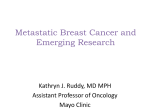
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of Locally Advanced and Metastatic HER2-Positive Breast Cancer Pretest Question #1 Which of the following is an antibody-drug conjugate indicated for use in HER2-positive metastatic breast cancer? A. B. C. D. Trastuzumab JL224 Lapatinib JL225 Ado-trastuzumab emtansine JL226 Pertuzumab JL227 Pretest Question #2 HER2 status must be tested on all newly diagnosed invasive breast cancers. In reviewing your patient’s pathology report, you note that the HER2 status on immunohistochemistry is 2+. What would you recommend? A. Treatment with trastuzumab is indicated JL228 B. Test should be validated by fluorescence in situ hybridization JL229 C. Patient should undergo another biopsy for confirmation JL231 D. None of the above JL232 Management of Locally Advanced and Metastatic HER2-Positive Breast Cancer Melanie Royce, MD, PhD University of New Mexico Comprehensive Cancer Center Karen Herold, DNP, WHCNP-BC, FNP-BC Hoag Memorial Hospital Presbyterian Financial Disclosure § Dr. Royce has received research support from Novartis. § Dr. Herold has no potential conflicts of interest to disclose. Learning Objectives 1. 2. 3. 4. 5. Describe scientific updates and key practice changes in the management of locally advanced and metastatic HER2-positive breast cancer Review HER2 testing guidelines for patients with breast cancer Discuss the best sequencing of FDA-approved targeted agents, mechanism of action, and toxicities Explain the role of neoadjuvant chemotherapy in HER2positive breast cancer, including use of HER2targeted agents Describe collaboration among various members of the health-care team (including but not limited to physician, advanced practitioner, and pharmacist) in management strategies for patients with locally advanced and metastatic HER2-positive breast cancer Breast Cancer Clinical Phenotypes HR (+) 86.5% Breast Cancer Triple (-‐) 15.5% 12.4% HER2 (+) 5.5% Kohler BA, et al. J Natl Cancer Inst. 2015;;107:djv048. FDA-Approved Oncology Drugs Since 2010 Eribulin* Lapatinib1 Pertuzumab* Ado-trastuzumab emtansine* Everolimus* Palbociclib1 http://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm279174.htm. Beyond Trastuzumab: Antibodies Targeting the HER2 Receptor Ado-trastuzumab emtansine [T-DM1] § § HER2-targeted antibody and microtubule inhibitor (emtansine) conjugate Indicated as single agent or in combination with chemo for treatment of metastatic disease after prior trastuzumab therapy or recurrence within 6 months of adjuvant therapy NCCN Clinical Practice Guidelines in Oncology. Breast cancer. v3.2015. http://www.nccn.org. LoRusso PM, et al. Clin Cancer Res. 2011;;17:6437-6447. EMILIA: Phase III Study Design Primary endpoints: Progression-free survival (PFS) by Independent Review Committee, overall survival (OS), and safety Secondary endpoints: Quality of life Treatment continues until disease progression or unmanageable toxicity. Key inclusion criteria: § § Prior treatment to include a taxane and trastuzumab in adjuvant, locally advanced, or metastatic s etting Documented progression of disease during or after treatment for advanced/metastatic disease or within 6 months of c ompleting adjuvant therapy Blackwell KL, et al. J Clin Oncol. 2012;;30 (suppl;; abstract LBA1). EMILIA: PFS, Independent Review Committee Median PFS was 3.2 months longer in the T-DM1 group than in the lapatinib-capecitabine group PFS = progression-free s urvival;; CI = c onfidence interval. Verma S, et al. N Engl J Med. 2012;;367:1783-1791. EMILIA: OS, Second Interim Analysis § 331 deaths;; median follow-up: – – § 18.6 mo (range, 0–41) in the lapatinib-capecitabine group 19.1 mo (range, 0–40) in the T-DM1 group Estimated survival rates, T-DM1 group vs. lapatinib-capecitabine group, respectively: – – 1-year: 85.2% (95% CI, 82.0%–88.5%) v s. 