Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
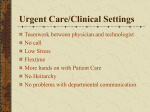
Pulse Pressure Amplification, Arterial Stiffness, and Peripheral Wave Reflection Determine Pulsatile Flow Waveform of the Femoral Artery Junichiro Hashimoto, Sadayoshi Ito Downloaded from http://hyper.ahajournals.org/ by guest on May 3, 2017 Abstract—Aortic stiffness, peripheral wave reflection, and aorta-to-peripheral pulse pressure amplification all predict cardiovascular risk. However, the pathophysiological mechanism behind it is unknown. Tonometric pressure waveforms were recorded on the radial, carotid, and femoral arteries in 138 hypertensive patients (age: 56⫾13 years) to estimate aorta-to-peripheral amplifications, aortic augmentation index, and aortic (carotid-femoral) pulse wave velocity. The femoral Doppler velocity waveform was recorded to calculate the reverse/forward flow index and diastolic/systolic forward flow ratio. The aorta-to-femoral and aorta-to-radial amplifications correlated inversely with the aortic augmentation index and pulse wave velocity. The femoral flow waveform was triphasic, composed of systolic forward, subsequent reverse, and diastolic forward phases in 129 patients, whereas it was biphasic and lacked a diastolic forward flow in 9 patients. Both the femoral reverse index (30⫾10%) and diastolic forward ratio (12⫾4%) correlated positively with the aorta-to-femoral amplification and inversely with the aortic augmentation index and pulse wave velocity; these correlations were independent of age, sex, diastolic pressure, and femoral artery diameter. Patients with biphasic (versus triphasic) flow were older, shorter, included more diabetics, had smaller femoral diameters, and showed greater aortic pulse wave velocity even when adjusted for all of these covariates. In conclusion, because of the inverse (peripheral-to-aortic) pressure gradient, pulse pressure amplification normally produces a substantial reversal of the femoral flow, the degree of which is determined by the aortic distensibility and peripheral wave reflection. Arteriosclerosis (increased stiffness, increased augmentation, and reduced amplification) decreases both the reverse and diastolic forward flows, potentially causing circulatory disturbance of truncal organs and lower extremities. (Hypertension. 2010;56:926-933.) Key Words: blood pressure 䡲 blood flow 䡲 arteriosclerosis 䡲 aorta 䡲 physiology 䡲 femoral 䡲 wave reflection T he arterial pulse provides important information on the cardiovascular prognosis. There is substantial evidence that the aortic pulse wave velocity (PWV) and augmentation index (AIx) predict cardiovascular morbidity and mortality in a variety of populations, as confirmed by recent meta-analysis studies.1,2 Similar prognostic significance has been also demonstrated for pulse pressure amplification from the central aorta to peripheral medium-sized muscular arteries.3–5 These pulse indices (PWV, AIx, and pulse amplification) depend on the structural and functional properties of the central elastic and peripheral muscular arteries, which interact closely through pressure wave transmission and reflection.6 –9 Potential mechanisms mediating these pulse abnormalities and cardiovascular disease progression include elevated central pressure leading to an increase in cardiac afterload10,11 and widened pulsatile pressure causing circumferential tensile stress that damages the vulnerable microvasculature in brain and kidney.12–14 It is not only blood pressure but also blood flow that is involved in target organ damage. Pulsatile flow produces tan- gential (frictional) shear stress on the arterial endothelium, whereas the mean flow contributes to tissue perfusion. Pulsatile flow stress may exert deleterious effects on the microvasculature synergistically with pulsatile pressure stress.12 The flow pulse waveforms of carotid15 and ophthalmic16 arteries have been shown to change with aging, indicating their association with arteriosclerosis. The femoral arteries, located between the body trunk and lower extremities, serve to supply blood flow inherently downstream. However, quite differently from the carotid and ophthalmic waveforms, the femoral flow waveform normally exhibits a triphasic pattern, including reverse (upstream) flow toward the central aorta.17–19 Previous investigations studied the reversal of femoral flow in association with cardiovascular risk factors and pharmacological intervention20 –22 and even postulated a potential connection with renal blood flow.23 Nevertheless, little attention has so far been paid to the fundamental, mechanical etiology of the generation of the flow reversal. Received July 14, 2010; first decision July 31, 2010; revision accepted August 30, 2010. From the Department of Blood Pressure Research (J.H., S.I.) and Division of Nephrology, Endocrinology, and Vascular Medicine (S.I.), Tohoku University Graduate School of Medicine, Sendai, Japan. Correspondence to Junichiro Hashimoto, Department of Blood Pressure Research, Tohoku University Graduate School of Medicine, 1-1 Seiryo-cho, Aoba-ku, Sendai 980-8574, Japan. E-mail [email protected] © 2010 American Heart Association, Inc. Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.110.159368 926 Hashimoto and Ito The pressure wave reflection responsible for aortic augmentation arises mainly from the lower body, particularly from the lower extremities.6 Central-to-peripheral (including aorta-to-leg) pulse amplification has been attributed to such peripheral wave reflection and gradual stiffening of arteries toward the periphery.9,24 However, another and possibly more important aspect of pulse amplification may be that it creates an inverse pressure gradient, namely from the periphery to the central aorta. We hypothesized in this study that pulse amplification would generate femoral reverse flow on account of the lower limb-to-aortic pressure gradient. To test this hypothesis, we examined hypertensive patients to evaluate the relationship between pressure pulse indices and the femoral flow waveform and its potential alteration with arteriosclerosis. Methods Downloaded from http://hyper.ahajournals.org/ by guest on May 3, 2017 An expanded Methods section is provided in the online Data Supplement (please see http://hyper.ahajournals.org). Subjects We studied 138 consecutive patients with hypertension, who were seen at the Division of Nephrology, Hypertension, and Endocrinology at Tohoku University Hospital. We excluded from the analysis patients with heart failure, peripheral artery disease, aortitis syndrome or aortic coarctation, thoracic or abdominal aortic aneurysm, sustained atrial fibrillation, and patients who had a history of acute coronary or stroke events within 6 months of the study. The study protocol had official approval from the institutional ethics committee of Tohoku University, and all of the subjects gave written informed consent. Laboratory Measurements Body height and weight were recorded for each subject to determine the body mass index. Details on laboratory measurements are provided in the online Data Supplement. Blood Pressure Measurements A series of vascular measurements were made in a quiet and temperature-controlled environment in accordance with consensus documentations.7 Patients rested in the supine position for 20 minutes, after which time blood pressure was measured twice over the brachial artery using a validated, automated cuff-oscillometric device (HEM-907, Omron Healthcare). Pressure Pulse Wave Analysis The radial artery pressure wave was recorded from the wrist with the applanation tonometry technique using a high-fidelity micromanometer (SPT-301, Millar Instruments). Details on pulse wave analysis are provided in the online Data Supplement. Briefly, the beat-to-beat pulse waveforms were ensemble averaged and calibrated using brachial systolic and