermal growth factor receptor polymorphisms and clinical outcomes in non-smallcell lung cancer patients treated with gefitinib. Pharmacogenomics J 2007. 6. Ray R, Jepson C, Wileyto P, et al. CREB1 haplotypes and the relative reinforcing value of nicotine. Mol Psychiatry 2007;12:615 – 7. 7. Lee AM, Jepson C, Hoffmann E, et al. CYP2B6 genotype alters abstinence rates in a bupropion smoking cessation trial. Biol Psychiatry 2007;62:635 – 41. 8. Munafo MR, Shields AE, Berrettini WH, Patterson F, Lerman C. Pharmacogenetics and nicotine addiction treatment. Pharmacogenomics 2005;6:211 – 23. 9. Mechanic LE, Bowman ED, Welsh JA, et al. Common genetic variation in TP53 is associated with lung cancer risk and prognosis in African Americans and somatic mutations in lung tumors. Cancer Epidemiol Biomarkers Prev 2007;16:214 – 22. 10. Neighbors CJ, Rogers ML, Shenassa ED, Sciamanna CN, Clark MA, Novak SP. Ethnic/racial disparities in hospital procedure volume for lung resection for lung cancer. Med Care 2007;45:655 – 63. 11. Mulligan CR, Meram AD, Proctor CD, Wu H, Zhu K, Marrogi AJ. Unlimited access to care: effect on racial disparity and prognostic factors in lung cancer. Cancer Epidemiol Biomarkers Prev 2006;15: 25 – 31. 12. Mervis J. Biomedical training programs. NIH told to get serious about giving minorities a hand. Science 2006;311:328 – 9. 1. Cancer Epidemiol Biomarkers Prev 2007;16(11). November 2007 Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2007 American Association for Cancer Research. Development of an Integrated Approach to Cancer Disparities: One Cancer Center's Experience Karen M. Emmons, Karen Burns White and Edward J. Benz Cancer Epidemiol Biomarkers Prev 2007;16:2186-2192. Updated version Cited articles Citing articles E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cebp.aacrjournals.org/content/16/11/2186 This article cites 9 articles, 5 of which you can access for free at: http://cebp.aacrjournals.org/content/16/11/2186.full.html#ref-list-1 This article has been cited by 1 HighWire-hosted articles. Access the articles at: /content/16/11/2186.full.html#related-urls Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cebp.aacrjournals.org on April 28, 2017. © 2007 American Association for Cancer Research.