78.4% (95% CI, 74.6%–82.3%) 2 years: 64.7% (95% CI, 59.3%–70.2%) v s. 51.8% (95% CI, 45.9%–57.7%) Verma S, et al. N Engl J Med. 2012;;367:1783-1791. EMILIA: Objective Response Rate and Duration of Response Verma S, et al. N Engl J Med. 2012;;367:1783-1791. EMILIA: Toxicity Profile § Most common grade 3 or 4 toxicity with T-DM1 – – Thrombocytopenia = 12.9%;; first occurrence, in first 2 cycles;; dose modifications à continued treatment Elevated serum [AST] = 4.3% and [ALT] = 2.9% § Three patients in each group had decreased LVEF from baseline to < 40% – Grade 3 LVEF dysfunction: T-DM1 = 1 vs. lapatinib-capecitabine = 0 Verma S, et al. N Engl J Med. 2012;;367:1783-1791. EMILIA: Conclusions § The consistent and favorable outcomes with T-DM1 with regard to the primary and secondary endpoints in the EMILIA trial indicate that this antibody-drug conjugate has efficacy in the treatment of HER2-positive advanced breast cancer. § The adverse events associated with T-DM1 were generally low grade, and patients were largely able to continue treatment after protocol-specified dose modification. § T-DM1 has therapeutic potential, across a heterogeneous population of patients, for the treatment of advanced, HER2-positive breast cancer that has progressed during or after treatment with trastuzumab and a taxane. Verma S, et al. N Engl J Med. 2012;;367:1783-1791. Beyond Trastuzumab: Antibodies Targeting the HER2 Receptor Pertuzumab § Recombinant humanized monoclonal antibody § Targets HER2 extracellular dimerization domain (subdomain II) à blocks ligand-dependent heterodimerization with other HER family members § Indicated in combination with trastuzumab and docetaxel in: 1. Neoadjuvant setting (accelerated approval) 2. Untreated metastatic disease NCCN Clinical Practice Guidelines in Oncology. Breast cancer. v3.2015. http://www.nccn.org. Baselga J, et al. Cancer Res. 2011;;71 (24 suppl;; abstract S5-5). CLEOPATRA: Phase III Study Design § § Randomization was s tratified by geographic region and prior treatment status (neo/adjuvant chemotherapy received or not) Study dosing q3wk: – – – Pertuzumab/placebo: 840-mg loading dose, 430-mg maintenance dose Trastuzumab: 8-mg/kg loading dose, 6-mg/kg maintenance dose Docetaxel: 75 mg/m2, escalating to 100 mg/m2 if tolerated * < 6 c ycles allowed for unacceptable toxicity or progressive disease;; > 6 c ycles allowed at investigator discretion Baselga J, et al. Cancer Res. 2011;;71 (24 suppl;; abstract S5-5). CLEOPATRA: Progression-Free Survival § § Median duration of response: pertuzumab = 20.2 mo (95% CI, 16.0 to 24.0), control = 12.5 mo (95% CI, 10.0 to 15.0) OS rate, pertuzumab vs. c ontrol group ─ ─ ─ ─ 1 year: 94.4% (95% CI, 92.1%–96.7%) v s. 89.0% (95% CI, 85.9%–92.1%) 2 years: 80.5% (95% CI, 76.5%–84.4%) v s. 69.7% (95% CI, 65.0%–74.3%) 3 years: 68.2% (95% CI, 63.4%–72.9%) v s. 54.3% (95% CI, 49.2%–59.4%) 4 years: 57.6% (95% CI, 52.4%–62.7%) v s. 45.4% (95% CI, 40.2%–50.6%) Swain SM, et al. N Engl J Med. 2015;;372:724-734. CLEOPATRA: Overall Survival § § Median OS: pertuzumab group = 56.5 mo (95% CI, 49.3 to not reached), control group = 40.8 mo (95% CI, 35.8–48.3), 15.7 mo longer survival OS rate pertuzumab group vs. c ontrol group: ─ ─ ─ ─ 1 year: 94.4% (95% CI, 92.1%– 96.7%) v s. 89.0% (95% CI, 85.9%–92.1%) 2 years: 80.5% (95% CI, 76.5%–84.4%) v s. 69.7% (95% CI, 65.0%–74.3%) 3 years: 68.2% (95% CI, 63.4%–72.9%) v s. 54.3% (95% CI, 49.2%–59.4%) 4 years: 57.6% (95% CI, 52.4%–62.7%) v s. 45.4% (95% CI, 40.2%–50.6%) Swain SM, et al. N Engl J Med. 2015;;372:724-734. CLEOPATRA: OS, Subgroup Analysis Swain SM, et al. N Engl J Med. 2015;;372:724-734. CLEOPATRA: Toxicity Profile Swain SM, et al. N Engl J Med. 2015;;372:724-734. CLEOPATRA: Conclusions § First-line therapy with pertuzumab, trastuzumab, and docetaxel significantly improved OS in HER2+ metastatic breast cancer – – – – Occurred