diastolic pressures.5,9 The averaged radial waveform was then converted with a validated generalized transfer function (SphygmoCor version 8.2, AtCor Medical) to a corresponding central aortic waveform.6,25 Hence, aorta-to-radial pulse pressure amplification (AMPA-R) was determined as the percentage ratio of the radial pulse pressure (PPR) to the aortic pulse pressure (PPA)9,26: (1) AMPA-R⫽PPR⫼PPA⫻100 (%) The aortic augmented pressure and aortic AIx (standardized for a heart rate of 75 bpm) were also measured, as described previously.25,27 The round-trip travel time of the pressure wave from the heart to the major reflecting sites and back was estimated as the time from the beginning upstroke of the aortic pressure wave to the systolic upstroke of the reflected wave (inflection point).27 Pulse Pressure Amplification and Femoral Flow 927 Subsequently, the tonometric waveform was recorded in a similar manner on the common femoral artery. Additional recording was also made on the dorsalis pedis artery in a subset of subjects (n⫽101). Similar to the radial waveform, the femoral and dorsalis pedis waveforms were calibrated using brachial pressures, that is, by equating the mean and diastolic pressure levels of both aortic and peripheral signals.5,9 Thus, the pulse amplification ratios of the aorta-to-femoral and aorta-to-dorsalis pedis regions (AMPA-F and AMPA-DP) were obtained according to the following equations: (2) AMPA-F⫽PPF⫼PPA⫻100 (%) and (3) AMPA-DP⫽PPDP⫼PPA⫻100 (%) where PPF and PPDP represent the femoral pulse pressure and dorsalis pedis pulse pressure, respectively. The femoral AIx (adjusted for heart rate of 75 bpm) was determined in the same manner as the aortic AIx. Based on the sequential pressure wave recordings, the PWV was measured, as described previously.28 Specifically, the measurements were made centrally from the carotid to femoral artery for all of the subjects and, in addition, distally from the femoral to dorsalis pedis artery for a subset of subjects (n⫽101). The carotid-femoral PWV measures elastic artery stiffness, whereas the femoral-dorsal pedis PWV measures muscular artery stiffness.6 Detailed methods for the PWV measurements are provided in the online Data Supplement. Doppler Flow Measurements The femoral blood flow velocity measurement was made using duplex ultrasonography equipped with a 7.5-MHz linear transducer (Vivid i, GE Healthcare). Detailed methods for the Doppler flow recording are provided in the online Data Supplement. The diameter of the femoral artery was determined by B-mode imaging. Flow Pulse Wave Analysis The beat-to-beat femoral pulse flow waveforms were ensemble averaged for 10 consecutive pulses using the foot points of the systolic upstrokes for synchronization (please see the online Data Supplement for details). From the averaged waveform, we determined the following parameters in terms of flow velocity and relevant time (Figure 1): systolic forward (maximum) peak velocity (VF); reverse (minimum) peak velocity (VR); end-diastolic velocity (VD); time-averaged mean velocity (VM); acceleration time (TACL); and deceleration time (TDCL). In most cases, the diastolic forward flow followed the reverse flow, so its peak velocity (VF2) was also measured whenever available. Then, we calculated the following parameters as relative ratios: (1) reverse-to-forward flow ratio ⫽ 兩VR兩⫼兩VF兩⫻100 (%); (2) reverse-to-forward flow index⫽兩VR⫺ VD兩⫼兩VF⫺VD兩⫻100 (%); and (3) diastolic-to-systolic forward flow ratio⫽兩VF2兩⫼兩VF兩⫻100 (%). Femoral flow volume (in milliliters per minute) was also calculated from the time-averaged mean flow velocity and the femoral artery diameter. Femoral vascular resistance (in millimeters of mercury per milliliter per minute) was obtained by dividing the mean arterial pressure by the flow volume. Statistical Analysis Data analyses were performed with SPSS software (version 13.0). Univariate comparisons were made using Student t test, ANOVA with a post hoc Bonferroni test, paired t test, or 2 test, as appropriate (please see the online Data Supplement for more details). Univariate correlations were evaluated as Pearson correlation coefficients (r). Multivariate linear regression analysis was performed to investigate independent correlates of the femoral reverse-flow index and diastolic forward-flow ratio. Multivariate comparisons of pulse wave parameters between patients with triphasic and biphasic flow were made using ANCOVA. Data are provided as mean⫾SD or percentages. All of the reported P values are 2 sided, and a P value of ⬍0.05 was considered statistically significant. 928 Hypertension Flo ow velo ocity (cm m/s) 120 November 2010 Table 1. VF Characteristics of Subjects (nⴝ138) Variable 80 Age, y VF2 40 Women, n (%) VM Height, cm Weight, kg 0 -40 40 Total Clinical measures TACL 0 VD VR TDCL 0 25 0.25 05 0.5 0 75 0.75 Time (s) Downloaded from http://hyper.ahajournals.org/ by guest on May 3, 2017 Figure 1. Definition of flow and time parameters derived from the ensemble-averaged femoral velocity waveform. VF indicates systolic forward peak velocity; VR, reverse peak velocity; VF2, diastolic forward peak velocity; VM, time-averaged mean velocity; VD, end-diastolic velocity; TACL, acceleration time; TDCL, deceleration time. Reverse/forward flow ratio (RFR), reverse/ forward flow index (RFI), and diastolic/systolic forward flow ratio (DFR) were calculated as follows: RFR⫽兩VR兩⫼兩VF兩⫻100 (%); RFI⫽兩VR⫺VD兩⫼兩VF⫺VD兩⫻100 (%); DFR⫽兩VF2兩⫼兩VF兩⫻100 (%). Results Subject Characteristics Baseline characteristics of the study subjects are presented in Table 1. The subjects included 52 men and 86 women, with a mean age of 56⫾13 years (range: 20 to 88 years). Mean brachial systolic/diastolic pressure was 125/69 mm Hg, and most of the subjects had their blood pressure controlled well with antihypertensive treatment. Some subjects had hypercholesterolemia (31.9%) and diabetes mellitus (29.7%). 56⫾13 86 (62) 160⫾9 64⫾14 Body mass index, kg/m2 24.8⫾4.1 Total cholesterol, mg/dL 183⫾44 High-density lipoprotein cholesterol, mg/dL 52⫾15 Low-density lipoprotein cholesterol, mg/dL 105⫾36 Fasting blood glucose, mg/dL 106⫾35 Hemoglobin A1c, % 5.7⫾1.1 Hypercholesterolemia, n (%) 44 (32) Diabetes mellitus, n (%) 41 (30) Pressure measures Brachial systolic blood pressure, mm Hg 125⫾18 Brachial diastolic blood pressure, mm Hg 69⫾10 Mean arterial pressure, mm Hg 88⫾12 Heart rate, bpm 65⫾9 Aortic systolic blood pressure, mm Hg 113⫾17 Aortic augmented pressure, mm Hg 12⫾7 Aortic AIx, %* 20⫾10 Round-trip travel time (TR), ms 138⫾9 Femoral AIx, %* ⫺9⫾14 Pulse amplification, % Aorta-to-radial (AMPA-R) 132⫾16 Aorta-to-femoral (AMPA-F) 128⫾15 Aorta-to-dorsalis pedis (AMPA-DP)† 179⫾31 PWV, m/s Pressure Pulse Parameters Pulse pressure amplifications of aorta-to-femoral, aorta-todorsalis pedis, and aorta-to-radial regions were all ⬎100% for every subject (Table 1). The amplification was greatest for the aorta-to-dorsalis pedis region, followed by the aorta-toradial and, then, aorta-to-femoral regions (Pⱕ0.001). The 3 amplifications had moderate-to-close inverse correlations with the aortic AIx standardized for the heart rate (aorta-tofemoral: r⫽⫺0.37; aorta-to-dorsalis pedis: r⫽⫺0.52; aortato-radial: r⫽⫺0.83; P⬍0.001 for all) and relatively mild inverse correlations with the aortic (ie, carotid-femoral) PWV (aorta-to-femoral: r⫽⫺0.25, P⫽0.004; aorta-to-dorsalis pedis: r⫽⫺0.31, P⫽0.002; aorta-to-radial: r⫽⫺0.22; P⫽0.01). The peripheral (ie, femoral-dorsalis pedis) PWV had no significant correlations with the pulse amplifications. Carotid-femoral (PWVC-F) 7.9⫾2.1 Femoral-dorsalis pedis (PWVF-DP)† 9.0⫾1.5 Femoral flow measures Femoral artery diameter, mm Systolic forward peak flow velocity (VF), cm/s Reverse peak flow velocity (VR), cm/s 7.9⫾1.1 69⫾19 ⫺19⫾6 Diastolic forward peak flow velocity (VF2), cm/s 8⫾4 End-diastolic flow velocity (VD), cm/s 1⫾3 Time-averaged