Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
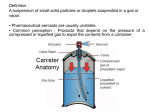
G E N E R A L I N T E R E S T Basics of Compounding Table 1. General Formula Components for Oral, Inhalation Inhalation, and Nasal Aerosol Preparations. Preparations Loyd V. Allen, Jr, PhD, RPh Drugs can be introduced into the lungs easily by the patient’s inhaling a dose of a drug in a properly designed dosage form that is caught up in the flow of air and carried into the deep recesses of the pulmonary environment. Drugs in the form of a vapor, a very fine powder, or a solution in the form of an aerosol can usually be transported by the airstream into the respiratory bronchioli and the alveolar region. An aerosol is generally a dispersed system consisting of a solid or liquid internal phase in an outer gaseous phase. Examples of a natural aerosol are a mist (water/air) or a dust (solid/air). Products administered by inhalation can produce either a local or a systemic effect. Drugs commonly administered for respiratory purposes include bronchodilators, corticosteroids, antitussives, expectorants, surfactants, respiratory stimulants, and therapeutic gases. There are numerous advantages to using oral inhalation products, including a rapid onset of action, elimination of the first-pass effect, avoidance of drug degradation in the gastrointestinal tract, use of low dosages that minimize adverse reactions, dose titration capability, flexibility in dosing, and providing an alternate route of administration when other drugs may chemically or physically interact with concurrent drugs or when drugs with erratic oral or parenteral administration pharmacokinetics are used. The ultimate deposition of inhalation aerosols is dependent on the product’s formulation; the design of components, packaging, and container; the administration skills and techniques of the product user; and the anatomic and physiologic status of the respiratory system. Numerous terms are used to describe the various dosage forms and methods of drug administration by inhalation, including aerosols, atomizers, inhalations, insufflations, metered dose inContinuing Education Goal: To provide pharmacists, pharmacy students, and pharmacy technicians with supportive information on the basics of extemporaneous compounding various types of inhalation products. Objectives: After reading and studying the article, the reader will be able to: 1. define the different types of inhalation products. 2. discuss the methods of extemporaneously preparing inhalation products. 3. detail the preliminary steps involved in preparing to extemporaneously compound. 4. use appropriate equipment and techniques to prepare and appropriately package various types of inhalation products. 452 International Journal of Pharmaceutical Compounding Vol.4 No.6 November/December 2000 Component Active ingredient Solvents Antioxidants Preservatives Buffers Tonicity adjustment Surfactants Vehicle Example Solubilized or suspended Ethyl alcohol, propylene glycol, purified water Ascorbic acid, bisulfites Benzalkonium chloride Phosphate buffers Sodium chloride Sorbitan esters Purified water halers, nebulizers, and vaporizers. By definition, an aerosol is a colloidal dispersion of a liquid or a solid in a gas. Oral inhalation and nasopharyngeal medications can both be administered in the form of an aerosol. Those products are commonly produced by means of manual sprays or from pressurized packages. Aerosols have become so widespread in use that the term now refers to a self-contained product that is sprayed and that has either a liquefied or a compressed gas as a propelling force. For pulmonary delivery, particles greater than 60 µ are usually deposited in the trachea, and those greater than 20 µ are deposited between the trachea and the bronchioles (but not into the bronchioles). Particles that are about 1µ in size often remain airborne and are exhaled. Consequently, particles that are from about 5 to 20 µ are desired if the bronchioles are to be reached. Inhalation aerosols are the largest group of oral aerosol products formulated either as solutions or suspensions. Factors influencing the deposition of inhalation aerosols include the formulation, the device, the administrative technique of the user, and the anatomic and physiologic status of the respiratory system. An atomizer is an instrument used to disperse a liquid in a fine spray. Many of the older pressure-type atomizers used the Bernoulli principle. When a stream of air moves at a high velocity over the tip of a dip tube, the pressure is lowered; this results in the liquid’s being drawn into the airflow. The liquid is broken up into a spray as it is taken up into the airstream. To produce smaller droplets, a baffle, a bead, or another device may be put in the flow to break the droplets into smaller droplets as they collide with the stationary device. Those smaller droplets are then carried by the airflow into the inhaled stream of air. Many different configurations are available when the Bernoulli principle is used. A finer spray can be obtained by using a pressure-type atomizer. Today’s plastic spray bottles are similar to pressure atomizers. When the plastic bottle is squeezed, the air inside is compressed, which forces the liquid up a dip tube into the tip. The liquid stream is mixed with air as it is emitted from the nozzle, thus producing a spray. Inhalations are preparations designed to deliver the drug into the respiratory tree of the patient for local or systemic effect. G E N E R A L Rapid relief is obtained when the vapors, the mist, or the droplets reach the affected area. The USP 24/NF 19 definition of inhalations states that “inhalations are drugs or solutions or suspensions of one or more drug substances administered by the nasal or oral respiratory route for local or