early and maintained over time Median OS = 56.5 à exceptionally long in this patient population Improvement of 15.7 months extended previous analyses results Majority of adverse events occurred during docetaxel treatment § Treatment with pertuzumab did not increase cardiac toxicity § Important questions remain to be addressed, including biomarkers beyond HER2+ to define who best benefits from combined therapy Swain SM, et al. N Engl J Med. 2015;;372:724-734. NeoSphere: Phase II Study Design § Patients with operable or locally advanced/inflammatory* HER2-positive breast cancer § Chemotherapy naive and primary tumors > 2 cm * Operable = T2-3, N0-1, M0;; locally advanced = T2-3, N2-3, M0 or T4a-c, any N, M0;; inflammatory = T4d, any N, M0 FEC = fluorouracil, epirubicin, and cyclophosphamide. Gianni L, et al. Lancet Oncol. 2012;;13:25-32. NeoSphere: Results § Approximately one-third of patients had locally advanced disease § Pathologic complete response after only 12 weeks of neoadjuvant therapy – THP >>> TH, statistically significant difference – Proportion of HER2-positive tumors (17% of HP, no chemotherapy) can be eradicated without chemotherapy à option for women who cannot receive cytotoxic drugs – One-third of patients did not respond to HP – 6% (25 of 417) had no surgery, mainly due to insufficient therapeutic response à occurred mostly in the chemotherapy-free group (group C) Gianni L, et al. Lancet Oncol. 2012;;13:25-32. NeoSphere: Pathologic Response Gianni L, et al. Lancet Oncol. 2012;;13:25-32. NeoSphere: Results § Toxicity profile – Tolerability of THP similar to conventional TH – Bone-marrow toxicity and febrile neutropenia occurred in all docetaxel-containing groups (A, B, & D) – Cardiac feasibility was good § The randomized, phase III APHINITY trial is evaluating the addition of pertuzumab to the current standard of care chemotherapy + trastuzumab in patients with HER2-positive early-stage breast cancer Gianni L, et al. Lancet Oncol. 2012;;13:25-32. MARIANNE: Phase III Study Design Patients with HER2+ progressive or recurrent locally advanced breast cancer or previously untreated metastatic breast cancer § § § § Primary endpoints: PFS as assessed by IRF;; safety Secondary endpoints: OS;; PFS by investigator: PRO analyses;; biomarkers Superiority design with noninferiority analysis between each of the experimental arms and control arm Interim futility analysis: Option to drop experimental arm Ellis PA, et al. J Clin Oncol. 2015;;33 (suppl;; abstract 507). MARIANNE: Results § None of T-DM1–containing regimen arms significantly improved PFS vs. trastuzumab + taxane chemo à THP remains first-line choice, with T-DM1 preferred 2nd-line option § Benefit with T-DM1 in regard to toxicity and HRQOL outcomes à lower grade 3/4 neutropenia, febrile neutropenia, and diarrhea in T-DM1–containing arms Ellis PA, et al. J Clin Oncol. 2015;;33 (suppl;; abstract 507). Targeting Both HER2 and ER Receptors § Postmenopausal women, hormone receptor–positive metastatic breast cancer § No prior therapy for advanced disease § HER2 status – – – 219 (17%): HER2-positive 952 (74%): HER2-negative 115 (9%): Unconfirmed Johnston S, et al. J Clin Oncol. 2009;;27:5538-5546. EGF30008: Progression-Free Survival § § Median follow-up time = 1.8 years In the HER2+ population, significant reduction in the risk of progression for the combination à median PFS increased from 3.0 to 8.2 months with the addition of lapatinib to letrozole Johnston S, et al. J Clin Oncol. 2009;;27:5538-5546. EGF30008: Overall Survival § Median OS in the HER2-positive population – Letrozole-placebo = 32.3 mo – Letrozole-lapatinib = 33.3 mo – HR = 0.74 (95% CI, 0.5–1.1;; P = .113) Johnston S, et al. J Clin Oncol. 