mean flow velocity (VM), cm/s 12⫾5 Flow pulse amplitude (VF⫺VR), cm/s 88⫾22 Reverse/forward flow ratio (VR/VF), % 28⫾10 Reverse/forward flow index (VR⫺VD/VF⫺VD), % 30⫾10 Diastolic/systolic forward flow ratio (VF2/VF), % Flow acceleration time (TACL), ms 12⫾4 106⫾17 Femoral Flow Waveform Flow deceleration time (TDCL), ms 200⫾30 Of the 138 subjects, 129 (93.5%) had a triphasic femoral flow velocity waveform, which was composed of the initial forward (positive) phase that flows in systole toward the peripheral leg arteries, the secondary reverse (negative) phase that flows backward to the central aorta, and the tertiary forward phase that flows in diastole toward the periphery (Figure 1 and Figure S1A, available in the online Data Supplement). The remaining 9 subjects (6.5%) had a biphasic Femoral vascular resistance, mm Hg/mL per min 0.33⫾0.22 *Data were standardized for heart rate of 75 bpm. †Data were available in 101 subjects. velocity waveform lacking a definite diastolic forward flow (Figure S1B). There were no patients showing a monophasic flow pattern suggestive of stenotic or occlusive arterial lesions. Hashimoto and Ito AMPA–F Femo oral revers se/forwarrd flow ind dex (%) 30 AMPA–DP (%) r = 0.35 P < 0.001 Pulse Pressure Amplification and Femoral Flow AMPA–R (%) r = 0.35 P < 0.001 929 (%) r = 0.22 P = 0.009 20 10 0 50 100 150 AIxA 30 200 50 100 150 200 250 300 PWVC–F (%) r = −0.29 P < 0.001 50 100 150 200 PWVF–DP (m/s) (m/s) r = −0.19 P = 0.02 r = 0.11 P = 0.29 20 Figure 2. Relationships between pressure wave parameters and femoral reverse/forward flow index. AMPA-F indicates aorta-to-femoral pulse pressure amplification; AMPA-DP, aorta-to-dorsalis pedis pulse pressure amplification; AMPA-R, aorta-to-radial pulse pressure amplification; AIxA, aortic AIx (standardized for heart rate of 75 bpm); PWVC-F, carotid-femoral PWV; PWVF-DP, femoraldorsalis pedis PWV. 10 Downloaded from http://hyper.ahajournals.org/ by guest on May 3, 2017 0 -20 0 20 40 60 0 5 10 15 20 0 The femoral flow velocity increased rapidly in early systole to reach the systolic peak (VF), with a mean acceleration time of 106 ms (Table 1 and Figure 1). Subsequently, it gradually decreased to reach the minimum reverse peak (VR) with a deceleration time of 200 ms; the deceleration time was longer than the acceleration time (P⬍0.001). The amplitude of the reverse flow velocity (兩VR兩) was always smaller than that of the systolic forward velocity (兩VF兩; P⬍0.001) and greater than that of the diastolic forward velocity (兩VF2兩; P⬍0.001). The end-diastolic flow velocity (VD) ranged across 0 between positive (9.5 m/s) and negative (⫺7.9 m/s) values among the subjects, whereas the time-averaged mean velocity (VM) was invariably positive (range: 3.2 to 24.3 m/s). The mean reverse-to-forward flow ratio (兩VR兩/兩VF兩), reverse-toforward flow index (兩VR⫺VD兩/兩VF⫺VD兩), and diastolic-to-systolic forward flow ratio (兩VF2兩/兩VF兩) were 28.1%, 29.5%, and 12.0%, respectively (Table 1). Determinants of Femoral Reverse Flow Figure 2 shows the relationships between the femoral reverseto-forward flow index and various pressure pulse parameters. The reverse flow index was significantly and positively correlated with each of the 3 pulse pressure amplifications; the correlation was stronger with the aorta-to-femoral and aorta-to-dorsalis pedis amplifications than with the aorta-toradial amplification. Significant inverse correlations were also found with aortic PWV and AIx, despite the lack of a correlation with the peripheral PWV (Figure 2). The femoral reverse-flow index was correlated also with femoral AIx (r⫽⫺0.30; P⬍0.001). There was only a marginal correlation between the femoral reverse flow index and the femoral vascular resistance (r⫽0.16; P⫽0.06). Subject characteristics were evaluated separately for the tertile groups divided according to femoral reverse flow index (Table S1). When compared with the lowest tertile, the highest tertile of the reverse flow index included more men who were taller of stature and had higher diastolic blood 5 10 15 20 pressure and greater femoral artery diameters. Also, the pulse amplifications were significantly greater and the aortic AIx and PWV were lower in the highest reverse-flow tertile. There were no differences in age, body mass index, biochemical parameters, prevalence of hypercholesterolemia or diabetes mellitus, brachial or aortic systolic pressure, or heart rate among the 3 tertiles of the reverse-flow index. Multivariate regression analysis revealed that the significant independent predictors of the femoral reverse-flow index were the aorta-to-femoral pulse amplification, carotidfemoral PWV, and diastolic blood pressure (Table 2). Age, sex, height, and femoral artery diameter were not signifiTable 2. Significant Independent Predictors of Femoral Reverse/Forward-Flow Index and Diastolic/Systolic Forward-Flow Ratio Variable Regression Coefficient⫾SE  P Model for reverse/forward-flow index (R 2⫽0.30; P⬍0.001)* Aorta-to-femoral pulse amplification, % Diastolic blood pressure, mm Hg 0.18⫾0.05 0.28 0.001 0.26⫾0.08 0.28 0.001 ⫺1.32⫾0.47 ⫺0.28 0.006 Carotid-femoral PWV, m/s ⫺0.65⫾0.21 ⫺0.26 0.002 Age, y ⫺0.11⫾0.03 ⫺0.28 0.002 Carotid-femoral PWV, m/s Model for diastolic/systolic forward-flow ratio (R 2⫽0.51; P⬍0.001)* Aorta-to-femoral pulse amplification, % Diastolic blood pressure, mm Hg Diabetes mellitus (yes⫽1, no⫽0) 0.06⫾0.02 0.08⫾0.04 ⫺1.59⫾0.80 0.17 0.02 0.15 0.03 ⫺0.14 0.049  indicates the standardized regression coefficient. *Variables included in the multiple linear regression models were age, sex, height, hypercholesterolemia, diabetes mellitus, diastolic blood pressure, aorta-to-femoral pulse amplification, carotid-femoral PWV, and femoral artery diameter. Only significant predictors were listed. Hypertension Femorral diastoliic/systolic forward flo ow ratio (% %) 930 25 November 2010 AMPA–F AMPA–DP AMPA–R AIxA PWVC–F PWVF–DP P < 0.001 P < 0.001 P = 0.001 P < 0.001 P < 0.001 P = 0.71 20 * * * * * * * 15 * * * 10 5 0 Downloaded from http://hyper.ahajournals.org/ by guest on May 3, 2017 (%) (%) (%) (%) (m/s) (m/s) Figure 3. Femoral diastolic/systolic forward-flow ratio in quartile groups classified by various pressure wave parameters. Abbreviations are the same as in Figure 2. P values are evaluated by ANOVA. *P⬍0.05 vs the lowest quartile (Bonferroni test). cantly associated. When substituted for the aorta-to-femoral amplification in this model, the aortic or femoral AIx was able to independently predict reverse flow index (aortic AIx: ⫽⫺0.26, P⫽0.02; femoral AIx: ⫽⫺0.31, P⫽0.002), but aorta-to-radial amplification was only marginally able to do so (⫽⫺0.17; P⫽0.06). Replacement of the diastolic blood pressure by the femoral vascular resistance or the mean arterial pressure did not meaningfully alter any of the results (Table S2). Similar but weaker associations were observed when the reverse-flow ratio instead of the index was used as a dependent variable (data not shown). Determinants of Femoral Diastolic Forward Flow Figure 3 shows comparisons of the femoral diastolic-to-systolic forward-flow ratio among the quartile groups divided according to each of 6 pressure pulse parameters. The diastolic forward-flow ratio increased in a dose-dependent manner with increasing quartiles of the aorta-to-femoral, as well as aorta-to-dorsalis pedis and aorta-to-radial, pulse amplifications. There was a significant decrease in the diastolic forward-flow ratio with increasing aortic PWV and AIx quartiles, although there was no difference among the peripheral PWV quartiles. A similar decrease was seen with increasing femoral AIx quartiles (P⬍0.001). A close correlation was observed between the diastolic forward-flow ratio and reverse-flow index (r⫽0.52; P⬍0.001). As shown in Table S3, division of the subjects into tertiles according to diastolic forward-flow ratio suggested that higher