Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
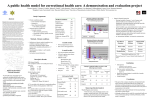
Improving Access to and Utilization of Health and Social Services for HIV-infected Jail and Prison Releases: Evaluation Results from the Corrections Demonstration Project Sofia S. Kennedy, Abt Associates Inc., Cambridge, Massachusetts USA Ted Hammett, Abt Associates Inc., Cambridge, Massachusetts USA Ronald Braithwaite, Rollins School of Public Health, Emory University, Atlanta Georgia USA Kimberly Jacob Arriola, Rollins School of Public Health, Emory University, Atlanta Georgia USA Expanded Access to HIV Services in Correctional Facilities Background Rates of HIV/STIs are up to five times higher among US inmates than in the total population Inmates have a legal right to health care in prison/ jail but often do not have access to health and social services after release, and are often denied services post-release because of their criminal record or the behavior that led to their arrest (e.g., drug sales) Funding The Corrections Demonstration Project (CDP) is funded by two US federal agencies: the Centers For Disease Control and Prevention and the Health Resources and Services Administration CDP Interventions Continuity of care: pre-release discharge planning & post-release case management HIV/STI testing & treatment, HIV prevention, peer educator training, staff training (not addressed in this poster) CDP Intervention Sites Departments of public health in six states (California, Florida, Georgia, Massachusetts, New Jersey and New York) and one city (Chicago, Illinois) were funded Services are provided in jails (non-sentenced & sentenced inmates, short sentences), prisons (sentences of >1 year), juvenile facilities, alternative & transitional correctional settings and in the community after release Evaluation Background Participation in the program and the evaluation is voluntary The evaluation follows clients from program recruitment (during incarceration) through 6 months after release Evaluation is ongoing Preliminary results from 30 days after release presented here Continuity of Care For People Living With HIV Being Released From Correctional Facilities Public Health Departments partnered with correctional facilities and contracted with NGOs to provide services NGO case managers work with inmates living with HIV (and some HIV-negatives) in the correctional facility Assess post-release needs related to: medical, mental health and substance abuse treatment, housing, benefits, employment, family and HIV prevention Provide discharge planning prior to release (make appointments for and referrals to post-release services) Provide case management in the community after release (escort client to appointments, make additional appointments & referrals, provide support during the transition) Transition client to permanent long-term case manager Table 1: Total clients served and participating in the evaluation Program Clients1 Longitudinal Evaluation Clients 30-Day Follow-up3 Served 2 Recruited3 Released3 Jail 3757 658 267 237 Prison 2103 448 335 247 Total 6027 1106 602 484 1 California data are not included, not participating in the client-level evaluation 2 February 2000-March 2004 (program start dates vary by site) 3 January 2001-September 2003 (evaluation start dates vary by site) Table 2: Service Utilization Before and After Incarceration (Prison Clients) Prior to 30 Days Post P-value Incarceration Release Total 247 HIV+ 211 (85.4%) 1 Mental Health Diagnosis 86 (34.8% )1 HIV Care 116 (55.0)2 165 (78.2)2 <0.0001 HIV Meds 87 (41.2)2 145 (68.7)2 <0.0001 Mental Health Care 37 (43.0)3 29 (33.7)3 NS Substance Abuse Treatment 84 (34.0)1 107 (43.3)1 0.0221 1 % of all clients 2 % of HIV-infected clients 3% of clients with a mental health diagnosis Discussion Almost 20% of clients served participated in the evaluation Not all clients were offered the option to be in the evaluation due to delays in the implementation of the evaluation (e.g., instrument development, IRB approval, site readiness) Over half the clients recruited for the evaluation were released and eligible for community services 80% of releasees were in case management 30 days after release Prison Programs Significantly more clients received HIV care, took HIV medication and participated in drug treatment after release than before prison This population may be interested in case management because they have been incarcerated for one or more years and may have initiated treatment in prison and never had HIV care in the community Jail Programs (n= 237) Significantly fewer clients received HIV care after release than before jail (data not shown) There were no other significant changes Less than half the program clients were released to community case management Clients who have been in jail for a short time may still be connected to community services Clients who receive care in jail may not need to see a provider right after release Lessons Learned/Recommendations Partnerships between correctional facilities (especially prisons), public health entities and NGOs help inmates to transition back to the community Connecting releasees to HIV care and medications can reduce the spread of resistant strains of HIV and may reduce the risk of transmission Connecting releasees to substance abuse treatment may reduce the risk of recidivism for drug-related crimes Access to some services in the community is limited Housing and mental health and substance abuse treatment are scarce Programs can and do bar people with criminal records (especially drug offenses) from services Jail-based programs are less common than prison programs and models may have to be altered to meet the needs of this population The high volume of clients, short stays and not being released to the community all need to be addressed For more information and final evaluation results contact: Sofia Kennedy Abt Associates Inc 55 Wheeler Street Cambridge MA 02138 USA +1-617-349-2797 [email protected] www.abtassoc.com www.sph.emory.edu/HIVCDP/index.html