2009;;27:5538-5546. EGF30008: Toxicity Profile § Safety data evaluated in 1,278 protocol-treated patients § Safety profile of lapatinib in this trial was consistent with previous safety data – Most common adverse reactions (≥ 10%) in the lapatinib plus letrozole arm: Diarrhea, rash, nausea, fatigue – Elevated liver enzymes reported in 53% and bilirubin in 22% of patients receiving lapatinib § LVEF decrease in lapatinib + letrozole-treated patients (n = 654) – 26 patients experienced grade 1 or 2 – 6 patients experienced grade 3 or 4 LVEF = left ventricular ejection fraction. Johnston S, et al. J Clin Oncol. 2009;;27:5538-5546. Remember the Good Oldies NCCN. Clinical Practice Guidelines in Oncology. Breast cancer. V3.2015. http://www.nccn.org. NCCN Guidelines: Preferred Agents for Recurrent or Metastatic HER2+ Disease § Preferred first-line agents – Petuzumab + trastuzumab + docetaxel (THP) – Pertuzumab + trastuzumab + paclitaxel § Other first-line agents (trastuzumab alone or with…) – – – – Paclitaxel ± carboplatin Docetaxel Vinorelbine Capecitabine NCCN. Clinical Practice Guidelines in Oncology. Breast cancer.v3.2015. http://www.nccn.org. NCCN Guidelines: Preferred Agents for Recurrent or Metastatic HER2+ Disease (cont) § Preferred agents for trastuzumab-exposed – Ado-trastuzumab emtansine (T-DM1) § Other agents for trastuzumab exposed – – – – Lapatinib + capecitabine Trastuzumab + capecitabine Trastuzumab + lapatinib (without cytotoxic therapy) Trastuzumab + other agents NCCN. Clinical Practice Guidelines in Oncology. Breast cancer. V3.2015. http://www.nccn.org. Case Study Case Study: A.K. § 46-year-old premenopausal Japanese female § Presents to primary care physician with occasional right upper quadrant pain, nausea, and 10-lb unintentional weight loss over past 2 months Case Study: A.K. (cont) § PMHx: Endometriosis § PSHx: Left lumpectomy 2 years ago for stage IIA (T1,N1,M0) infiltrating ductal adenocarcinoma, ER+, PR+, Ki67 = 22%, HER2-positive by IHC 3+, grade 3, SBR 8/9 § Meds: Tamoxifen 20 mg daily § No known allergies § Family history: Mom breast cancer age 48, no other significant family cancer history § GYN Hx: G2P2, menarche at age 12, condoms as birth control, last menstrual period 10 days ago § Social history: Kindergarten teacher, lives with husband and 2 sons A.K.’s Primary Tumor: H&E H&E Courtesy of Hoag Hospital A.K.’s Primary Tumor: ER/PR PR § ER-positive § IHC staining intensity: 80% § PR-positive Courtesy of Hoag Hospital § IHC staining intensity: 50% A.K.’s Primary Tumor: Ki67 and HER2 Ki67 Ki67 = 22%, HER2 = IHC 3+ Courtesy of Hoag Hospital HER2 Applying the 2013 ASCO/CAP Guidelines Giordano SH, et al. J Clin Oncol. 2014;;32:2078-2099. Applying the HER2 ISH Testing Algorithm Giordano SH, et al. J Clin Oncol. 2014;;32:2078-2099. HER2 Status of Breast Cancer Cells Determined by HER2 Testing 1 IHC DETECTS HER2 PROTEIN OVEREXPRESSION IHC 0 IHC 1 + FISH– HER2-‐negative IHC 2 + HER2-‐equivocal ISH DETECTS HER2 GENE AMPLIFICATION HER2-‐negative IHC 3 + FISH+ HER2+ HER2+ The ASCO/CAP HER2 testing guidelines recommend that every case of primary, recurrent, or metastatic breast cancer be evaluated for HER2, estrogen-receptor, and progesterone-receptor status. Wolff AC, et al. J Clin Oncol. 2013;;31:3997-4013. Principles of HER2 Testing Reproduced with permission from the NCCN Clinical Practice G uidelines in Oncology ( NCCN G uidelines ®) for Breast Cancer V.3.2015. © 2015 National Comprehensive Cancer Network, Inc. All r ights r eserved. The NCCN G uidelines ® and illustrations herein may not be reproduced in any form for any purpose without the express written permission of the NCCN. To v iew the most r ecent and c omplete version of the NCCN G uidelines, go online to NCCN.org. National Comprehensive Cancer Network ®, NCCN G uidelines ®, and all other NCCN Content are trademarks owned by the National Comprehensive Cancer Network, Inc. A.K.’s Primary Treatment § Received adjuvant management of chemotherapy with AC followed by T (doxorubicin, cyclophosphamide, paclitaxel) plus trastuzumab § Completed 1 year of adjuvant trastuzumab § Endocrine therapy planned for 5 years with tamoxifen (started when paclitaxel was completed) § Received whole-breast radiation after chemotherapy NCCN Dosing Schedule for HER2+ Disease Reproduced with permission from the NCCN Clinical Practice G uidelines in Oncology ( NCCN G uidelines ®) for Breast Cancer V.3.2015. © 2015 National Comprehensive Cancer Network, Inc. All r ights r eserved. The NCCN G uidelines ® and illustrations herein may not be reproduced in any form for any purpose without the express written permission of the NCCN. To v iew the most r ecent and c omplete version of the NCCN G uidelines, go online to NCCN.org. National Comprehensive Cancer Network ®, NCCN G uidelines ®, and all other NCCN Content are trademarks owned by the National Comprehensive Cancer Network, Inc. Initial Workup for Metastatic Disease § § § § § § § § History and physical exam Complete blood cell count, platelets Liver function tests and alkaline phosphatase PET-CT Chest diagnostic CT Bone scan Liver biopsy Determine tumor ER/PR/HER2 status of metastatic site Recurrent/Stage IV Disease Workup Reproduced with permission from the NCCN Clinical Practice G uidelines in Oncology ( NCCN G uidelines ®) for Breast Cancer V.3.2015. © 2015 National Comprehensive Cancer Network, Inc. All r ights r eserved. The NCCN G uidelines ® and illustrations herein may not be reproduced in any form for any purpose without the express written permission of the NCCN. To v iew the most r ecent and c omplete version of the NCCN G uidelines, go online to NCCN.org. National Comprehensive Cancer Network ®, NCCN G uidelines ®, and all other NCCN Content are trademarks owned by the National Comprehensive Cancer Network, Inc. Workup: PET-CT Contrast-enhanced CT scan showing liver metastasis Courtesy of Hoag Hospital Workup: Bone Scan Courtesy of Hoag Hospital Workup: Genetic Counseling/Testing § A.K.’s mother was diagnosed with breast cancer at age 48, no other family history of cancer § Genetic counseling/testing was recommended at first diagnosis due to patient’s young age and mother’s breast cancer at age 48, but patient declined § At subsequent diagnosis, genetic counseling/testing was recommended;; patient completed BRCAplus testing (Ambry Genetics), with negative results Workup: Liver Biopsy METASTATIC CARCINOMA LIVER Courtesy of Hoag Hospital Workup: Liver Biopsy Courtesy of Hoag Hospital H&E ER PR HER2 A.K.’s Liver Biopsy § PET-CT–confirmed lesion(s) suspicious for metastatic disease § Liver biopsy revealed same profile as primary tumor § Confirmed breast cancer (not new primary) Audience Response Question What is the best treatment option for A.K., who has symptomatic metastatic HER2+/ER+/PR+ breast cancer progression for recurrent disease? A. B. C. D. Single-agent fulvestrant JL233 Lapatinib and letrozole JL234 Pertuzumab, trastuzumab, and docetaxel JL235 Doxorubicin, cyclophosphamide, and paclitaxel JL236 CLEOPATRA Trial: Summary § § § § § Multicenter, randomized, double-blind, placebo-controlled phase III trial in > 800 patients with first line-HER2+ metastatic breast cancer Compared pertuzumab, trastuzumab, and docetaxel with placebo, trastuzumab, and docetaxel Pertuzumab arm–containing regimen significantly prolonged the primary endpoint, PFS, without any increase in cardiac toxic effects Addition of pertuzumab to trastuzumab and docetaxel compared with addition of placebo significantly improved median overall survival to 56.5 months (HR = 0.68, 95% CI 0.56–0.84;; P = .0002) Benefit of pertuzumab-containing regimen on PFS was noted in all protocol-specified subgroups, classified by age, race/ethnicity, geographic region, visceral vs. nonvisceral disease, HR status, use of IHC or FISH to determine HER2 status, and previous exposure to neoadjuvant or adjuvant