systemic effect.” The drugs may be nebulized to produce droplets sufficiently fine and uniform in size to reach the bronchioles. The mist may be breathed directly from the nebulizer of a face mask, or a tent or an intermittent positive pressure breathing (IPPB) machine may be used to produce a contained environment that maximizes the quantity of drug available in the breathing environment for delivery into the lungs. Inhalants are drugs that are characterized by a high vapor pressure and that can be carried by an air current into the nasal passage, where they usually exert their effect. The device or container from which the inhalant is usually administered is called an inhaler. An inhalant consists of cylindrical rolls of a fibrous material that has been impregnated with the drug and that usually contains an aromatic substance in addition to an active substance. Those devices are often cylindrical and have a cap in place to retard the loss of the medication. When the device is used, the cap is removed and the inhaler is inserted into a nostril. When the patient inhales, the air passes through the inhaler and carries the vapor of the medication into the nasal passage. An actual drug vapor is delivered to the patient. For example, menthol, camphor, amyl nitrite, propylhexedrine, and tuaminoheptane inhalants are of that type. Another type, the amyl nitrite inhalant, is packaged so that the drug is contained in a thin glass ampule encased in a gauze netting. When the product is squeezed and the glass ampule is broken, the amyl nitrite is released and is absorbed on the gauze netting for inhalation by the patient. Nebulae, or spray solutions, were intended for spraying into the throat and nose. Generally, those were simple solutions. Sprays in plastic spray bottles work in a manner similar to that of pressure atomizers. When the flexible plastic container is squeezed, the air is compressed, which forces the liquid in the container up through a dip tube into the tip, where it mixes with a stream of air. Droplets are formed, depending on the geometry of the device and the pressure of the individual who is squeezing the bottle. The Latin term for mist is “nebula.” A nebulizer is a small, vacuum-type atomizer inside a chamber. When a nebulizer is used, large droplets strike the walls of the chamber and then fall back and are reprocessed. The smaller particles are carried in the airstream out of the unit. The patient using the nebulizer places it into his or her mouth and inhales while simultaneously squeezing the bulb. For a nebulizer to be suitable for the administration of inhalation solutions, it must produce droplets sufficiently fine and uniform in size (optimally 0.5 to 7 µ) to enable the mist to reach the bronchioles. A vaporizer is an electrical device that produces moist steam that does or does not contain medication for inhalation. A vaporizer is often used to soothe upper respiratory irritations but is relatively ineffective in providing medications to the deeper areas of the respiratory tract. I N T E R E S T Composition Solution aerosols can be formulated rather easily, but if their formulation is difficult, a suspension or emulsion aerosol can be prepared. Either solution or suspension aerosols are used for oral inhalation. Examples of ingredients in oral inhalation and nasal aerosol solutions or suspensions are shown in Table 1. Citric acid is often used in those formulations as an acidifying agent. Polysorbate 80 is used as an emulsifying and a solubilizing agent. Sodium chloride and dextrose are used as tonicity-adjusting agents. Physicochemical Considerations When products for oral inhalation are compounded or formulated, the variables to consider include particle size, solubility, vehicles, tonicity, pH, sterility, preservatives, viscosity, buffers, surfactants, and moisture content. Particle Size Usually, the particle size should lie within the range of about 0.5 to 10 µ (more preferably between about 3 to 6 µ) for a drug that, International Journal of Pharmaceutical Compounding 453 Vol.4 No.6 November/December 2000 G E N E R A L I N T E R E S T when inhaled, is intended to penetrate to the small bronchioles and the lung alveoli and to provide a rapid effect. This size range of particles is deposited in the lung by gravitational sedimentation, by inertial impaction, and by diffusion into terminal alveoli via Brownian motion. With respect to inhalation aerosols, particles 5 to 10 µ are common; for topical sprays, 50 to 100 µ are common. Solubility Active drugs that are soluble in the matrix and in the pulmonary fluids have a rapid onset of action and usually a shorter duration of action when compared with drugs that are somewhat less soluble in the matrix and in the pulmonary fluids. Drugs that are poorly soluble in the pulmonary fluids may cause problems by irritating the lung tissue. For suspensions, it is best to select a vehicle in which the drug is not very soluble to minimize the phenomenon of particle size growth, which occurs when the drug in solution crystallizes out onto the crystals that are present. Polymorphic forms of crystalline drugs should not be used for suspension aerosols. To enhance the stability of a suspension aerosol, the selection of a liquid phase with a density similar to that of the suspensoid will minimize the tendency to settle. Vehicle Commonly used vehicles that carry the drugs in inhalations include sterile water for inhalation or 0.9% sodium chloride inhalation solution. Some inhalations are simple solutions of nonvolatile or volatile medications in water or cosolvent mixtures. Small quantities of alcohol or glycerin may be used to solubilize ingredients. Tonicity Usually, it is best to have inhalation solutions that are isotonic with physiologic fluids, ie, that are equivalent to 0.9% sodium chloride, or