Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neonatal infection wikipedia , lookup
Hepatitis B wikipedia , lookup
Meningococcal disease wikipedia , lookup
Cysticercosis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Anthrax vaccine adsorbed wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
Whooping cough wikipedia , lookup
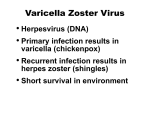
Picture courtesy of Centers for Disease Control and Prevention (2011). Chickenpox Varicella Photos. Retrieved on 10/23/13 from http://www.cdc. gov/chickenpox/about/pho tos.html. Reducing Varicella Complications in Women of Lynn M. Scott, RN, IBCLC Childbearing Age SUNYIT, NUR 490 November 12, 2013 Background • Varicella is predominantly a childhood disease (also known as chickenpox) that is highly contagious and is caused by the varciella zoster virus (VZV) . • With the exception of pregnant women, anyone born in the U.S. prior to 1980 is assumed to be varicella immune. Nursing Theory Thielen (2012) states: “Pregnancy itself is not an illness or disease state; rather, it should be seen as a state of wellness. To facilitate behavior that promotes health and wellness, Pender’s (Nola J.) health and wellness model fosters the use of nursing interventions that empower the client’s ability to self-care through education …” (p. 211). Methods • Most severe cases of chickenpox develop in immunocompromised individuals, adults, and pregnant women and their fetuses. • If VZV is contracted during the first and second trimester (between the 5th and 24th weeks) of pregnancy, spontaneous abortion and premature labor may occur, or the baby may be born with varicella pneumonia, neonatal varicella herpes zoster, or Congenital Varicella Syndrome (CVS), which includes abnormalities of the limbs, central nervous system and cognitive impairment, seizures, and growth deficiency. The information provided in this presentation was obtained from an integrative literature review of 12 articles obtained from CINAHL and Medline via EBSCO host and include the following types of research and informative literature: Comparative study, cross-sectional study, case study, supplements (3), research letter, pediatric review, vaccine standing orders, critical review, vaccine recommendations, and patient information sheet. • CVS, documented as 14 cases in 2,000 deliveries, carries a 30% mortality rate in the first few months of lie. • While at risk for various complications, varicella pneumonia, a high risk complication of VZV in pregnant women, is the most common cause of mortality in this population. • In 2005, the Advisory Committee on Immunization Practices (ACIP) recommended routine screening during pregnancy for evidence of immunity to varicella and postpartum vaccination of women without such evidence. EVIDENCE OF VARICELLA IMMUNITY History of varicella or herpes zoster Documentation of 2 doses of varciella vaccine at least4 weeks apart Lab confirmation of varicella immunity with IgG ELISA lab studies Objectives PICO QUESTION: • Taking into consideration the pros and cons of administering the varicella vaccine, will vaccinating women in the immediate postpartum period decrease the reportable incidences of mortality and morbidity from complications of varicella in childbearing-aged women and, subsequently, their newborns? • Population: Women of childbearing age during the immediate postpartum period; • Intervention: Vaccination with the varicella vaccine; • Comparison: Pros and cons of vaccination, and; • Outcome: A decrease in the reportable incidences of mortality and morbidity from complications of varicella in childbearing-aged women and, subsequently, their newborns. Infant with hemorrhagic varicella infection with cellulitis. Picture courtesy of American Academy of Pediatrics (no date). Press Room Photos. Retrieved 10/28/13 from http://www.aap.org/enus/about-the-aap/aappress-room/aap-pressroom-mediacenter/pages/AAPPressroomPhotos.aspx. • • EVALUATION STRATEGY PROS CONS 1. Since the start of the varicella vaccine 1. The extent to which vaccinated individuals program in 1995, there has been an harbor latent infection with vaccine380.9% reduction in the number of related VZV and the contribution of this varicella cases. towards protective immunity against VZV 2. Varicella vaccine will help protect the is unknown. public from the risks and costs of the 2. There are several potential adverse effects complications of varicella. of the varicella vaccine: 3. Overall adverse effects of the varicella • Transmission of varicella from a vaccine were 2.6 cases per 100,000 recently vaccinated individual (5 distributed doses. cases in 55 million distributed 4. The components of the varicella doses); vaccine have not been found in human • Development of chickenpox or breastmilk. herpes zoster (rare) in vaccinated 5. It has been documented that VZV can individuals; occur as IgG levels can wane over time. • Primary failure of vaccine 6. Reinfection with VZV might occur (infection) and secondary failure of even after natural exposure or infection. vaccine (reinfection); 7. Out of 600 women listed in the • Discomfort at injection site; • Anaphylactic reaction, seizures, VARIVAX® Pregnancy Registry (in Stephen Johnson Syndrome, conjunction with the Centers for encephalopathy, rash, etc. Disease Control and Prevention) that 3. Women who are vaccinated should avoid were inadvertently vaccinated against becoming pregnant for 1 month after each varicella during or around pregnancy, vaccine injection. there were no reported cases of CVS. 8. The risk of an infant developing birth defects due to their seronegative mother’s exposure to the varicella vaccine during the highest risk period is similar to the reported prevalence rate in the general population. 