diastolic forward flow was associated with younger age, male sex, taller stature, lower prevalence of diabetes mellitus and hypercholesterolemia, lower blood pressure, and larger femoral artery diameter. There was no association between the diastolic forward-flow ratio and femoral vascular resistance. In a multivariate model considering these relevant factors, diastolic forward-flow ratio was predicted significantly and independently by carotid-femoral PWV, as well as by age, diastolic blood pressure, diabetes mellitus and aorta-tofemoral amplification (Table 2). On replacement of the aorta-to-femoral amplification, the aortic AIx was also capable of independently predicting the diastolic forward-flow ratio (⫽⫺0.20; P⫽0.02). Femoral vascular resistance was not an independent predictor of the diastolic forward-flow ratio (Table S2). Determinants of Flow Acceleration Time The acceleration time of the systolic forward flow correlated inversely with age (r⫽⫺0.17; P⫽0.04), systolic pressure (r⫽⫺0.26; P⫽0.002), mean arterial pressure (r⫽⫺0.19; P⫽0.02), aortic PWV (r⫽⫺0.17; P⫽⫺0.04), and peripheral PWV (r⫽⫺0.33; P⫽0.001) and correlated positively with the round-trip travel time of the pressure wave (r⫽0.34; P⬍0.001). Even after adjustment for age and systolic pressure, peripheral PWV and round-trip travel time were significantly related to the flow acceleration time (⫽⫺0.24, P⫽0.02 and ⫽0.29, P⫽0.004), whereas the aortic PWV was not. Subject Characteristics of Biphasic Versus Triphasic Femoral Flow When compared with subjects with a typical triphasic flow waveform, those with a biphasic waveform lacking diastolic forward flow were significantly older of age, shorter of stature, and more frequently female and diabetic and had lower diastolic blood pressure and smaller femoral artery diameter (Table S4). They also showed smaller pulse amplifications, greater aortic AIx, and higher carotid-femoral but similar femoral-dorsalis pedis PWVs. The patients with a biphasic flow pattern had a reverse stiffness gradient, that is, the aortic PWV tended to be greater than the peripheral PWV. After adjusting for age, sex, height, diabetes mellitus, diastolic blood pressure, and femoral artery diameter by ANCOVA, Hashimoto and Ito the significance of differences in pulse amplifications and aortic AIx disappeared, but the difference in carotid-femoral PWV persisted with high significance (P⫽0.005) between the subjects with triphasic flow (adjusted mean PWV: 7.8 m/s [95% CI: 7.5 to 8.0 m/s]) and those with biphasic flow (adjusted mean PWV: 9.5 m/s [95% CI: 8.3 to 10.6 m/s]). Discussion Downloaded from http://hyper.ahajournals.org/ by guest on May 3, 2017 The existence of significant reverse flow in the femoral arteries has long been recognized, although questions remain concerning the source of the flow reversal. The present study investigated the femoral velocimetric flow with respect to the pulsatile pressure differences between various arterial sites using time-domain analysis and, to our knowledge, for the first time found that the central-to-peripheral pulse pressure amplification determines the degree of flow reversal. Because pulse amplification means, by definition, higher systolic and pulse pressures in peripheral (eg, femoral and dorsalis pedis) arteries than in the central aorta,9 it naturally generates an inverse (peripheral-to-central) pressure gradient during late systole and early diastole, which follows a forward (centralto-peripheral) pressure gradient because of cardiac ejection in early systole. Our results indicate that this inverse pressure gradient is responsible for the femoral reverse flow. This interpretation agrees with the physiological principle that the pressure gradient along the artery, rather than the pressure itself, determines pulsatile flow.6 Such a view is also supported by the present finding that the lower-body (ie, aortato-femoral and aorta-to-dorsalis pedis) amplifications were more closely correlated with the femoral reverse flow than the upper-body (aorta-to-radial) amplification (Figure 2), suggesting an important role of the local pressure gradient at the femoral site in determining the reverse flow. Our results indicating the contribution of the pulse amplification to the femoral reverse flow accord well with the observations of previous relevant studies. For instance, both pulse amplification29 and femoral reverse flow18,20,22 have been shown to increase in response to treatment with nitrate vasodilators. Both are decreased by cigarette smoking21,30 and with aging.17,31 All of these parallel changes are probably explicable by direct causality between them. The present study showed that the aortic AIx and carotidfemoral PWV were correlated inversely with the femoral reverse-flow index (Figure 2). It is well recognized that peripheral wave reflection–induced aortic pressure augmentation reduces the pulse amplification.24,32,33 Considering this together with the close inverse relationship between the aortic AIx and pulse amplification observed in the present study, the influence of the pressure wave reflection on the femoral reverse flow may be largely through pulse amplification. It is important to note that a lower rather than higher AIx was associated with greater femoral reverse flow (Figure 2 and Table S1), because this finding indicates that it is not the magnitude of the reflected pressure wave itself but rather the pressure gradient generated by the summation of the incident and reflected waves that causes the flow reversal. In contrast, the influence of aortic stiffness on the femoral reverse flow appears to be, at least in part, independent of the pulse amplification (Table 2), although it is attributable in part to Pulse Pressure Amplification and Femoral Flow 931 the “nonaugmented” incident wave amplification.24,33 This indicates that the amount of the femoral reverse flow is determined not only by the pressure gradient but also by the distensibility of upstream arteries that can passively receive the reversed flow. The important relevance of arterial distensibility to pulsatile flow is consistent with Bramwell and Hill’s equation34 showing that the blood volume change depends on the PWV, as well as on the blood pressure change. The femoral diastolic forward flow had essentially the same determinants as the reverse flow, including pulse amplification, aortic stiffness, and peripheral wave reflection (Figure 3 and Table 2). Also, a close correlation was observed between the two. These results may suggest that the femoral diastolic forward flow originates at least in part from the reverse flow; in other words, blood first accumulates in the distensible aorta during late systole and early diastole on account of the reverse (upstream) flow, and then the blood flows out of the aorta during middiastole on account of the aortic elasticity (Windkessel function). Such a transition from reverse to forward flow could also result from secondary reflection (rereflection) of the reflected pressure waves.6 Because the femoral reverse flow is usually greater than the diastolic forward flow (Table 1), it seems reasonable to assume that some reverse flow becomes antegrade flow into internal organs of the body trunk,23 the rest going into the lower extremities. Interestingly, the acceleration time of the femoral flow was found to depend on the peripheral (rather than central) PWV and on the round-trip travel time of the pressure wave. One may speculate from this finding that the transition from flow acceleration to deceleration relates to the time of the pressure wave to travel from the femoral artery to distal (downstream) reflecting sites and back.35 In the present study, a small but significant number of subjects (6.5%) had a biphasic femoral flow waveform (Figure S1B). Although this flow pattern clearly differs from the monophasic pattern suggestive