Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
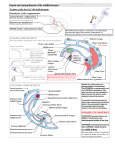
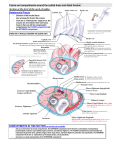
CHRONIC EXERTIONAL COMPARTMENT SYNDROME DR GAVIN SHANG SPORTS PHYSICIAN MBBCH (WITS) MPHIL SPORTS MED (UCT/SSISA) INTRODUCTION • Many muscle groups contained within connective tissue boundaries known as fascia • Fascia separates muscle groups into various compartments • With exercise, muscle blood =low increases and these muscles increase in size and weight • Different etiology compared with traumatic compartment syndrome (medical emergency) CHRONIC EXERTIONAL COMPARTMENT SYNDROME If fascial boundaries are unable to increase accordingly with this change: -‐ pressure in the affected compartment(s) rises -‐ results in pain, parasthesiae, heaviness and tingling -‐ compression on intra-‐compartmental structures (neuro-‐vascular supply) -‐ critical closing pressures of vessels exceeded -‐ decrease venous return and arteriolar =low -‐ insuf=icient perfusion and oxygenation CLINICAL • Inability to perform or continue activity at normal intensity • Asymptomatic at rest • Dull ache (usually anterior, lateral, bilateral) • Subjective tightness, swelling • Associated transient parasthesiae • Worsening with continued training • Typical crescendo-‐decrescendo pain cycle DIFFERENTIAL DIAGNOSES • Bone stress injury / stress fractures • Medial tibial periostalgia • Popliteal artery entrapment • Claudication • Referred pain • Nerve entrapments • DVT CAUSES • -‐ -‐ -‐ -‐ • -‐ -‐ ACUTE: Fracture Muscle trauma Re-‐perfusion syndrome Crush injuries CHRONIC EXERTIONAL: Anabolic steroids Repetitive motion exercises (running, cycling, swimming) LOWER LEG • ANTERIOR COMPARTMENT: Anterior tibial artery Deep peroneal nerve Tibialis anterior, extensor digitorum longus, extensor hallucis longus LOWER LEG • LATERAL COMPARTMENT: Peroneal artery Super=icial peroneal nerve Peroneus longus, peroneus brevis LOWER LEG • SUPERFICIAL POSTERIOR COMPARTMENT: Medial sural cutaneous nerve Medial and lateral gastrocnemius, soleus LOWER LEG • DEEP POSTERIOR COMPARTMENT: Posterior tibial artery Tibial nerve Tibialis posterior, =lexor hallucis longus, =lexor digitorum longus LOWER LEG FOREARM • DORSAL COMPARTMENT: Radial artery, radial recurrent artery, profunda brachii artery, posterior interosseous artery Radial nerve, posterior interosseous nerve Super=icial muscles (brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis, extensor carpi ulnaris) Intermediate muscles (extensor digitorum, extensor digiti minimi) Deep muscles (abductor pollicis longus, extensor pollicis longus, extensor pollicis brevis, extensor indicis, supinator) FOREARM • VOLAR COMPARTMENT: Ulnar artery Median nerve (anterior interosseous nerve) Ulnar nerve (muscular branches) Super=icial muscles (=lexor carpi radialis, palmaris longus, =lexor carpi ulnaris, pronator teres, =lexor digitorum super=icialis) Deep muscles (=lexor digitorum profundus, =lexor policis longus, pronator quadratus) FOREARM METHOD • Compartment Pressure Testing is used to differentiate chronic exertional compartment syndrome from other causes of chronic pain, commonly in lower legs, less frequently in the forearms • Pressure testing of the relevant compartments is performed using Stryker Intra-‐Compartmental Monitoring System METHOD (CONTINUED) • Accurate and consistent technique • Protocol: Resting pressure(s) >15mmHg Post-‐exercise pressure(s) >30mmHg 5minute post-‐exercise pressure(s) >20mmHg LOWER LEG • Anterior: midpoint lower leg, lateral aspect of tibia, directly over tibialis anterior muscle • Lateral: midpoint lower leg, lateral surface of palpated =ibula, directly over peroneal muscles • Super=icial posterior: proximal 1/3 of calf into head of medial or lateral gastrocnemius (depending on which is more symptomatic) • Deep posterior: midpoint lower leg, medial and posterior to medial border of tibia, staying super=icial and into tibialis posterior muscle CONTRAINDICATIONS • Bleeding disorders • Anticoagulant therapy • Malignancy • Systemic illness • Localized in=lammation / infection METHOD (CONTINUED) • Affected areas examined and investigation deemed appropriate • Areas demarcated, cleaned and anaesthetized • Needle catheter inserted into compartments • Baseline measurement of resting pressures • Patient exercised to induce symptoms • Exercise stopped once symptoms clinically signi=icant • Immediate post-‐exercise and up to 5 minutes post-‐exercise pressures measurements recorded COMPLICATIONS • • • -‐ -‐ -‐ -‐ Localized tenderness and/or bruising Subcutaneous and/or intramuscular bleeding EMERGENCY AFTER PROCEDURE (rare): increased swelling parasthesiae sensory loss increasing or unremitting pain MANAGEMENT • Stop aggravating activity • Change activity and decrease intensity • Stretches • Isokinetic testing and de=icit correction • Gait analysis and correction MANAGEMENT • Minimally invasive subcutaneous fasciotomy -‐ high rate of return to previous activity levels