an osmolality of about 290 mOsm. To enhance movement of the fluid and drug through the alveoli, it may be best to have the solution slightly hypotonic. When the solution is hypertonic, fluids have a tendency to move from the alveoli into the pulmonary space to reach an isotonic equilibrium. If the solution is hypotonic, the administered drug solution may have a greater tendency to move into the tissue, which produces more rapid absorption and greater therapeutic effect. pH A pH in the neutral range similar to that of body fluids minimizes any cough reflex that might occur when the pH is too low. However, the solubility and stability characteristics of the drug must be considered. Sterility A new requirement for inhalation solutions is sterility. That requirement was instituted as a result of contamination problems with different inhalation solution products and adverse experience reports of commercially available products. Sterility can be easily accomplished by using 0.2 µ filtration systems designed for extemporaneous compounding. Preservative Any preparation that is not in unit dose containers should contain a preservative, especially because of the latest requirement of sterility for this class of dosage forms. The minimum amount of preservative that is still effective should be used. If too high a concentration is used, it may initiate a cough reflex in the patient. Also, too high a concentration of certain preservatives that are also surfactants may result in foaming that may interfere with the delivery of the complete dose. Viscosity The viscosity of the external phase for most aerosol products is very low, and as a result they are very sensitive systems. Evaporation, sedimentation, and an increase in the particle size are processes that may occur and may change rapidly. Buffer A buffer, if used, should be at low buffer strength to maintain the desired pH and to not induce pH changes in a microenvironment in the pulmonary cavity. 454 International Journal of Pharmaceutical Compounding Vol.4 No.6 November/December 2000 G E N E R A L Surfactants Surfactants can be used as dispersing agents for suspensions, as solubilizing agents to enhance the solubility of the drug, and as spreading agents when the drug is deposited in the lungs. The sorbitan esters (especially sorbitan trioleate) are used, as well as lecithin derivatives, oleyl alcohol, and others. One should be cautious and should keep the surfactant concentration as low as possible to minimize foaming that might interfere with proper administration. Moisture Content For inhalation dispersion aerosols in general, the moisture content should be kept extremely low for all active and inactive ingredients. The ingredients should be anhydrous to minimize caking. Preparation Methods and Techniques 1. Calculate the quantity of the individual ingredients required for the total amount to be prepared. 2. Accurately weigh/measure each of the ingredients. 3. Dissolve the solids in about 2/3 of the volume of vehicle for 4. 5. 6. 7. I N T E R E S T the preparation. Add the liquid ingredients and mix well. Add sufficient vehicle to volume and mix well. Filter through a 0.2 µ filter system into sterile containers. Package and label. Specific Quality Control Solutions should be checked for precipitation, discoloration, haziness, gas formation caused by microbial growth, final volume, and sterility. Storage and Labeling Usually, oral inhalation preparations should be stored at either room temperature or refrigerated temperature. Stability Without stability information that is applicable to a specific drug and preparation, a beyond-use date for water-containing formulations should be not later than 14 days when stored at cold temperatures for products prepared from ingredients in solid form. A similar commercially available product with an extended date can be taken into consideration. However, a maximum of 6 months should be used for compounded preparations. ■ Examples The example formulas illustrated here are for preservative-free formulations. These should be packaged as single-use or unit-dose products. Formulations are provided for 100 mL quantities for ease of calculations. The formulas should be reduced or expanded according to the total quantity to be compounded. These solutions can be preserved by the addition of 4 mg benzalkonium chloride per 100 mL of solution (this would be 3 mL of a benzalkonium chloride 1:750 solution). Albuterol Sulfate 0.5% Inhalant Solution (Preservative Free) Albuterol sulfate Citric acid, anhydrous Sodium chloride Sterile water for inhalation qs 500 mg 100 mg 800 mg 100 mL Beclomethasone Dipropionate 0.042% Nasal Solution (Preservative Free) Beclomethasone dipropionate, monohydrate 42 mg Dextrose 5.4 g Polysorbate 80 1 mL Hydrochloric acid (3% - 5%) Adjust to pH 7 Ethanol, 95% 13 mL 0.9% Sodium chloride solution qs 100 mL Flunisolide 0.025% Inhalation Solution (Preservative Free) Flunisolide 25 mg Ethanol, 95% 2 mL 0.9% Sodium chloride solution qs 100 mL Ipratropium Bromide 0.02% Solution (Preservative Free) Ipratropium bromide 20 mg Citric acid, anhydrous 50 mg 0.9% Sodium chloride solution qs 100 mL Terbutaline 0.1% Inhalant Solution (Preservative Free) Terbutaline sulfate 100 mg Citric acid, anhydrous 100 mg 0.9% Sodium chloride solution qs 100 mL Albuterol-Cromolyn-Betamethasone for Inhalation (Preservative Free) Albuterol sulfate 500 mg Cromolyn sodium 1g Betamethasone sodium phosphate 250 mg Citric acid, anhydrous 100 mg Sodium chloride 800 mg Sterile water for inhalation qs 100 mL Adjust pH to 6.8 - 7.0 Albuterol-Ipratropium for Inhalation (Preservative Free) Albuterol sulfate 100 mg Ipratropium bromide 20 mg Citric acid, anhydrous 50 mg Sterile water for inhalation qs 100 mL International Journal of Pharmaceutical Compounding 455 Vol.4 No.6 November/December 2000