of stenotic or occlusive arterial lesions, it appears not to be an independent entity distinct from the typical triphasic pattern but rather to represent its extreme of reduced diastolic forward flow. The biphasic flow pattern related to an increased aortic PWV even after adjustment of various relevant factors (Table S4), indicating that aortic stiffening (arteriosclerosis) can markedly reduce diastolic flow into lower extremities owing solely to an impaired Windkessel function, even without accompanying peripheral artery stenosis.36 This study has several strengths in terms of methodology. The pulsatile flow was recorded as the instantaneous, spatially averaged mean velocity at a constant interval of 100 Hz continuously over 16 seconds, and steady-state flow waveforms of as many as 10 pulse beats were ensemble averaged using a dedicated program. Such automatic recording of the pulse waveform and quantitative evaluation of the flow parameters enabled us to minimize potential observer and data selection biases. Estimation of the pulse amplification was made from the pulse waveforms alone and, therefore, was free from any influence of the cuff pressure measurement that might be more prone to error.2,25,26 Calculation of the 932 Hypertension November 2010 Downloaded from http://hyper.ahajournals.org/ by guest on May 3, 2017 reverse flow index (rather than the ratio) enabled us to eliminate any potential interference on the pulsatile flow of the steady flow (ie, end-diastolic flow) that could be modulated by peripheral vascular resistance.18,37 In fact, the present data confirmed that the relevance of pulse pressure amplification and arterial stiffness to the femoral reverse flow is independent of the femoral vascular resistance (Table S2). This study has some limitations. Blood flow was quantified as velocity rather than volume, because it is quite difficult with commonly available ultrasonographs to measure minute instantaneous changes of the arterial diameter simultaneously with the flow velocity. However, it should be noted that this study focused not on the absolute values of, but on the relative ratio between, the pulsatile flow components, on which the influence of arterial diameter seems to be negligibly small. Another limitation is the cross-sectional, observational nature of this study. The suggested causal relationship between pressure and flow needs be confirmed further by prospective interventional studies. Perspectives Our data demonstrated substantial reverse flow from lower extremities toward the abdominal aorta in hypertensive subjects and its reduction attributed to aortic stiffening. Of interest, previous data by Bogren and Buonocore23 suggest that reverse flow in the lower body supplies diastolic flow to internal abdominal organs, such as the kidneys, and it importantly contributes to visceral perfusion. Taken together, it seems likely that the reduction in femoral reverse flow resulting from aortic stiffening causes visceral diastolic hypoperfusion leading to target organ failure (Figure 2). On the other hand, aortic stiffening could predispose to peripheral artery disease in consequence of reduced diastolic flow into lower extremities (Figure 3).36 Our study suggests that normalization of the pulse amplification and/or aortic stiffness by pharmacological treatment could help to restore blood flow into internal organs, as well as lower extremities. Verification of this possibility requires future studies. Acknowledgment We are grateful to Dr Berend E. Westerhof, BMEYE (Amsterdam, the Netherlands) for programming software dedicated to flow waveform analysis. Sources of Funding This work was supported by a grant from Tohoku University Hospital. Disclosures None. References 1. Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;55:1318 –1327. 2. Vlachopoulos C, Aznaouridis K, O’Rourke MF, Safar ME, Baou K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with central haemodynamics: a systematic review and meta-analysis. Eur Heart J. 2010;31:1865–1871. 3. Safar ME, Blacher J, Pannier B, Guerin AP, Marchais SJ, Guyonvarc’h PM, London GM. Central pulse pressure and mortality in end-stage renal disease. Hypertension. 2002;39:735–738. 4. Williams B, Lacy PS, Thom SM, Cruickshank K, Stanton A, Collier D, Hughes AD, Thurston H, O’Rourke M. Differential impact of blood pressure-lowering drugs on central aortic pressure and clinical outcomes: principal results of the Conduit Artery Function Evaluation (CAFE) Study. Circulation. 2006;113:1213–1225. 5. Benetos A, Thomas F, Joly L, Blacher J, Pannier B, Labat C, Salvi P, Smulyan H, Safar ME. Pulse pressure amplification a mechanical biomarker of cardiovascular risk. J Am Coll Cardiol. 2010;55:1032–1037. 6. Nichols WW, O’Rourke MF. McDonald’s Blood Flow in Arteries: Theoretical, Experimental and Clinical Principles. London, United Kingdom: Hodder Arnold; 2005. 7. Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27:2588 –2605. 8. Agabiti-Rosei E, Mancia G, O’Rourke MF, Roman MJ, Safar ME, Smulyan H, Wang JG, Wilkinson IB, Williams B, Vlachopoulos C. Central blood pressure measurements and antihypertensive therapy: a consensus document. Hypertension. 2007;50:154 –160. 9. Avolio AP, Van Bortel LM, Boutouyrie P, Cockcroft JR, McEniery CM, Protogerou AD, Roman MJ, Safar ME, Segers P, Smulyan H. Role of pulse pressure amplification in arterial hypertension: experts’ opinion and review of the data. Hypertension. 2009;54:375–383. 10. Hashimoto J, Nichols WW, O’Rourke MF, Imai Y. Association between wasted pressure effort and left ventricular hypertrophy in hypertension: influence of arterial wave reflection. Am J Hypertens. 2008;21:329 –333. 11. Roman MJ, Okin PM, Kizer JR, Lee ET, Howard BV, Devereux RB. Relations of central and brachial blood pressure to left ventricular hypertrophy and geometry: the Strong Heart Study. J Hypertens. 2010;28: 384 –388. 12. O’Rourke MF, Hashimoto J. Mechanical factors in arterial aging: a clinical perspective. J Am Coll Cardiol. 2007;50:1–13. 13. Safar ME. Peripheral pulse pressure, large arteries, and microvessels. Hypertension. 2004;44:121–122. 14. Temmar M, Jankowski P, Peltier M, Mouquet V, Debicka-Dabrowska D, Hamida F, Kawecka-Jaszcz K, Safar ME. Intraaortic pulse pressure amplification in subjects at high coronary risk. Hypertension. 2010;55: 327–332. 15. Hirata K, Yaginuma T, O’Rourke MF, Kawakami M. Age-related changes in carotid artery flow and pressure pulses: possible implications for cerebral microvascular disease. Stroke. 2006;37:2552–2556. 16. Michelson G, Harazny J, Schmieder RE, Berendes R, Fiermann T, Warntges S. Fourier analysis of the envelope of the ophthalmic artery blood flow velocity: age- and blood pressure related impact. Hypertension. 2007;50: 964–969. 17. Nimura Y, Matsuo H, Hayashi T, Kitabatake A, Mochizuki S. Studies on arterial flow patients - instantaneous velocity spectrums and their phasic changes - with directional ultrasonic Doppler technique. Br Heart J. 1974;36:899 –907. 18. Labs KH, Labs R. Drug-induced changes of the flow pulse contour recorded by directional CW-Doppler devices: a possible estimation of changes in vascular characteristic impedance and peripheral resistance. Methods Find Exp Clin Pharmacol. 1985;7:603– 608. 19. Holland CK, Brown JM, Scoutt LM, Taylor KJ. Lower extremity volumetric arterial blood flow in normal subjects. Ultrasound Med Biol. 1998;24:1079 –1086. 20. Mahler F, Brunner HH, Bollinger A, Casty M, Anliker M. Changes in phasic femoral artery flow induced by various stimuli: a study with percutaneous pulsed Doppler ultrasound. Cardiovasc Res. 1977;11: 254 –260. 21. Caro CG, Lever MJ, Parker KH, Fish PJ. Effect of cigarette smoking on the pattern of arterial blood flow: possible insight into mechanisms underlying the development of arteriosclerosis. Lancet. 1987;2:11–13. 