chemotherapy Swain SM, et al. N Engl J Med. 2015;;372:724-734. Dosing Schedules for HER2-Positive Recurrent or Metastatic Breast Cancer Reproduced with permission from the NCCN Clinical Practice G uidelines in Oncology ( NCCN G uidelines ®) for Breast Cancer V.3.2015. © 2015 National Comprehensive Cancer Network, Inc. All r ights r eserved. The NCCN G uidelines ® and illustrations herein may not be reproduced in any form for any purpose without the express written permission of the NCCN. To v iew the most r ecent and c omplete version of the NCCN G uidelines, go online to NCCN.org. National Comprehensive Cancer Network ®, NCCN G uidelines ®, and all other NCCN Content are trademarks owned by the National Comprehensive Cancer Network, Inc. Audience Response Question Before A.K. begins treatment with pertuzumab, trastuzumab, and docetaxel, additional tests that must be ordered include (choose all that apply): A. Multiple-gated acquisition scan (MUGA) or echocardiogram JL237 B. Beta hCG test JL238 C. Complete blood cell count (CBC) JL239 Audience Response Question Eight days after A.K. receives treatment with her 4th cycle of pertuzumab, trastuzumab, and docetaxel, she develops a low-grade fever. You have a strong index of suspicion for febrile neutropenia because: A. B. C. D. She is at her nadir following treatment JL240 She was previously treated with tamoxifen JL241 She is Asian JL242 She has metastatic liver disease JL243 Pertuzumab Dosing Considerations § Dosing fixed, not based on surface area § Pertuzumab, trastuzumab, and docetaxel should be administered sequentially § Pertuzumab and trastuzumab can be given in any order, but docetaxel should be administered after pertuzumab and trastuzumab § Observation period is important: 60 min after loading dose of pertuzumab and before administering trastuzumab and docetaxel;; 30 min after subsequent infusions of pertuzumab and prior to trastuzumab and docetaxel Genentech. (2015). Perjeta (pertuzumab) package insert. Audience Response Question Three months after A.K. begins treatment with pertuzumab, trastuzumab, and docetaxel, her left ventricular ejection fraction (LVEF) drops from 57% to 38% without any physical findings of congestive heart failure. What do you do? A. Discontinue pertuzumab and trastuzumab and continue with single-agent paclitaxel JL244 B. Continue pertuzumab, trastuzumab, and docetaxel and add an angiotensin-converting enzyme (ACE) inhibitor JL245 C. Hold trastuzumab and pertuzumab and check A.K.’s LVEF in 3 weeks. Restart therapy if LVEF has recovered to > 49%, or if recovered to 45%–49% with a < 10-point difference from baseline of 57% JL246 Cardiac Monitoring § Left ventricular ejection fraction (LVEF) checked at baseline, then every 3 months until treatment completion and then every 6 months for 2 years in adjuvant setting § *Check LVEF at regular intervals in the metastatic setting, usually every 3 months CLEOPATRA Trial Left Ventricular Dysfunction Pertuzumab + trastuzumab + docetaxel (n = 407) Placebo + trastuzumab + docetaxel (n = 397) Left ventricular dysfunction 4.4% 8.3% Symptomatic LVSD (CHF) 1.0% 1.8% Genentech. (2015). Perjeta (pertuzumab) package insert;; Baselga S. N Engl J Med. 2012;; 366:109- 119. Withhold pertuzumab + trastuzumab dosing for at least 3 wk if the patient has: Pertuzumab may be resumed if: A drop in LVEF to less than 40% OR LVEF has recovered to at least 45% OR LVEF of 40% to 45% and the absolute decrease from the pretreatment value is 10 percentage points or more LVEF has recovered to 40% to 45% and the absolute decrease from the pretreatment LVEF is less than 10 percentage points If LVEF has not improved at reassessment at 3 weeks or has declined further, discontinuation of pertuzumab and trastuzumab should be strongly considered, unless the benefits for the individual patient are deemed to outweigh the risks. Most