9. The varicella vaccine is 70%-100% effective if administered within 72 hours of exposure to an individual infected with VZV. 10. Varicella-related morbidity and mortality have dramatically decreased in countries where varicella vaccination has been introduced. As a result of the information obtained through the research contained herein, policy, protocol, and standing orders on Varicella Vaccine for Postpartum Women are being created for this author’s employer under the advisement of the institution’s Executive Director. Conclusions Evidence • Prevention of VZV infection in pregnant women through the vaccination of childbearing-aged women is key to continuing the documented reduction of varicella-related maternal and neonatal morbidity and mortality. The decline in the number of cases of VZV has decreased the exposure but increased the susceptibility of women to this virus in their childbearing years. • Varicella vaccination is a safe and effective intervention to prevent VZV infections and complications of the disease in women of childbearing age with 99% immunity protection by administering two doses of VARIVAX®, 4 weeks apart, in postpartum women. Pregnant women who are exposed to VZV in the low-risk period of gestation should be evaluated as soon as possible through physical examination and serology testing. Post-exposure prophylaxis with Varicella Zoster Immune Globulin (VariZIG®) as soon as possibly close to exposure should be considered for susceptible candidates in order to avoid potential complications in the pregnant mother (e.g., bacterial superinfection of skin lesions, pneumonia, acute cerebellar ataxia, encephalitis, thrombocytopenia, and Reye Syndrome). It is important that these women are followed up with varicella vaccine upon completion of their pregnancy.. • When pregnant mothers develop VZV between 5 days prior to delivery and 2 days after delivery, their newborns are at high risk for severe varicella complications, specifically an untreated mortality rate as high as 31%, usually from varicella pneumonia. • The assessment of serological data is essential for the appropriateness and impact of counseling, screening, and vaccination for varicella • Healthcare providers should educate their patients about the benefits of varicella vaccination. Indications for the Varicella Vaccine • Implementation All adults who do not show evidence of immunity to varicella unless they have one of the following contraindications: Contraindications to the Varicella Vaccine (In childbearing-aged women specifically) • History of allergy or anaphylactic reaction to components of varicella vaccine; • Pregnancy or anticipated pregnancy within 1 month; • Any malignant conditions including blood dyscrasias, leukemia, lymphoma, or any other types of malignant neoplasms of the bone marrow or lymphatic system; • Currently receiving high-dose immunosuppressive therapy (e.g., two weeks or more of 20 mg or greater Prednisone); • CD4 and T-Lymphocyte count <200 cells/uL, and; • Family history of congenital/hereditary immunodeficiency in a firstdegree relative. Precautions to the Varicella Vaccine • Receipt of antibody-containing blood products within the past 11 months, and; • Moderate to severe acute illness with or without a fever. References Centers for Disease Control and Prevention (2013). MMWR: Updated recommendations for use of VariZIG® - United States, 2013. Retrieved on 10/23/13 from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6228a4.htm. FDA.gov (2010). Patient information about Varivax®. Retrieved on 10/23/13 from http://www.fda.gov/downloads/BiologicsBloodVaccines/Vaccines/ ApprovedProducts/UCM165651.pdf. Guido, M., Tinelli, A., DeDonno, A., Quattrochi, M., Malvasi, A., Camplilongo, F., & Zizza, A. (2012). Susceptibility to varicella zoster among pregnant women in the province of Lecce, Italy. Journal of Clinical Virology, 53, 72-76, doi: 10.1016/j.jcv2011.10.007. Hackley, B. (2008). Incorporating immunization services into reproductive healthcare. Journal of Midwifery & Women’s Health, 53(3), 175-187. doi: 10.1016/j.jmwh.2008.01.002. Hambleton, S., Steinberg, S. P., LaRussa, P. S., Shapiro, E. D., & Gershon, A. A. (2008). Risk of herpes zoster in adults immunized with varicella vaccine. The Journal of Infectious Diseases, 197, S196-S199. doi: 10.1086/522131. Hendriksz, T. (2011). Vaccines for measles, mumps, rubella, varicella, and herpes zoster: Immunization guidelines. Journal of the American Osteopathic Association, 111(10), S10-S12. Immunization Action Coalition (2013). Standing orders for administering varicella (chickenpox) vaccine to adults. Retrieved on 10/01/13 from http://www.immunize.org/catg.d/p3080.pdf. Kett, J. C. (2013). Perinatal varicella. Pediatrics in Review, 34(1), 49-51. doi: 10.1542/pir.34-1-49. Picone, O., Vauloup-Fellous, C., Senat, M. V., Frydman, R., & GrangeotKeros, L. (2008). Maternal varicella infection during pregnancy in a vaccinated patient. Prenatal Diagnosis, 28, 971-972. doi: 10.1002/pd.2083. PubMed.gov (2005). Chickenpox vaccines: New drugs. A favourable riskbenefit balance in some situations. Prescrire International, 14(77), 85-91. Thielen, K. (2012). Exploring the group prenatal care model: A critical review of the literature. The Journal of Perinatal Education, 21(4), 209-218, doi: http://dx.doi.org/10.1891/1058-1243.21.4.209. Wilson, E., Goss, M. A., Marin, M., Shields, K. E., Seward, J. F., Rasmussen, S. A., & Sharrar, R. G. (2008). Varicella vaccine: Exposure during pregnancy. The Journal of Infectious Diseases, 197, S178-S184. doi: 10.1086/522136.