22. Caro CG, Fish PJ, Goss DE, Halls J, Lever MJ, Parker KH, Clear AS. Effects of isosorbide dinitrate on the pattern of arterial blood flow in healthy human subjects. Clin Sci (Lond). 1990;79:215–220. 23. Bogren HG, Buonocore MH. Blood flow measurements in the aorta and major arteries with MR velocity mapping. J Magn Reson Imaging. 1994; 4:119 –130. 24. Wilkinson IB, Franklin SS, Hall IR, Tyrrell S, Cockcroft JR. Pressure amplification explains why pulse pressure is unrelated to risk in young subjects. Hypertension. 2001;38:1461–1466. 25. Hashimoto J, Imai Y, O’Rourke MF. Indices of pulse wave analysis are better predictors of left ventricular mass reduction than cuff pressure. Am J Hypertens. 2007;20:378 –384. Hashimoto and Ito 26. Hashimoto J, Imai Y, O’Rourke MF. Monitoring of antihypertensive therapy for reduction in left ventricular mass. Am J Hypertens. 2007;20: 1229 –1233. 27. Hashimoto J, Westerhof BE, Westerhof N, Imai Y, O’Rourke MF. Different role of wave reflection magnitude and timing on left ventricular mass reduction during antihypertensive treatment. J Hypertens. 2008;26: 1017–1024. 28. Wilkinson IB, Fuchs SA, Jansen IM, Spratt JC, Murray GD, Cockcroft JR, Webb DJ. Reproducibility of pulse wave velocity and augmentation index measured by pulse wave analysis. J Hypertens. 1998;16: 2079 –2084. 29. Kelly RP, Gibbs HH, O’Rourke MF, Daley JE, Mang K, Morgan JJ, Avolio AP. Nitroglycerin has more favourable effects on left ventricular afterload than apparent from measurement of pressure in a peripheral artery. Eur Heart J. 1990;11:138 –144. 30. Mahmud A, Feely J. Effect of smoking on arterial stiffness and pulse pressure amplification. Hypertension. 2003;41:183–187. 31. McEniery CM, Yasmin, McDonnell B, Munnery M, Wallace SM, Rowe CV, Cockcroft JR, Wilkinson IB. Central pressure: variability and impact Pulse Pressure Amplification and Femoral Flow 32. 33. 34. 35. 36. 37. 933 of cardiovascular risk factors: the Anglo-Cardiff Collaborative Trial II. Hypertension. 2008;51:1476 –1482. Segers P, Mahieu D, Kips J, Rietzschel E, De Buyzere M, De Bacquer D, Bekaert S, De Backer G, Gillebert T, Verdonck P, Van Bortel L. Amplification of the pressure pulse in the upper limb in healthy, middle-aged men and women. Hypertension. 2009;54:414 – 420. Hashimoto J, Ito S. Some mechanical aspects of arterial aging: physiological overview based on pulse wave analysis. Ther Adv Cardiovasc Dis. 2009;3:367–378. Bramwell JC, Hill AV. Velocity of transmission of the pulse wave. Lancet. 1922:891– 892. Jones CJ, Singer DR, Watkins NV, MacGregor GA, Caro CG. Abnormal arterial flow pattern in untreated essential hypertension: possible link with the development of atherosclerosis. Clin Sci (Lond). 1990;78:431– 435. Suzuki E, Kashiwagi A, Nishio Y, Egawa K, Shimizu S, Maegawa H, Haneda M, Yasuda H, Morikawa S, Inubushi T, Kikkawa R. Increased arterial wall stiffness limits flow volume in the lower extremities in type 2 diabetic patients. Diabetes Care. 2001;24:2107–2114. Holenstein R, Ku DN. Reverse flow in the major infrarenal vessels: a capacitive phenomenon. Biorheology. 1988;25:835– 842. Downloaded from http://hyper.ahajournals.org/ by guest on May 3, 2017 Pulse Pressure Amplification, Arterial Stiffness, and Peripheral Wave Reflection Determine Pulsatile Flow Waveform of the Femoral Artery Junichiro Hashimoto and Sadayoshi Ito Downloaded from http://hyper.ahajournals.org/ by guest on May 3, 2017 Hypertension. 2010;56:926-933; originally published online September 27, 2010; doi: 10.1161/HYPERTENSIONAHA.110.159368 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2010 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/56/5/926 Data Supplement (unedited) at: http://hyper.ahajournals.org/content/suppl/2010/09/29/HYPERTENSIONAHA.110.159368.DC1 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/ ONLINE SUPPLEMENT Pulse Pressure Amplification, Arterial Stiffness, and Peripheral Wave Reflection Determine Pulsatile Flow Waveform of the Femoral Artery Authors: Junichiro Hashimoto, MD, PhD,1 and Sadayoshi Ito, MD, PhD1,2 1 Department of Blood Pressure Research, and 2Division of Nephrology, Endocrinology, and Vascular Medicine, Tohoku University Graduate School of Medicine, Sendai, Japan Short title: Pulse Pressure Amplification and Femoral Flow Address for correspondence: Junichiro Hashimoto, MD, PhD Associate Professor Department of Blood Pressure Research Tohoku University Graduate School of Medicine 1-1 Seiryo-cho, Aoba-ku, Sendai 980-8574, Japan Tel: +81-22-717-7163; Fax: +81-22-717-7168 E-mail: [email protected] 1 Expanded Methods Subjects We studied 138 consecutive patients with hypertension, who were seen at the Division of Nephrology, Hypertension, and Endocrinology, Tohoku University Hospital. We excluded from the analysis patients with heart failure (left ventricular ejection fraction <40 % or documented), peripheral artery disease (ankle-brachial pressure index < 0.9 or documented), aortitis syndrome or aortic coarctation, thoracic or abdominal aortic aneurysm, sustained atrial fibrillation, and patients who had a history of acute coronary or stroke events within 6 months of the study. The study protocol had official approval from the institutional ethics committee of Tohoku University, and all subjects gave written informed consent. Laboratory measurements Body height and weight were recorded for each subject to determine the body mass index. Venous blood samples were drawn to measure total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, fasting blood glucose and hemoglobin A1c by standard methods. Diabetes mellitus was defined as a fasting glucose concentration ≥ 126 mg/dl or undergoing anti-diabetic drug treatment, and hypercholesterolemia as a total cholesterol ≥ 240 mg/dl or undergoing treatment with a cholesterol-lowering drug. Blood pressure measurements A series of vascular measurements were made in a quiet and temperature-controlled environment in accordance with consensus documentations.1 Patients were rested in the supine position for 20 minutes, after which time blood pressure was measured over the brachial artery using a validated, automated cuff-oscillometric device (HEM-907, Omron Health Care, Kyoto, Japan). The measurement was repeated twice at an interval of 3 minutes, and the average of two measurements was used as representative of the brachial blood pressure. Pressure pulse wave analysis The radial artery pressure wave was recorded from the wrist with the applanation tonometry technique using a high fidelity micromanometer (SPT-301, Millar Instruments, Houston, TX). The pressure signals were sampled at a rate of 256 Hz for 11 seconds, and the beat-to-beat pulse waveforms were ensemble-averaged. Brachial 2 systolic and diastolic pressures were used to calibrate the radial pressure waveform, and the mean arterial pressure was derived by integration of the radial waveform. The heart rate was determined from the waveform using the cardiac cycle length. The averaged radial waveform was then converted with a validated generalized transfer function (SphygmoCor version 8.2, AtCor Medical, Sydney, Australia) to a corresponding central aortic waveform.2,3 Hence, aorta-to-radial pulse pressure amplification (AMPA-R) was determined as the percent ratio of the radial pulse pressure (PPR) to the aortic pulse pressure (PPA):4,5 AMPA-R = PPR ÷ PPA × 100 (%). Of note, the amplification ratio can be determined from the pulse wave shapes alone without any calibration to absolute blood pressure values, since the mean arterial pressure and diastolic pressure are (almost) identical for elastic (e.g. aortic) and muscular (e.g. radial) conduit arteries.4,6 The aortic augmented pressure was also measured as the difference between the early-systolic peak (or shoulder) and late-systolic peak pressures. The aortic augmentation index (AIx) was then calculated as the percent ratio of aortic augmented pressure to aortic pulse