Common Adverse Reactions With Pertuzumab in Combination With Trastuzumab and Doctaxel § § § § Diarrhea: Mild-to-moderate diarrhea usually occurs in first 3 cycles Hydrate aggressively, small meals, avoid irritants like lactose-containing products, loperamide at initial dose of 4 mg followed by 2 mg every 4 hours or after every unformed stool Infusion reactions occur in approximately 10% of patients. Treatment of infusion reaction is clinician choice, most use same premedications used during adjuvant treatment with trastuzumab Febrile neutropenia: Common grade 3/4 adverse reaction, in CLEOPATRA, Asian patients had a higher rate of febrile neutropenia compared with other groups Alopecia, nausea, fatigue, rash, and peripheral neuropathy Genentech. (2015). Perjeta (pertuzumab) package insert;; Baselga S. N Engl J Med. 2012;; 366:109-119. Audience Response Question Six months later, A.K. presents complaining of increasing back pain, and imaging reveals bone metastases in the spine. What is the next best treatment option? A. B. C. D. Capecitabine and lapatinib JL247 Paclitaxel and trastuzumab JL248 Trastuzumab and lapatinib JL249 Single-agent ado-trastuzumab emtansine JL250 Audience Response Question What are the most common side effects that lead to discontinuation of ado-trastuzumab emtansine? A. Neutropenia, peripheral neuropathy JL251 B. Neutropenia, thrombocytopenia JL252 C. Peripheral neuropathy, increased aspartate transaminase JL253 D. Thrombocytopenia, increased aspartate transaminase JL254 Ado-Trastuzumab Emtansine: Recommended Labs § Complete blood cell count (CBC), liver enzymes, and bilirubin at baseline and before each dose (preferably within 72 hours) § Baseline left ventricular ejection fraction (LVEF) and regular monitoring: Recommended every 3 months but clinician to determine frequency of testing based on patient’s history and signs/symptoms § Hemorrhage: Not related to platelet count and there have been deaths;; check other drugs patient is taking, like fish oil Genentech. (2015). Kadcyla (ado-trastuzumab emtansine) package insert. Treatment Options for Metastatic HER2+ Disease § More choices for treatment of HER2+ metastatic breast cancer can result in improved PFS and OS § Development of HER2-targeted agents for the treatment of HER2-positive breast cancer has dramatically improved outcomes for patients with this disease § Understanding the role of HER2 in promoting breast cancer cell growth is a strong foundation for more effective treatments References § § § § § Carver JR. Management of trastuzumab-related cardiac dysfunction. Prog Cardiovasc Dis. 2010;;53:130-139. Giordano SH, Temin S, Kirshner JJ, et al. Systemic therapy for patients with advanced human epidermal growth factor receptor 2-positive breast cancer: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol. 2014;;32:2078-2099. National Comprehensive Cancer Network (NCCN). Clinical Practice Guidelines in Oncology: Breast cancer. v3.2015. http://www.nccn.org. Swain SM, Baselga J, Kim SB, Ro J, et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med. 2015;;372:724-734. Wolff AC, Hammond ME, Hicks, DG, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013;;31:3997-4013. Posttest Question #1 Which of the following is an antibody-drug conjugate indicated for use in HER2-positive metastatic breast cancer? A. B. C. D. Trastuzumab JL255 Lapatinib JL256 Ado-trastuzumab emtansine JL257 Pertuzumab JL258 Posttest Question #2 HER2 status must be tested on all newly diagnosed invasive breast cancers. In reviewing your patient’s pathology report, you note that the HER2 status on immunohistochemistry is 2+. What would you recommend? A. Treatment with trastuzumab is indicated JL259 B. Test should be validated by fluorescence in situ hybridization JL260 C. Patient should undergo another biopsy for confirmation JL261 D. None of the above JL262