pressure, and standardized for a heart rate of 75 bpm. The round-trip travel time (TR) of the pressure wave from the heart to the major reflecting sites and back was estimated as the time from the beginning upstroke of the aortic pressure wave to the systolic upstroke of the reflected wave (inflection point).7 Subsequently, the tonometric waveform was recorded in a similar manner on the common femoral artery. Additional recording was also made on the dorsalis pedis artery in a subset of subjects (n = 101). Similarly to the radial waveform, these femoral and dorsalis pedis waveforms were calibrated using brachial pressures, i.e. by equating the mean and diastolic pressure levels of both aortic and peripheral signals.4,6 Thus, the pulse amplification ratios of the aorta-to-femoral and aorta-to-dorsalis pedis regions (AMPA-F and AMPA-DP) were obtained from respective waveforms according to the following equations: AMPA-F = PPF ÷ PPA × 100 (%); and AMPA-DP = PPDP ÷ PPA × 100 (%); where PPF and PPDP represent the femoral pulse pressure and dorsalis pedis pulse pressure, respectively. Again, calculation of these amplifications is free from influence by the blood pressure calibration.4,6 Additionally, the femoral AIx was determined in the same manner as the aortic AIx. Based on the sequential pressure wave recordings, the pulse wave velocity (PWV) was measured, as well. Specifically, the measurements were made centrally from the 3 carotid to femoral artery for all subjects and in addition, distally from the femoral to dorsalis pedis artery for a subset of subjects (n = 101). The carotid-femoral PWV (PWVC–F) measures elastic artery stiffness, while the femoral-dorsal pedis PWV (PWVF–DP) measures muscular artery stiffness.2 The pulse travel time between two arterial sites was calculated from the differences between the R wave of a simultaneously recorded ECG and the foot points of the pressure wave at the respective sites.8 For determination of the carotid-femoral PWV, the travel distance was estimated by subtracting the distance between the carotid site and the suprasternal notch from the distance between the suprasternal notch and the femoral site. For the femoral-dosalis pedis PWV, the travel distance was estimated as linear between the two sites. Hence, PWV was obtained by dividing the travel distance by the transit time. Beat-to-beat PWVs during a steady 11-second period were averaged to be used as representative. Doppler flow measurements The blood flow velocity measurement was made using duplex ultrasonography equipped with a 7.5-MHz linear transducer (Vivid i, GE Healthcare, Tokyo, Japan). Two-dimensional real-time B-mode and bidirectional pulsed Doppler signals were acquired from the proximal straight portion of the common femoral artery at the groin. Care was taken to avoid the level of bifurcation because of changes in the flow velocity profile that can occur there. The scan head was moved until the ultrasound beam was aligned along the arterial axis so that the appropriate longitudinal image was obtained. The spatial length of the Doppler pulse (i.e. sample volume) was chosen large enough to encompass the entire lumen and include the slower moving flow near the vessel wall.9 The wall filter (high-pass filter) was chosen to be as low as possible so that the slower moving flow would be included in the calculation of flow. The direction of the ultrasound beam was adjusted to produce an angle of insonation between 45° and 60°; the angle was minimized as much as the anatomy allowed. Thus, the instantaneous mean velocity was calculated as a spatial average of the intensity-weighted, instantaneous Doppler shift signals within the sample volume. The mean velocity was recorded continuously for 16 seconds, digitized, and stored as time-series data for further analysis. The diameter of the femoral artery was also determined by B-mode imaging at the same site as the Doppler recording. Flow pulse wave analysis The 16-sec data of the femoral flow velocity was interpolated offline every 10 ms and plotted against time using a dedicated program written in Mathematica software 4 (version 4.0). The beat-to-beat pulse waveforms were ensemble-averaged for 10 consecutive pulses (i.e. over the 10 cardiac cycles) using the foot points of the systolic upstrokes for synchronization (BeatScope, BMEYE, Amsterdam). From the averaged waveform, we determined the following parameters in terms of flow velocity and relevant time (Figure 1): systolic forward (maximum) peak velocity (VF); reverse (minimum) peak velocity (VR); end-diastolic velocity (VD); time-averaged mean velocity (VM); acceleration time (TACL, the time from the start of flow to the forward flow peak); and deceleration time (TDCL, the time from the forward flow peak to the reverse flow peak). In most cases, the diastolic forward flow followed the reverse flow, so its peak velocity (VF2) was also measured whenever available. Furthermore, in order to minimize the potential influence of the insonation angle on the absolute flow values, we calculated the following parameters as relative ratios: Reverse-to-forward flow ratio = |VR| ÷ |VF| × 100 (%); Reverse-to-forward flow index = |VR − VD| ÷ |VF − VD| × 100 (%); and Diastolic-to-systolic forward flow ratio = |VF2| ÷ |VF| × 100 (%). In addition, femoral flow volume (ml/min) was calculated from the time-averaged mean flow velocity and the arterial diameter. Femoral vascular resistance (mmHg/ml/min) was obtained by dividing the mean arterial pressure by the flow volume. Statistical analysis Data analyses were performed with SPSS software (version 13.0). Comparisons of continuous variables between two groups were made using Student’s t test, and those among tertile or quatile groups using analysis of variance (ANOVA) with a post-hoc Bonferroni test. Paired t test was used to evaluate intra-subject differences. Comparisons of categorical variables were made using χ2 test. Univariate correlations were evaluated as Pearson’s correlation coefficients (r). Multivariate linear regression analysis was performed to investigate independent correlates of the femoral reverse flow index and diastolic forward flow ratio. For this analysis, the diastolic maximum forward flow velocity was considered zero if the subject had a biphasic waveform with no definite positive diastolic flow. Of the 3 pulse amplifications, aorta-to-femoral amplification was chosen as an explanatory variable to enter into the models because of the closest univariate correlation. Multivariate comparisons of pulse wave parameters between patients with triphasic and biphasic flow were made using analysis of covariance (ANCOVA). Data are provided as means±SD or percentages. All reported P values are 2-sided, and a P value of <0.05 was considered statistically significant. 5 References 1. Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur Heart J. 2006;27:2588-2605. 2. Nichols WW, O'Rourke MF. Mcdonald's blood flow in arteries: Theoretical, experimental and clinical principles. London: Hodder Arnold; 2005. 3. Hashimoto J, Imai Y, O'Rourke MF. Indices of pulse wave analysis are better predictors of left ventricular mass reduction than cuff pressure. Am J Hypertens. 2007;20:378-384. 4. Avolio AP, Van Bortel LM, Boutouyrie P, Cockcroft JR, McEniery CM, Protogerou AD, Roman MJ, Safar ME, Segers P, Smulyan H. Role of pulse pressure amplification in arterial hypertension: Experts' opinion and review of the data. Hypertension. 2009;54:375-383. 5. Hashimoto J, Imai Y, O'Rourke MF. Monitoring of antihypertensive therapy for reduction in left ventricular mass. Am J Hypertens. 2007;20:1229-1233. 6. Benetos A, Thomas F, Joly L, Blacher J, Pannier B, Labat C, Salvi P, Smulyan H, Safar ME. Pulse pressure amplification a mechanical biomarker of cardiovascular risk. J Am Coll Cardiol. 2010;55:1032-1037. 7. Hashimoto J, Westerhof BE, Westerhof N, Imai Y, O'Rourke MF. Different role of wave reflection magnitude and timing on left ventricular mass reduction during antihypertensive treatment. J Hypertens. 2008;26:1017-1024. 8. Wilkinson IB, Fuchs SA, Jansen IM, Spratt JC, Murray GD, Cockcroft JR, Webb DJ. Reproducibility of pulse wave velocity and augmentation index measured by pulse wave analysis. J Hypertens. 1998;16:2079-2084. 9. Holland CK, Brown JM, Scoutt LM, Taylor KJ. Lower extremity volumetric arterial blood flow in normal subjects. Ultrasound Med Biol. 1998;24:1079-1086. 6 Table S1. Patient characteristics according to femoral reverse/forward flow index Tertiles of reverse/forward flow index Lowest Middle Highest <25.8 25.8–32.3 >32.3 Variable (n=46) (n=45) (n=47) Age, y 58 ± 16 57 ± 11 52 ± 11 Women, n (%) 37 (80) 29 (64) 20 (43) Height, cm 156 ± 8 160 ± 9 163 ± 9 Weight, kg 59 ± 12 66 ± 14 67 ± 14 Body mass index, kg/m2 24.0 ± 4.6 25.7 ± 4.2 24.7 ± 3.5 Total cholesterol, mg/dl 179 ± 35 178 ± 28 193 ± 61 High-density lipoprotein cholesterol, mg/dl 53 ± 15 50 ± 13 54 ± 17 Low-density lipoprotein cholesterol, mg/dl 100 ± 30 104 ± 28 110 ± 46 Fasting blood glucose, mg/dl 111 ± 47 102 ± 18 104 ± 33 Hemoglobin A1c, % 5.8 ± 1.2 5.7 ± 1.3 5.4 ± 0.5 Hypercholesterolemia, n (%) 18 (39) 13 (29) 13 (28) Diabetes, n (%) 16 (35) 12 (27) 13 (28) Brachial systolic blood pressure, mmHg 129 ± 22 121 ± 15 126 ± 17 Brachial diastolic blood pressure, mmHg 66 ± 11 68 ± 9 73 ± 10 Mean arterial pressure, mmHg 88 ± 13 86 ± 10 91 ± 12 Heart rate, bpm 65 ± 8 65 ± 10 64 ± 10 Aortic systolic blood pressure, mmHg 117 ± 21 109 ± 14 113 ± 16 Aortic augmented pressure, mmHg 15 ± 9 10 ± 7 9 ± 5 Aortic augmentation index (AIx), %* 28 ± 10 24 ± 10 23 ± 11 Round-trip travel time (TR), ms 134 ± 9 140 ± 10 140 ± 7 Femoral augmentation index, %* −6 ± 11 −9 ± 13 −13 ± 18 Pulse Amplification, % Aorta-to-radial (AMPA–R) 128 ± 16 134 ± 15 135 ± 18 Aorta-to-femoral (AMPA–F) 122 ± 11 128 ± 13 134 ± 16 Aorta-to-dorsalis pedis (AMPA–DP)† 171 ± 32 173 ± 26 194 ± 28 Pulse wave velocity, m/s Carotid-femoral (PWVC–F) 8.5 ± 2.4 7.6 ± 1.8 7.5 ± 1.8 Femoral-dorsalis pedis (PWVF–DP)† 8.8 ± 1.5 9.3 ± 1.4 9.0 ± 1.7 Femoral artery diameter, mm 7.4 ± 0.9 8.2 ± 0.9 8.3 ± 1.1 Femoral vascular resistance, mmHg/ml/min 0.31 ± 0.19 0.28 ± 0.13 0.39 ± 0.30 Femoral reverse/forward flow index, % 19.7 ± 4.3 29.0 ± 1.9 39.6 ± 6.9 *Standardized for heart rate of 75 bpm. †Data available in 101 subjects. 7 P 0.08 0.001 0.001 0.006 0.13 0.19 0.46 0.39 0.41 0.10 0.43 0.65 0.12 0.007 0.18 0.82 0.08 <0.001 0.03 0.002 0.05 0.13 <0.001 0.002 0.04 0.39 <0.001 0.03 <0.001 Table S2. Significant independent predictors of femoral reverse/forward flow index and diastolic/systolic forward flow ratio Variable β P 0.05 3.4 0.43 0.13 0.26 0.30 −0.22 0.32 0.002 <0.001 0.02 0.01 −0.56 ± 0.20 −0.12 ± 0.03 0.07 ± 0.02 −0.22 −0.30 0.19 0.006 <0.001 0.007 Regression coefficient ± SE Model for reverse/forward flow index (R2=0.30, P<0.001)* Aorta-to-femoral pulse amplification, % Femoral vascular resistance, mmHg/ml/min Carotid-femoral PWV, m/s Body height, cm Model for diastolic/systolic forward flow ratio (R2=0.48, P<0.001)* Carotid-femoral PWV, m/s Age, years Aorta-to-femoral pulse amplification, % 0.17 12.8 −1.03 0.33 ± ± ± ± β, standardized regression coefficient; PWV, pulse wave velocity. *Variables included in the multiple linear regression models were age, gender, height, hypercholesterolemia, diabetes, femoral vascular resistance, aorta-to-femoral pulse amplification, and carotid-femoral PWV. Only significant predictors were listed in. 8 Table S3. Patient characteristics according to femoral diastolic/systolic forward flow ratio Tertiles of diastolic/systolic forward flow ratio Lowest Middle Highest <10.1 10.1–14.66 >14.66 Variable (n=45) (n=47) (n=46) Age, y 64 ± 12 54 ± 11 50 ± 12 Women, n (%) 35 (78) 28 (60) 33 (50) Height, cm 156 ± 9 161 ± 9 163 ± 9 Weight, kg 59 ± 11 66 ± 15 66 ± 13 Body mass index, kg/m2 24.2 ± 4.4 25.4 ± 4.1 24.9 ± 3.9 Total cholesterol, mg/dl 183 ± 33 184 ± 33 183 ± 62 High-density lipoprotein cholesterol, mg/dl 49 ± 13 52 ± 17 55 ± 14 Low-density lipoprotein cholesterol, mg/dl 105 ± 30 107 ± 32 103 ± 44 Fasting blood glucose, mg/dl 116 ± 47 105 ± 33 97 ± 12 Hemoglobin A1c, % 6.0 ± 1.3 5.7 ± 1.2 5.3 ± 0.4 Hypercholesterolemia, n (%) 17 (38) 20 (43) 7 (15) Diabetes, n (%) 21 (47) 16 (34) 4 (9) Brachial systolic blood pressure, mmHg 131 ± 19 126 ± 19 119 ± 14 Brachial diastolic blood pressure, mmHg 66 ± 9 72 ± 11 69 ± 10 Mean arterial pressure, mmHg 89 ± 11 90 ± 14 86 ± 11 Heart rate, bpm 65 ± 8 65 ± 9 64 ± 10 Aortic systolic blood pressure, mmHg 120 ± 18 114 ± 17 106 ± 14 Aortic augmented pressure, mmHg 17 ± 8 10 ± 5 8 ± 5 Aortic augmentation index (AIx), %* 25 ± 6 20 ± 8 15 ± 11 Round-trip travel time (TR), ms 133 ± 8 138 ± 10 142 ± 7 Femoral augmentation index, %* −4 ± 9 −7 ± 16 −16 ± 14 Pulse Amplification, % Aorta-to-radial (AMPA–R) 124 ± 10 133 ± 15 139 ± 20 Aorta-to-femoral (AMPA–F) 119 ± 10 128 ± 15 136 ± 14 Aorta-to-dorsalis pedis (AMPA–DP)† 158 ± 25 186 ± 24 197 ± 30 Pulse wave velocity, m/s Carotid-femoral (PWVC–F) 8.9 ± 2.3 7.7 ± 1.8 7.0 ± 1.6 Femoral-dorsalis pedis (PWVF–DP)† 8.9 ± 1.4 9.0 ± 1.7 9.2 ± 1.6 Femoral artery diameter, mm 7.5 ± 1.0 8.0 ± 1.1 7.9 ± 1.1 Femoral vascular resistance, mmHg/ml/min 0.34 ± 0.21 0.34 ± 0.22 0.30 ± 0.24 Femoral diastolic/systolic forward flow ratio, % 6.3 ± 3.5 12.5 ± 1.3 17.2 ± 2.4 *Standardized for heart rate of 75 bpm. †Data available in 101 subjects. 9 P <0.001 0.02 0.001 0.008 0.37 0.99 0.16 0.89 0.03 0.009 0.01 <0.001 0.004 0.03 0.20 0.68 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 0.001 0.81 0.007 0.64 <0.001 Table S4. Comparison between subjects with triphasic and biphasic femoral flow Femoral flow waveform Variable Age, y Triphasic Biphasic (n = 129) (n = 9) 54 Women, % ± 12 76 60 Height, cm ± 11 100 P <0.001 0.02 161 ± 9 150 ± 6 0.001 65 ± 14 53 ± 10 0.02 Body mass index, kg/m 24.9 ± 4.1 23.8 ± 4.4 0.47 Total cholesterol, mg/dl 182 ± 45 198 ± 38 0.29 High-density lipoprotein cholesterol, mg/dl 53 ± 15 47 ± 14 0.32 Low-density lipoprotein cholesterol, mg/dl 104 ± 35 118 ± 46 0.26 Fasting blood glucose, mg/dl 105 ± 34 118 ± 38 0.29 Hemoglobin A1c, % 5.6 ± 1.1 6.5 ± 1.2 0.03 Weight, kg 2 Hypercholesterolemia, % 31 44 0.40 Diabetes, % 27 67 0.01 Brachial systolic blood pressure, mmHg 124 ± 18 138 ± 22 0.03 Brachial diastolic blood pressure, mmHg 70 ± 10 59 ± 9 0.004 Mean arterial pressure, mmHg 88 ± 12 87 ± 13 0.73 Heart rate, bpm 65 ± 9 66 ± 10 0.72 112 ± 17 125 ± 20 0.03 Aortic augmented pressure, mmHg 11 ± 7 22 ± 10 <0.001 Aortic augmentation index (AIx), %* 19 ± 9 28 ± 5 0.007 Round-trip travel time (TR), ms 139 ± 9 127 ± 7 <0.001 Femoral augmentation index, %* −10 ± 15 −5 ± 5 0.03 Aorta-to-radial (AMPA-R) 133 ± 17 121 ± 7 0.001 Aora-to-femoral (AMPA-F) 128 ± 15 118 ± 6 0.001 Aorta-to-dorsalis pedis (AMPF-DP)† 182 ± 30 147 ± 23 0.001 Carotid-femoral (PWVC-F) 7.7 ± 1.9 10.5 ± 2.9 <0.001 Femoral-dorsalis pedis (PWVF-DP)† 9.0 ± 1.5 9.3 ± 1.4 0.63 8.0 ± 1.0 7.0 ± 1.1 0.008 0.31 ± 0.21 0.53 ± 0.29 0.005 Aortic systolic blood pressure, mmHg Pulse amplification, % Pulse wave velocity, m/s Femoral artery diameter, mm Femoral vascular resistance, mmHg/ml/min *Standardized for heart rate of 75 bpm. †Data available in 101 (93 triphasic and 8 biphasic) subjects. 10 Flow velocity (cm/s) A B 60 100 30 50 0 0 0.5 1 0.5 -30 1 -50 Time (s) Figure S1. Two representative types of the femoral flow velocity waveform. (A) is a triphasic waveform of a 43-year-old man. The waveform was composed of initial systolic forward, secondary reverse and tertiary diastolic forward phases. As shown in this example, the tertiary diastolic forward flow was occasionally followed by additional small flow oscillations. (B) is a biphasic waveform of a 62-year-old woman with diabetes. Note that the diastolic forward flow is absent. 11